Genotypic diversity of multi- and extensively drug-resistant Mycobacterium tuberculosis in Iran: a systematic review and meta-analysis
Mansour Kargarpour Kamakoli, Ehsan Zare BanadKoki, Mehran Nakhaeizadeh, Ava Behrouzi, Nasim Ebrahimifard, Shima Hadifar

TL;DR
This study identifies the most common drug-resistant tuberculosis bacteria types in Iran, which can help improve treatment strategies.
Contribution
The study provides a comprehensive meta-analysis of Mtb genotypes in Iran, highlighting dominant drug-resistant strains.
Findings
Haarlem and Beijing genotypes are the most prevalent among MDR/XDR-TB cases in Iran.
Beijing genotype dominates pre-/XDR-TB cases in Iran.
Local tracking of drug-resistant Mtb is critical for managing TB treatment failure.
Abstract
Monitoring the genetic diversity of the drug-resistant Mycobacterium tuberculosis (Mtb) population contributes to gaining better insight into the bacterial dynamics and informing effective strategies to tackle the challenge of drug resistance. This meta-analysis study investigates the pooled prevalence of Mtb genotypes among Iranian multidrug-resistant (MDR)/extensively drug-resistant (XDR)-TB patients. We performed a systematic search across repositories, including PubMed, Scopus, Web of Science, and Iranian databases, to find studies reporting Mtb genotype prevalence among Iranian MDR/XDR-TB patients through 31 August 2024. Random-effects or fixed-effect models were used to evaluate the pooled proportion. Statistical analysis was conducted using a meta package in R software. In this meta-analysis, 26 out of 34 included studies focused on MDR genotypes, while the remaining studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
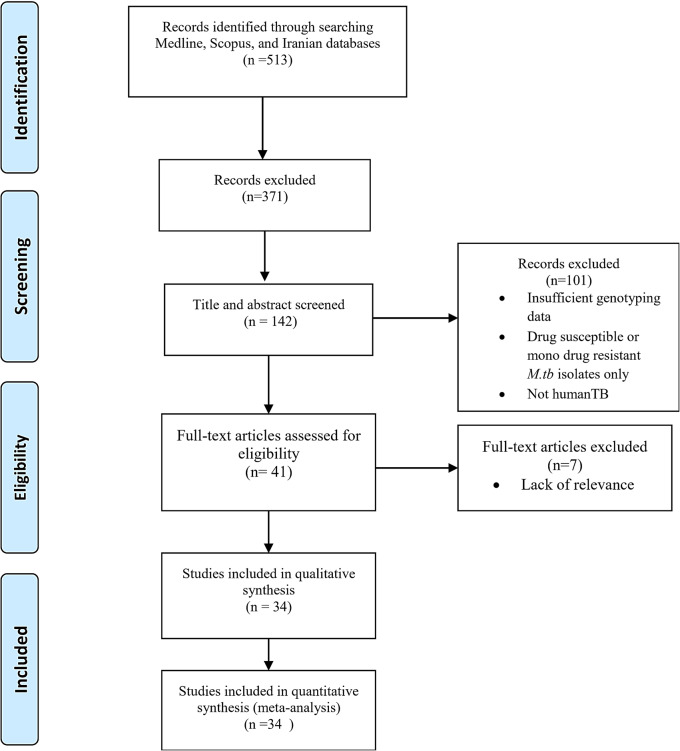 Figure 1
Figure 1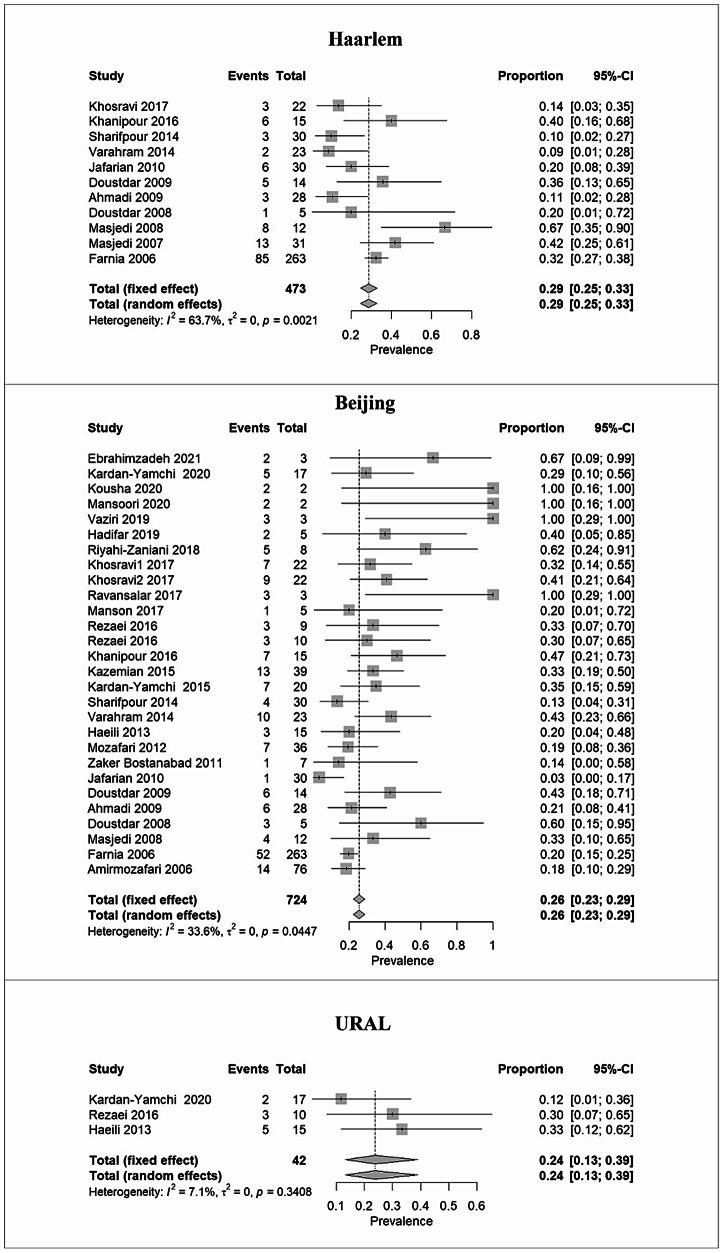 Figure 2
Figure 2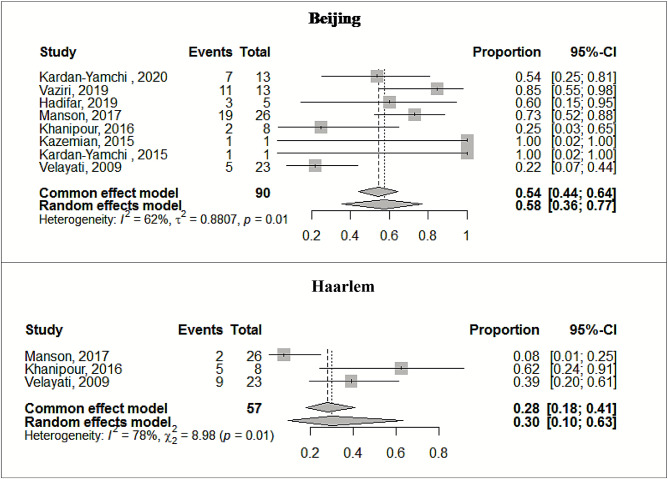 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Mycobacterium research and diagnosis · Diagnosis and treatment of tuberculosis
Introduction
The management and control of tuberculosis (TB), caused by Mycobacterium tuberculosis (Mtb), continue to pose a global health challenge. Despite the global effort, the rate of decrease in TB incidence has been 1.6–2% per year [1]. The ongoing increase in the number of individuals diagnosed with multidrug-resistant (MDR), defined as resistance to at least isoniazid and rifampicin, pre-extensively drug-resistant –TB (pre-XDR), defined as MDR-TB with resistance to a fluoroquinolone, and extensively drug-resistant (XDR)-TB, which is MDR-TB having also resistance to a fluoroquinolone, bedaquiline, and/or linezolid [2], exacerbated the problem, particularly in resource-limited settings [3]. In 2021, the rate of increase in drug-resistant TB (DR-TB) was 6.4%. XDR-TB cases are on the rise, with 13,068 new cases reported across 81 countries. By 2022, the global proportion of MDR/XDR-TB was estimated to be 18%. [1, 4]. Notably, the incidence and mortality rate of DR-TB presented significant geographical heterogeneity [3].
In Iran, situated at the crossroads of high TB burden regions, the pooled prevalence of MDR-TB from 1981 to 2019 was reported at 12.31% and remains a critical concern [5]. This situation is further complicated by the diverse genetic landscape of Mtb strains circulating within the country, which can influence pathobiological properties, control measures, and specific clonal expansion within geographical regions [6–10]. Furthermore, certain populations have documented a relationship between genotype and treatment outcome [11, 12].
In the Iranian population, Beijing and Haarlem genotypes have been identified with notable prevalence among MDR-TB cases [13]. However, the recent increase in the circulation of NEW-1 and CAS genotypes, both known for their potential to acquire drug resistance [14, 15], underscores the necessity of local tracking of DR-Mtb population dynamics to identify specific pathobiological characteristics and also improve the ability to manage local MDR/XDR-TB.
Despite the growing body of research on Mtb epidemiology in Iran, a comprehensive and up-to-date analysis of DR strains diversity, particularly focusing on the genotypes of MDR and XDR Mtb, is lacking.
This systematic review and meta-analysis advances prior reviews, many of which focused on overall MDR-TB prevalence or single genotypes, by synthesizing evidence across studies to provide a consolidated overview of genotypic diversity among MDR- and pre-/XDR-TB cases in Iran.
Methods
The protocol for this systematic review and meta-analysis was registered on the PROSPERO database with the registration number CRD42020223433. The search protocol adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guideline [16] in the current study.
Literature search strategy
A comprehensive literature search was conducted across international and regional databases—including PubMed, Scopus, Web of Science, and Iranian scientific repositories—covering publications up to 31 August 2024. The following terms with the connectors “AND” and “OR” were used for the study searches: “Mycobacterium tuberculosis,” “tuberculosis,” “multidrug resistance,” “MDR,” “XDR,” “drug-resistant,” “molecular typing,” “genetic diversity,” “genotyping, and “Iran”. Persian-language articles were retrieved using the same search strategy with Persian keywords in the relevant Iranian databases. The titles and abstracts of papers selected by our primary search were further examined for full-text review. Moreover, the literature searches were supplemented by checking the reference lists of the collected papers to identify citations not captured in the utilized database. Two authors independently performed the literature searches.
Study selection
Eligible publications were selected based on the following criteria:
- Presented the prevalence of MDR- and/or pre-/XDR-Mtb genotypes; 2) determined the genotypes based on Spoligotyping, mycobacterial interspersed repetitive unit-variable number tandem repeat (MIRU-VNTR) typing, IS6110-RFLP, and Whole Genome Sequencing (WGS) methods; 3) provided clear data on genotype frequencies; and 4) reported data from Iran.
We excluded studies if they were restricted to reporting the prevalence of drug-susceptible Mtb genotypes. Studies provided incomplete data or failed to present it clearly. Additionally, we excluded studies that were published as case reports, meta-analyses, and systematic reviews, as well as those restricted to reporting the prevalence of a single genotype or animal-adapted members of Mtb and that were not published in English or Persian. In studies with overlapping data, times, and sample collection locations, we prioritized the study that provided the most detailed genotyping information. We did not impose restrictions based on publication date.
It should be noted that the WHO revised the definitions of XDR-TB in 2021. According to the updated definition, XDR-TB refers to a MDR-TB that also shows resistance to a fluoroquinolone and at least one Group A agent (bedaquiline or linezolid). As all pre-/XDR studies included in our meta-analysis predate 2021, XDR-TB in this review was defined according to the pre-2021 WHO definition (an MDR strain with additional resistance to a fluoroquinolone and at least one of the injectable agents, amikacin, kanamycin, or capreomycin). We retained the earlier WHO definitions reported by each study and interpreted the pooled results, acknowledging this shift.
Data extraction and quality assessment
The following data were extracted from the eligible studies:
First author, publication year, study location, typing method, detected Mtb genotypes, prevalence of MDR and pre-/XDR genotypes, sample sizes, and population characteristics (pulmonary/extrapulmonary, nationality) (Table 1). Two independent reviewers extracted the data.Table 1. Characteristics of included studies in this meta-analysisFirst authorLocationYear of publicationTyping methodGenotypesTotal genotypesTotal MDRTotal sampleGenotypesTotal genotypesTotal pre-XDR/XDRTotal sampleType of sampleNationalityBakhtiyariniya[17]Khuzestan202224-MIRUVNTRCAS,NEW1,LAM, EAICAS:4/NEW1:1/LAM:1/EAI:11029----PTBIranianEbrahimzadeh[18]Tehran202124-MIRUVNTRBeijing,CameroonBeijing:2/Cameroon:1350----PTBIranianRamazanzadeh[19]Ardabil, Hamadan, Qazvin, Tabriz and Kurdistan2020SpoligoNEW1,UNEW1:4,U:41247----PTBIranianKardan-Yamchi[20]IRAN2020WGSBeijing, CAS, URAL, LAM, NEW1Beijing:5/CAS:6/URAL:2/LAM:3/NEW1:11735Beijing, LAM, NEW1Beijing:7/LAM:2/NEW1:41335PTB/EPTBIranian/immigrantsKousha[21]East Azerbaijan, Kurdistan, and Kermanshah2020IS6110 RFLPBeijingBeijing:2264----PTBIranianMansoori[22]Golestan2020SpoligoBeijingBeijing:22166----PTBIranianVaziri[23]Tehran2019WGSBeijingBeijing:3338Beijing, CAS, NEW1Beijing:11/CAS:1/NEW1:11338PTBIranianHadifar[24]Tehran201924- loci MIRU-VNTR/SpoligoBeijing, CAS, NEW1Beijing:2/CAS:1/NEW1:25172Beijing, CAS, TBeijing:3/CAS:1/T:15172PTB/EPTBIranianRiyahiZaniani[25]Isfahan201824-MIRUVNTRBeijing, LAM, CASBeijing :5/LAM:2/CAS:1818---PTB/EPTBIranianKhosravi[26]Ahvaz, Shiraz, Gorgan, Kermanshah, Mashhad andQom201712-MIRUVNTRBeijing,NEW1,CAS, LAMBeijing :7/NEW1 :1/CAS:1/LAM:222100---PTBIranianKhosravi[27]Ahvaz, Shiraz, Gorgan, Kermanshah, Mashhad, Kashan, Tehran andQom201712-MIRUVNTRBeijing,Haarlem,Uganda, BovisBeijing :9/Haarlem:3/Uganda :1/Bovis:12288---PTBIranianRavansalar[28]Khorasan201712-MIRUVNTR/SpoligoBeijingBeijing:33140---31PTBIranian/immigrantsManson[29]Global2017WGSBeijing, CAS,T1Beijing:1/CAS:1/T1:3531Beijing,CAS,T1,HaarlemBeijing:19/CAS:1/T1:4/Haarlem:226-IranianRezaei[30]Tehran, Zahedan, Isfahan and Khorasan2016SpoligoBeijing, CAS, NEW1,T1, H37RvBeijing:3/CAS:1/NEW1:1/T1:1/,H37Rv:3923---PTBIranianKhanipour[31]Tehran201624-MIRUVNTR/SpoligoBeijing, CAS, T1, HaarlemBeijing:7/CAS:1/T1:1/Haarlem:61523Beijing, Haarlem,T1Beijing:2/Haarlem:5/T1:1823PTBIranianRezaei[32]Tehran, Zahedan, Isfahan and Khorasan2016SpoligoBeijing, CAS, NEW1,URALBeijing:3/CAS:1/NEW1:3/URAL:31020---PTBIranianZamani[33]Hormozgan201615-MIRU-VNTR/SpoligoT1, MANU2T1:2/MANU2:1338---PTBIranianKazemian[34]Tehran, Mashhad, Kermanshah and Zahedan2015SpoligoBeijing, CAS, NEW1, LAM, T, EAI, MANU2,H37RvBeijing:13/CAS:4/NEW1:9/LAM:3/T:2/EAI:1/MANU2:2/H37Rv:33940BeijingBeijing:1140PTBIranianKardan-Yamchi[35]IRAN2015SpoligoBeijing,CAS, NEW1, LAM, EAI,H37RvBeijing: 7/CAS:2/NEW1:1/LAM:3/EAI:1/H37Rv:42031BeijingBeijing:1131PTBIranianSharifpour[36]Tehran2014SpoligoCAS,Beijing, Haarlem,T1Beijing:4/CAS:3/Haarlem:3/T1:330190---PTBIranianVarahram[37]Tehran2014SpoligoBeijing,CAS,Haarlem, LAM,T, EAI, MANU,UBeijing: 10/CAS:1/Haarlem:2/LAM:1/T:1/EAI:5/MANU:2/U:123151---PTBIranian/immigrantsHaeili[38]Tehran, Alborz, Sistan-Baluchestan, Hormozgan, and Kermanshah2013SpoligoBeijing, CAS, URALBeijing: 3/CAS:1/URAL:515291---PTBIranianMozafari[39]Tehran2012MIRUVNTR/SpoligoBeijingBeijing:736105---PTBIranianZaker Bostanabad[40]Tehran2011SpoligoBeijing, CAS, EAI, UBeijing:1/CAS:2/EAI:3/U:17149---PTBIranianJafarian[41]Tehran201012-MIRUVNTR/SpoligoBeijing,CAS,Haarlem,Uganda,Cameron,Ghana,BovisBeijing:1/CAS:5/Haarlem:6//LAM:4/Uganda:2/Cameron:2/Ghana:1/Bovis:13060---PTBIranian/immigrantsVelayati[42]Tehran2009Spoligo----Beijing,CAS,Haarlem,EAIBeijing:5/CAS:4/Haarlem:9/EAI:52323PTBIranian/immigrantsDoustdar[43]Tehran2009IS6110 RFLP/SpoligotypingBeijing, CAS, EAI, HaarlemBeijing:6/CAS:2/EAI:1/Haarlem:51434---PTBIranianAhmadi[44]Tehran2009SpoligoBeijing, CAS, EAI, Haarlem,T1,UBeijing:6/CAS:7/EAI:8/Haarle:3/T1:2/U:228238---PTBIranian/immigrantsDoustdar[45]Tehran2008SpoligotypingBeijing, CAS, HaarlemBeijing: 3/CAS:1/Haarlem:1530---PTBIranianMasjedi[46]Tehran2008SpoligoBeijing, HaarlemBeijing:4/Haarlem:81265---PTB/EPTBIranian/immigrantsMasjedi[47]Tehran2007IS6110 RFLP/SpoligotypingCAS, Haarlem, EAICAS:2/Haarlem:13/EAI:143131---PTBIranianFarnia[48]Tehran2006SpoligoBeijing, CAS,Haarlem, EAI,X,T1Beijing:52/CAS:32/Haarlem:85/EAI:21/X:12/T1:11263263---PTB/EPTBIranian/immigrantsAmirmozafari[49]Tehran2006SpoligoBeijingBeijing:1476439---PTB/EPTBIranian/immigrantsPTB: Pulmonary Tuberculosis, EPTB: Extrapulmonary Tuberculosis, WGS: Whole-Genome Sequencing, MDR: Multidrug resistant, XDR: Extensively drug-resistant.
Two authors using a modified Newcastle–Ottawa Scale (NOS) independently evaluated the quality of each included study [50]. Evaluation was based on participant selection, design and analysis comparability, and outcome ascertainment. The maximum possible score on this method is nine (categorized as high quality). Low-quality studies were excluded from further analysis.
Statistical analysis
The point estimate and 95% confidence interval (CI) were calculated to determine the prevalence of Mtb genotypes among Iranian MDR/XDR-TB patients. Heterogeneity across the studies was assessed using the I^2^ statistic, with a threshold of ≥ 50%, and the Chi-square test, with a P-value < 0.10, was applied to indicate significant heterogeneity [51]. Random-effects meta-regression was conducted to explore the sources of heterogeneity. The Egger regression asymmetry test was employed to assess potential publication bias, with a significance threshold of 5% [52]. A sensitivity analysis was carried out to evaluate the potential influence of the effect of small sample size study (n < 5 and n < 10) on the overall findings. Finally, the subgroup analyses were conducted by year of publication. All statistical analyses and graphical representations were conducted using the meta package in R (v 4.1.1). A two-sided P-value of ≤ 0.05 was considered statistically significant unless otherwise specified.
Results
Search results and studies’ characteristics
A total of 513 papers were screened, and based on title and abstract, 371 were excluded for being irrelevant or duplicates (Fig. 1). Forty-one studies were eligible for full-text review, of which seven were subsequently excluded based on the criteria. Ultimately, 34 studies were selected to assess the prevalence of Mtb genotypes among Iranian MDR/XDR-TB cases. Of these, eight studies focused on pre-/XDR isolates, while the remaining studies provided data on MDR-TB. The publication year of the reviewed studies among MDR genotypes ranged from 2006 to 2022, whereas the studies on pre-/XDR-TB spanned 2009–2020 (before the 2021 WHO definition update).Fig. 1. Flow diagram of meta-study
All papers included in the systematic review assessing the prevalence of MDR genotypes were cross-sectional studies, with sample sizes ranging from two to 263. For studies investigating the prevalence of pre-/XDR genotypes, the highest sample size was 26. Of the 34 conducted studies, five included both Iranian participants and several immigrants. In both MDR and pre-/XDR groups, spoligotyping and MIRU-VNTR typing were mainly used for genotyping (Table 1). The detailed information regarding the included studies is presented in Table 1.
Prevalence rate of MDR/XDR-Mtb genotypes
Based on the results of the 34 included studies, there were 780 MDR-Mtb genotypes and 90 pre-/XDR-Mtb genotypes. Random or fixed effects meta-analysis results indicated Haarlem as 28.5% (95% CI: 24.6–32.8), Beijing as 25.6% (95% CI: 22.5–28.9), and URAL as 23.8% (95% CI: 13.3–38.9) as the predominant MDR genotypes. MANU, T, and Uganda were identified as Mtb genotypes with the lowest prevalence ( < 8%). More details about the overall prevalence are presented in Table 2.Table 2. The pooled prevalence of MDR/XDR MTBC genotypes in TB patientsTypeLineageGenotypeStudy numbersPooled prevalence of genotypeHeterogeneityPublication biasPrevalence%(Number)(95%CI)%I^2^Qp**-valueBegg’sp-value**Egger’s p-valueMDRL4Haarlem1128.5%135(24.6–32.8)%63.7%27.560.0020.2420.266L2Beijing2825.6%185(22.5–28.9) %33.6%40.630.04470.0650.002L4URAL323.80%10(13.3–38.9)%7.10%2.150.3410.1170.402L4NEW1915.97%23(10.8–22.9)%27.5%11.30.20.4040.091L4H37Rv314.70%10(8.1–25.2)%49.50%3.90.1380.6020.669U314.9%7(7.3–28.1)%48.9%3.910.1410.6020.691L3CAS2113.04%79(10.6–15.9)%11.4%22.580.3090.7150.898L1EAI912.64%55(8.6–26.2)%80.8%41.73 < 0.0010.5310.904L4LAM811.24%19(7.3–16.9)%0%3.950.780.9990.532L4Cameroon29.10%3(3.0–24.7)%46.20%1.860.173--L1MANU37.70%5(3.2–17.2)%18.10%2.40.2950.1170.204L4T96.26%26(4.3–9.0)%63.80%22.10.0050.2110.065L4Uganda25.80%3(1.9–16.4)%0%0.10.747--Bovis23.85%2(1.0–14.1)%0%0.10.823--Pre-/XDRL2Beijing857.60%49(35.8–76.8)%61.50%18.20.0110.7060.728L4Haarlem330.20%16(9.8–63.3)%77.70%90.0110.6020.822L4NEW1219.20%26(8.2–38.7)%48.50%1.90.164--L4T315.40%39(7.1–30.3)%0%0.10.9360.6020.917L3CAS410.5%67(5.1–20.3)%0%2.60.4620.9990.430
Beijing genotype was particularly dominant in pre-/XDR cases (57.6%, 95% CI: 35.8–76.8), followed by Haarlem (30.2%, 95% CI: 9.8–63.3) and NEW1 (19.2%, 95% CI: 8.2–38.7) (Table 2). Notably, CAS was revealed as the genotype with the lowest prevalence in Iranian pre-/XDR-TB cases (10.5%, 95% CI: 5.1–20.3). The forest plots in Figs. 2 and 3 illustrate the prevalence of dominant genotypes in both studied groups, providing a visual representation of the data.Fig. 2. Forest plots illustrate the prevalence of predominant Mtb genotypes among MDR-TB casesFig. 3Forest plots present the prevalence of predominant Mtb genotypes among pre-/XDR-TB cases
Subgroup analysis
The result of year grouping, significant changes were observed for the Beijing (pre-/XDR-TB; p = 0.006) and EAI (MDR-TB; p = 0.027) and genotype. The EAI genotype showed a significant decrease after 2015, whereas the prevalence of Beijing lineage with higher resistance levels (Pre-/XDR) significantly increased during the same period (Table 3). The highest and lowest prevalence of MDR genotypes in the studies that were published before 2015 were related to Haarlem (24.3%, 95% CI: 14.7–37.5) and T (4.94%, 95% CI: 3.1–7.8). In contrast, after 2015, Beijing (40%, 95% CI: 33.1–47.2) and EAI (4.35%; 95% CI: 3.1–7.8) were observed with the highest and lowest prevalence genotypes. Similarly, in pre-/XDR-TB cases, Beijing showed growing prevalence over time (Supplementary file).Table 3. Subgroup analysis of M. tb genotypes by study yearTypeVariablesEstimate (95%CI)P-valueBeijingBefore 2015Ref < 0.001MDRAfter 20150.94 (0.58, 1.30)CASBefore 2015Ref0.558After 20150.15 (−0.36, 0.68)HaarlemBefore 2015Ref0.978After 2015−0.19 (−1.42, 1.38)EAIBefore 2015Ref0.027After 2015−1.84 (−3.47, −0.21)TBefore 2015Ref0.082After 20151.15 (−0.14, 2.45)Pre-/XDRBeijingBefore 2015Ref0.006After 20151.93 (0.55, 3.31)
Publication bias and sensitivity analysis
Several cases in Table 2 showed significant heterogeneity in prevalence across the included studies, as indicated by Q test results (Cochran’s Q p < 0.05; I^2^ > 50%). However, the result of Egger’s linear regression and Begg’s tests showed that publication bias was not statistically significant in this meta-analysis, except for MDR–Beijing (Egger p = 0.002) and a borderline signal for MDR–T (p ≈ 0.065). (Table 2). We conducted a sensitivity analysis with two scenarios: excluding studies with sample sizes less than 5 and then excluding studies with sample sizes less than 10. The results showed no significant difference or substantial impact on the pooled prevalence estimates. These findings are detailed in the supplementary file.
Discussion
M. tuberculosis drug resistance is a major public health issue, jeopardizing WHO‘s End TB goals [53]. Understanding the transmission dynamics of drug-resistant Mtb genotypes and tailoring effective regional control strategies are feasible through targeted molecular surveillance. Accordingly, the current study aimed to provide a comprehensive overview of the diversity and pooled prevalence of MDR and pre-/XDR Mtb genotypes in Iran through a systematic review and meta-analysis.
Our analysis revealed that Haarlem (28.5%, 95% CI: 24.6–32.8), Beijing (25.6%, 95% CI: 22.5–28.9), and URAL (23.8%, 95% CI: 13.3–38.9) were the predominant genotypes in the MDR-TB population, respectively, and among the pre-/XDR-TB cases, the Beijing genotype had the highest frequency (57.6%, 95% CI: 35.8–76.8). The results are broadly consistent with global and regional trends and can contribute to informing local health planning [54, 55].
Studies have shown that Beijing strains are associated with low cure rates, treatment failures, and faster transmission, in addition to their greater capability to develop MDR and XDR. The association of Beijing with drug resistance has been linked to compensatory mutations that mitigate fitness costs, facilitating persistent transmission [56]. Reports from China, India, Russia, and the Middle Eastern countries have repeatedly emphasized that the Beijing genotype is responsible for a significant proportion of MDR/XDR-TB cases [13, 55, 57–60]. In this context, the prominence of Beijing among Iranian pre-/XDR- and MDR-TB populations may signify its historical introduction through migration, particularly cross-border migration from high-burden neighbours (notably Afghanistan and Pakistan), successful local adaptation and clonal expansion, leveraged by its enhanced transmissibility and propensity for accumulating drug resistance mechanisms. However, the hypotheses are plausible; genomic studies are needed to confirm these associations. Further, year grouping identified a significant heterogeneity in Beijing genotype (p < 0.001), whereas the prevalence of this genotype was increasing after 2015 (MDR-TB: 40.0%, pre-/XDR-TB: 65.67%). Based on the increasing prevalence trend of this genotype and its pathogenic capability, local tracking dynamics of drug-resistant Mtb population through molecular characterisation and genomic typing are critical to improving our ability to manage local MDR/XDR-TB.
Haarlem genotype is also a major component of the global MDR-TB landscape, notable for its prevalence in diverse regions [61, 62]. Reports from Iran and neighbouring countries (e.g., Turkey, Pakistan) document this genotype among drug-resistant patients. Additionally, an increase in prevalence of Haarlem from 2% to 70% documented for Afghan immigrants in Iran [14, 63]. The prominence of Haarlem in both MDR and pre-/XDR-TB in our meta-analysis aligns with a previous report [63]from Iran showing the dominating Haarlem genotype in the MDR-TB population. Persistence in the prevalence of Haarlem could potentially reflect its adaptation, transmission and survival capacity, and potential biological advantages under selective drug pressure.
URAL and NEW1 genotypes, which were linked to MDR- and pre-XDR-TB populations with high pooled proportion in our analysis, are not globally distributed. Still, the association of these genotypes with MDR and an increase in their prevalence has garnered considerable attention [14, 64]. Intriguingly, the phylogeography of NEW1 is specific to Iran; however, the pattern of distribution changes remarkably [14]. The high frequency of these genotypes in MDR and XDR cases underscores an emerging health concern in our region.
In the pre-/XDR-TB population, the CAS genotype was less prevalent (10.5%, 95% CI: 5.1–20.3%). From 2004 onward, the proportion of CAS represents a noticeable change in MDR/XDR [65]. Given the predominant presence of the CAS genotype around the Indian Ocean and West Asia, the importation of this strain by people from these regions, combined with its biological capabilities for local adaptation, may justify the presence of this genotype. Other genotypes, such as LAM, T, Cameroon, and EAI, with different proportions, were also observed in our meta-analysis. This high genetic diversity and the variation in the prevalence of MDR/XDR genotypes reflect a combination of numerous factors, including migration patterns, treatment behaviours, methodological differences (e.g., MIRU-VNTR), the biological capabilities of genotypes, and disease control policies. The transition toward all-oral regimens and wider use of bedaquiline and linezolid may influence selection pressures and transmission dynamics; however, causal inferences are beyond the scope of this review.
This study has some limitations; first, small sample sizes in some studies and relatively wide confidence intervals, particularly those focusing on pre-/XDR-TB cases, may have affected the precision of the pooled prevalence estimates and limited generalizability. Second, all pre-/XDR-TB data in this review predate the 2021 WHO revision of definitions; therefore, our estimates reflect prior criteria and may not be fully comparable with data generated under the updated definitions. Third, substantial heterogeneity likely arose from moderators such as geography, age, and nationality, which were not feasible due to incomplete reporting across studies. Finally, as some DR-TB studies reported drug susceptibility patterns without corresponding genotyping, the pooled proportions may not capture the full underlying genotype distribution in Iran.
Conclusion
In conclusion, the results of this study highlighted the significant genotypic diversity within the MDR- and pre-/XDR-TB populations, particularly the high prevalence of Haarlem and Beijing genotypes. The situation of Iran at the crossroads of high TB burden regions, as well as its migrant and refugee population, has created complex conditions for the spread of drug-resistant genotypes. This emphasizes the urgent need for continuous molecular monitoring programs and genotype-informed treatment and control strategies in the country. To enhance treatment effectiveness and better manage the MDR-/XDR-TB epidemic in Iran, it is crucial to improve molecular diagnostic capabilities and integrate methods like 24-locus MIRU-VNTR typing into routine surveillance, strengthening detection and systematic contact tracing, with prioritization of high-risk genotypes to inform targeted interventions.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. Global tuberculosis report 2023. World Health Organ. 2023. https://www.whoint/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2023.
- 2Sarkar R, Lenders L, Wilkinson KA, Wilkinson RJ, Nicol MP. Modern lineages of mycobacterium tuberculosis exhibit lineage-specific patterns of growth and cytokine induction in human monocyte-derived macrophages. 2012.10.1371/journal.pone.0043170 PMC 342089322916219 · doi ↗ · pubmed ↗
- 3Page MJ, Mc Kenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE. The PRISMA, 2020 statement: an updated guideline for reporting systematic reviews. bmj. 2021;372.10.1136/bmj.n 71PMC 800592433782057 · doi ↗ · pubmed ↗
- 4Kousha A, Farajnia S, Ansarin K, Khalili M, Shariat M, Sahebi L. Does the Bacillus Calmette-Guerin vaccine have different protective effects on various strains of tuberculosis? Clin Exp Immunol. 2020.10.1111/cei.13549 PMC 780644533188532 · doi ↗ · pubmed ↗
- 5Vaziri F, Kohl TA, Ghajavand H, Kargarpour Kamakoli M, Merker M, Hadifar S, Khanipour S, Fateh A, Masoumi M, Siadat SD, et al. Genetic diversity of multi- and extensively drug-resistant mycobacterium tuberculosis isolates in the capital of Iran, revealed by whole-genome sequencing. J Clin Microbiol. 2019;57(1).10.1128/JCM.01477-18PMC 632247230404943 · doi ↗ · pubmed ↗
- 6Manson AL, Cohen KA, Abeel T, Desjardins CA, Armstrong DT, Barry CE III, Brand J, Jureen P, Malinga L, Nordenberg D. Genomic analysis of globally diverse mycobacterium tuberculosis strains provides insights into the emergence and spread of multidrug resistance. Nature Genetics. 2017;49(3):395.10.1038/ng.3767 PMC 540276228092681 · doi ↗ · pubmed ↗
- 7Zamani S, Haeili M, Nasiri MJ, Imani Fooladi AA, Javadpour S, Feizabadi MM. Genotyping of mycobacterium tuberculosis isolates from Hormozgan province of Iran based on 15-locus MIRU-VNTR and spoligotyping. Int J Bacteriol. 2016, 2016.10.1155/2016/7146470 PMC 508188027819023 · doi ↗ · pubmed ↗
- 8Varahram M, Farnia P, Nasiri MJ, Karahrudi MA, Dizagie MK, Velayati AA. Association of Mycobacterium tuberculosis lineages with IFN-γ and TNF-α gene polymorphisms among pulmonary tuberculosis patient. Mediterranean J Hematol Infect Dis. 2014;6(1).10.4084/MJHID.2014.015PMC 396572724678392 · doi ↗ · pubmed ↗