Atopic diseases in pediatric population: prematurity and small for gestational age
Yi-Yu Su, Chi-Jen Chen, Mei-Huei Chen, Ching-Chun Lin, Chin-Kan Chan, Wu-Shiun Hsieh, Hsi Chang, Chung-Ming Chen, Hsiu-Chen Lin, Pau-Chung Chen

TL;DR
This study explores how being born prematurely or being small for gestational age affects the risk of atopic diseases like asthma and allergies in children.
Contribution
The study identifies specific associations between prematurity and atopic diseases in a large pediatric cohort, revealing sex-specific differences.
Findings
Premature infants had increased risks of allergic rhinitis and asthma but lower risks of atopic dermatitis.
Small-for-gestational-age status was not associated with atopic diseases in term infants.
Adjustments for demographics and socioeconomic factors confirmed the observed associations.
Abstract
Atopic diseases, including asthma, atopic dermatitis (AD), allergic rhinitis (AR), and food allergy, are significant chronic conditions in the pediatric population. Prematurity and small-for-gestational-age (SGA) status are critical factors influencing long-term health outcomes. This study investigated the associations between prematurity, SGA, and the development of atopic diseases in children using a nationwide longitudinal cohort. We analyzed data from Taiwan’s National Health Insurance Research Database (NHIRD), which includes nearly all residents. The cohort comprised infants born between January 1, 2004, and December 31, 2019, excluding those with early death and multiple births. Premature or SGA infants were designated as study cases, while term, appropriate-for-gestational-age (AGA) infants served as controls. Kaplan-Meier analysis estimated cumulative incidence, and log-rank…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
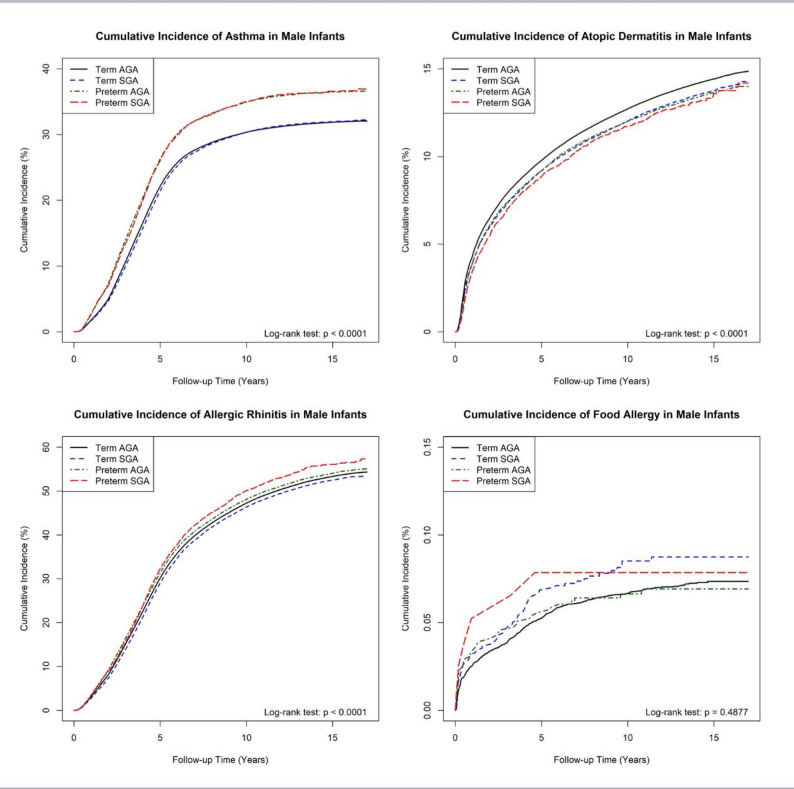 Figure 1
Figure 1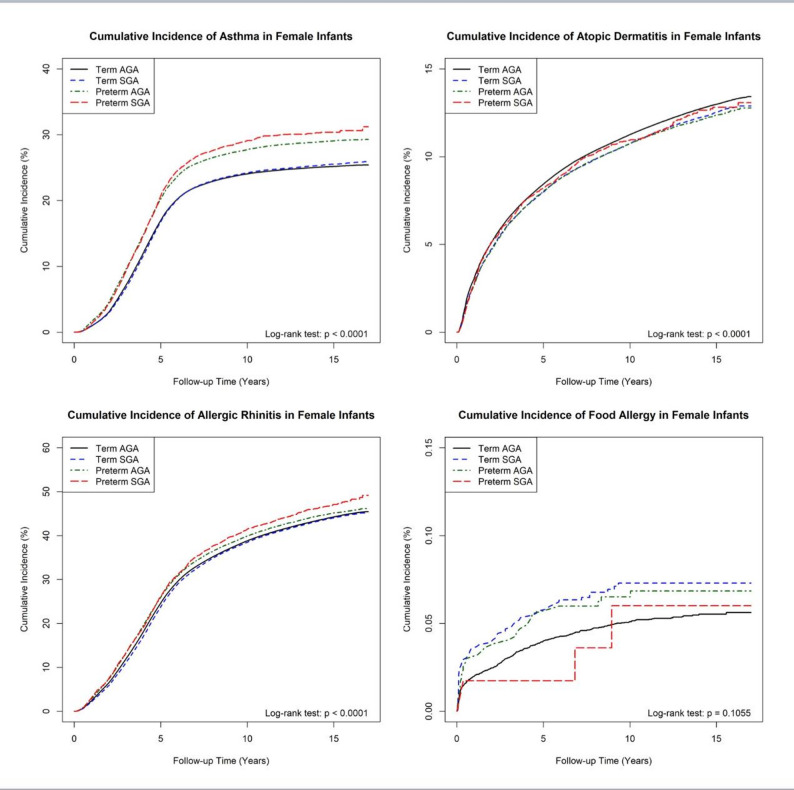 Figure 2
Figure 2- —https://doi.org/10.13039/501100010613Taipei Medical University Hospital
- —https://doi.org/10.13039/100015820Tao Yuan General Hospital, Ministry of Health and Welfare
- —https://doi.org/10.13039/501100004737National Health Research Institutes
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAsthma and respiratory diseases · Birth, Development, and Health · Neonatal Respiratory Health Research
Introduction
Atopic diseases including asthma, atopic dermatitis (AD), allergic rhinitis (AR), and food allergy, are significant chronic conditions in pediatric population and have shown increasing incidence over the past 30 to 40 years [1]. Despite their lifelong impact on patients and the substantial economic burden they place on healthcare systems, prevention strategies and treatable causes for these conditions remain unclear [2]. Early-life exposures, particularly during prenatal and early childhood periods when the immune system is developing, are thought to play a pivotal role in the pathogenesis of atopic diseases [3]. Research in recent decades has revealed that these conditions often follow a time-based progression, beginning with AD and food allergy in infancy, followed by asthma and AR in later childhood [4]. This phenomenon, known as the “atopic march,” is likely driven by shared genetic and environmental risk factors that shape immune responses across different atopic conditions [5]. While the mechanisms underlying this progression remain incompletely understood, certain risk factors appear to be consistently associated with multiple atopic diseases.
Among these risk factors, prematurity and small-for-gestational-age (SGA) status have been increasingly recognized as key determinants of long-term health outcomes, including the development of atopic diseases [6, 7]. The Developmental Origins of Health and Disease (DOHaD) theory suggests that fetal growth patterns and early developmental exposures may predispose individuals to chronic conditions later in life [8]. Studies indicate that preterm or SGA infants may exhibit distinct patterns of atopic disease development compared to their term or appropriate-for-gestational-age (AGA) counterparts. Notably, prematurity has been associated with an increased risk of asthma but a lower risk of AD, suggesting a differential immune trajectory in preterm infants [6, 9, 10]. In contrast, the relationship between SGA and asthma risk remains inconsistent, with studies reporting positive, null, or even inverse associations [11, 12]. These discrepancies may stem from differences in study populations, sample sizes, and definitions of atopic outcomes.
Given these uncertainties, a large-scale, longitudinal analysis is needed to better understand the relationship between prematurity, SGA status, and the development of atopic diseases. Therefore, we conducted a nationwide cohort study to estimate the association between prematurity, SGA status, and the risk of atopic diseases in the pediatric population.
Methods
This study utilized data from Taiwan’s National Health Insurance Research Database (NHIRD), which has collected comprehensive medical records for nearly 23 million residents since 1996 and covers 99.9% of the population [13]. In 2015, the Health and Welfare Data Center (HWDC) of the Ministry of Health and Welfare (MOHW) integrated NHIRD with other health-related databases to establish the Taiwan Maternal and Child Health Database (TMCHD), providing reliable mother-child linkages for perinatal and pediatric research [14].
The study cohort included all live births in Taiwan between January 1, 2004, and December 31, 2019. Multiple births were excluded, and infants who died during follow-up were censored from the analysis. Multiple births were excluded because they significantly increase the risk of both prematurity and being born SGA [15]. Excluding them reduced heterogeneity in perinatal conditions and strengthened the validity of our analyses. Prematurity was defined as birth before 37 weeks of gestation, while SGA was defined as birth weight below the 10th percentile for gestational age, as assessed by healthcare providers. Infants were categorized into four groups based on gestational age and birth weight: term AGA (control group), term SGA, preterm AGA, and preterm SGA. Given the well-documented sex-related differences in growth, metabolism, and atopic disease development, all analyses were performed separately for males and females [16, 17].
Diagnoses of asthma, AD, AR, and food allergy were identified using the International Classification of Diseases (ICD) coding system, including both the Ninth and Tenth Revision Clinical Modification (ICD-9-CM and ICD-10-CM) codes. Asthma (ICD-9: 493, ICD-10: J45), atopic dermatitis (ICD-9: 691.8, ICD-10: L20), allergic rhinitis (ICD-9: 477, ICD-10: J30), and food allergy (ICD-9: 693.1, 995.6, ICD-10: Z91.01) were identified using their respective ICD codes. To ensure diagnostic accuracy, atopic disease diagnoses—including asthma, AD, AR, and food allergy—were confirmed based on the requirement of at least three outpatient visits or one hospital admission.
Covariates included in the analysis were demographics (sex, age), pregnancy-related factors (maternal age, pregnancy complications including gestational hypertension, preeclampsia, and premature rupture of membranes), and complications of prematurity (chronic lung disease, cerebral palsy, hydrocephalus, and necrotizing enterocolitis). Socioeconomic status (SES) was assessed using monthly salary data from NHIRD, categorized into three income brackets: <15,840 New Taiwan Dollars (NTD), 15,841–25,000 NTD, and ≥ 25,001 NTD. These thresholds were selected based on Taiwan’s statutory minimum wage (15,840 NTD) during the study period and an additional cutoff at 25,000 NTD to distinguish middle-income earners from higher-income groups. Urbanization level was classified into four categories (Level I: most urbanized to Level IV: least urbanized), based on residential characteristics including population density, educational attainment, the proportion of elderly residents, agricultural employment rates, and access to healthcare resources [18]. Both socioeconomic status and urbanization level were included as covariates in logistic regression and Cox proportional hazards models to adjust for their potential confounding effects.
Descriptive analyses were performed using univariate and bivariate statistics to summarize baseline characteristics and assess initial associations. Cox proportional hazards models were employed to estimate hazard ratios (HRs) and 95% confidence intervals (CIs), adjusting for all specified covariates. The Kaplan-Meier method was used to estimate the cumulative incidence for each atopic disease, and the log-rank test was applied to compare differences among groups. All statistical analyses were conducted using SAS statistical software (version 9.4; SAS Institute, Cary, NC).
Results
A total of 1,758,460 infants were included in the study, comprising 914,713 males and 843,747 females, born between 2004 and 2019. Infants who died during follow-up were censored, and multiple births were excluded. Table 1 presents the demographic characteristics of the study cohort. The mean gestational age for term AGA infants was 38.6 ± 1 weeks in males and 38.7 ± 1.1 weeks in females, while for term SGA infants, it was 38.8 ± 1 weeks in males and 38.9 ± 1 weeks in females, showing minimal differences from the control group. Preterm AGA infants had a mean gestational age of 34.8 ± 2 weeks in males and 34.8 ± 2.1 weeks in females, whereas preterm SGA infants were born earlier at 34.6 ± 2 weeks in males and 34.5 ± 2.1 weeks in females. Birth weight followed a similar pattern, with term AGA infants having the highest mean birth weights (3192.9 ± 272.8 g in males, 3091.1 ± 265.4 g in females) and preterm SGA infants the lowest (1851.5 ± 404 g in males, 1734.2 ± 401.1 g in females).Table 1. Characteristics of the cohortCharacteristicsTerm AGATerm SGAPreterm AGAPreterm SGAMale n76436981599611047641 Birth gestational age (weeks)38.6 (1)38.8 (1)34.8 (2)34.6 (2) Birth body weight (grams)3192.9 (272.8)2602.2 (206.5)2524.1 (462.1)1851.5 (404)Pregnancy related variables Maternal age30.1 (4.7)29.3 (5)30.4 (5.2)30.7 (5.3) Diabetes5771 (0.76%)516 (0.63%)995 (1.63%)169 (2.21%) Hypertension3546 (0.46%)1006 (1.23%)1093 (1.79%)773 (10.12%) Premature rupture of membranes8698 (1.14%)897 (1.1%)4679 (7.66%)587 (7.68%) Preeclampsia or eclampsia1353 (0.18%)535 (0.66%)862 (1.41%)973 (12.73%) Cesarean section251752 (32.94%)22491 (27.56%)25348 (41.48%)4205 (55.03%)Prematurity complications^†^ All2222 (0.29%)474 (0.58%)1897 (3.1%)412 (5.39%)Other variablesUrbanization level I (highest)218909 (28.64%)21930 (26.88%)16389 (26.82%)2092 (27.38%) II251231 (32.87%)26653 (32.66%)19953 (32.65%)2342 (30.65%) III144135 (18.86%)15549 (19.06%)11672 (19.1%)1496 (19.58%) IV (lowest)150094 (19.64%)17467 (21.41%)13090 (21.42%)1711 (22.39%)Socioeconomic Status: Monthly Salary (NTD) < 1584095779 (12.53%)13270 (16.26%)9746 (15.95%)1346 (17.62%) 15841–25000319467 (41.79%)34334 (42.08%)25641 (41.96%)3040 (39.79%) >=25001349123 (45.67%)33995 (41.66%)25717 (42.09%)3255 (42.60%)Female n71239578864467315757 Birth gestational age (weeks)38.7 (1.1)38.9 (1)34.8 (2.1)34.5 (2.1) Birth body weight (grams)3091.1 (265.4)2524.8 (199)2424.5 (468)1734.2 (401.1)Pregnancy related variables Maternal age30.1 (4.7)29.3 (4.9)30.4 (5.2)30.9 (5.3) Diabetes4925 (0.69%)446 (0.57%)812 (1.74%)120 (2.08%) Hypertension3441 (0.48%)884 (1.12%)1147 (2.45%)704 (12.23%) Premature rupture of membranes7873 (1.11%)805 (1.02%)3740 (8%)354 (6.15%) Preeclampsia or eclampsia1391 (0.2%)575 (0.73%)915 (1.96%)918 (15.95%) Cesarean section226426 (31.78%)20723 (26.28%)20152 (43.12%)3482 (60.48%)Prematurity complications^†^ All1478 (0.2%)356 (0.45%)1350 (2.89%)288 (5%)Other variablesUrbanization level I (highest)204526 (28.71%)21414 (27.15%)12635 (27.04%)1570 (27.27%) II234141 (32.87%)25716 (32.61%)15060 (32.23%)1834 (31.86%) III134177 (18.83%)14921 (18.92%)8947 (19.15%)1073 (18.64%) IV (lowest)139551 (19.59%)16813 (21.32%)10089 (21.59%)1280 (22.23%)Socioeconomic Status: Monthly Salary (NTD) < 1584089488 (12.56%)12480 (15.82%)7969 (17.05%)1051 (18.26%) 15841–25000296481 (41.62%)33444 (42.41%)19385 (41.48%)2277 (39.55%) >=25001326426 (45.82%)32940 (41.77%)19377 (41.46%)2429 (42.19%)† Prematurity complications encompassed chronic lung disease, cerebral palsy, hydrocephalus, and necrotizing enterocolitis
Maternal characteristics varied across groups. Mean maternal age at delivery was similar, but pregnancy-related complications were more prevalent in mothers of preterm infants compared to term AGA controls. Gestational hypertension and preeclampsia were particularly elevated in preterm SGA infants (gestational hypertension: 10.12% in males, 12.23% in females; preeclampsia: 12.73% in males, 15.95% in females), compared to term AGA controls (0.46% in males, 0.48% in females for hypertension; 0.18% in males, 0.2% in females for preeclampsia). Although term SGA infants also had a higher incidence of pregnancy complications than controls, the differences were less pronounced. Cesarean section rates were higher in preterm infants, particularly those born SGA.
Neonatal complications associated with prematurity were most frequent in preterm SGA infants, who had the highest rates of chronic lung disease, cerebral palsy, hydrocephalus, and necrotizing enterocolitis (5.39% in males, 5% in females), followed by preterm AGA infants (3.1% in males, 2.89% in females), term SGA infants (0.58% in males, 0.45% in females), and term AGA controls (0.29% in males, 0.2% in females). Additionally, preterm and SGA infants were more likely to reside in highly urbanized areas and have lower socioeconomic status compared to term AGA infants.
Atopic diseases and risk associations
The incidence of asthma, AD, and AR differed across groups and sexes, as detailed in Tables 2 and 3. Males had higher overall incidence rates of these atopic diseases than females. The average age at diagnosis varied across different atopic diseases and between sexes. Among children who developed each condition, the median age of diagnosis for asthma, allergic rhinitis, atopic dermatitis, and food allergy is summarized by sex in the supplementary table. Prematurity was significantly associated with an increased risk of asthma (HR: 1.19, 95% CI: 1.17–1.21 in males; HR: 1.17, 95% CI: 1.15–1.20 in females) and AR (HR: 1.03, 95% CI: 1.01–1.04 in males; HR: 1.03, 95% CI: 1.02–1.05 in females). In contrast, prematurity was associated with a lower risk of AD (HR: 0.94, 95% CI: 0.92–0.97 in males; HR: 0.95, 95% CI: 0.93–0.98 in females) among AGA infants. Similar patterns were observed in preterm SGA infants, who exhibited increased risks of asthma (HR: 1.17, 95% CI: 1.13–1.22 in males; HR: 1.21, 95% CI: 1.16–1.28 in females) and AR (HR: 1.07, 95% CI: 1.03–1.10 in males; HR: 1.06, 95% CI: 1.02–1.11 in females), but a reduced risk of AD (HR: 0.92, 95% CI: 0.86–0.98 in males; HR: 0.95, 95% CI: 0.88–1.03 in females).Table 2. Allergic diseases in male infants across each groupIncidence (per 10^5^)95%CICrude HR95%CIP valueAdjusted HR^†^95%CIP valueAsthmaTerm AGA3287.83274.4 To 3301.11.00-1.00-Term SGA32743233.3 To 3314.70.990.98 to 1.010.32841.010.99 to 1.020.4624Preterm AGA3947.73894.9 To 4000.51.201.18 to 1.22< 0.00011.191.17 to 1.21< 0.0001Preterm SGA3994.23843 To 4145.51.201.15 to 1.24< 0.00011.161.12 to 1.21< 0.0001Atopic dermatitisTerm AGA1251.81244.1 To 1259.51.00-1.00-Term SGA1180.91158 To 1203.80.950.93 to 0.96< 0.00010.980.96 to 1.000.0181Preterm AGA1173.41147.1 To 1199.80.940.92 to 0.96< 0.00010.940.92 to 0.97< 0.0001Preterm SGA1159.71085.3 To 1234.20.920.86 to 0.980.01070.920.86 to 0.980.0088Allergic rhinitisTerm AGA5971.95952.7 To 5991.11.00-1.00-Term SGA5780.35722.9 To 5837.70.970.96 to 0.98< 0.00010.990.98 to 1.000.1266Preterm AGA6144.36075 To 6213.51.031.02 to 1.04< 0.00011.031.01 to 1.04< 0.0001Preterm SGA6492.76289 To 6696.41.081.05 to 1.12< 0.00011.061.02 to 1.090.0012Food allergyTerm AGA5.95.4 to 6.41.00-1.00-Term SGA7.25.5 to 8.91.210.94 to 1.560.13261.180.91 to 1.510.2119Preterm AGA5.74 to 7.50.980.71 to 1.340.88160.940.68 to 1.300.6888Preterm SGA6.81.4 to 12.31.150.51 to 2.560.73860.950.41 to 2.210.9118† Adjusted for age, pregnancy related variables, prematurity complications and other variables mentioned in Table 1. Table 3Allergic diseases in female infants across each groupIncidence (per 10^5^)95%CICrude HR95%CIP valueAdjusted HR^†^95%CIP valueAsthmaTerm AGA2466.22454.5 To 2477.81.00-1.00-Term SGA2485.62450.4 To 2520.71.010.99 to 1.020.40641.021.00 to 1.030.0492Preterm AGA2938.92888.5 To 2989.41.191.17 to 1.21< 0.00011.171.15 to 1.20< 0.0001Preterm SGA3134.42984.4 To 3284.41.251.19 to 1.31< 0.00011.201.14 to 1.26< 0.0001Atopic dermatitisTerm AGA11011093.6 To 1108.51.00-1.00-Term SGA1051.41029.6 To 1073.30.960.94 to 0.98< 0.00010.990.96 to 1.010.1866Preterm AGA1042.21014 To 1070.40.950.92 to 0.980.00030.950.93 to 0.980.0006Preterm SGA1084.31001.4 To 1167.20.980.90 to 1.050.52890.950.88 to 1.030.2295Allergic rhinitisTerm AGA4577.24560.4 To 45941.00-1.00-Term SGA4510.14460.2 To 45600.980.97 to 1.000.00831.000.99 to 1.020.4855Preterm AGA4751.44684.3 To 4818.61.041.03 to 1.06< 0.00011.031.02 to 1.05< 0.0001Preterm SGA5006.14807.7 To 5204.51.091.05 to 1.13< 0.00011.051.01 to 1.090.0186Food allergyTerm AGA4.54 to 4.91.00-1.00-Term SGA6.14.5 to 7.71.371.04 to 1.820.02721.331.01 to 1.770.0455Preterm AGA5.73.7 to 7.71.280.89 to 1.850.18651.100.75 to 1.610.6160Preterm SGA4.50.9 to 13.31.010.32 to 3.150.98660.730.22 to 2.360.5949† Adjusted for age, pregnancy related variables, prematurity complications and other variables mentioned in Table 1
SGA status in term infants was not associated with increased atopic disease risk. However, in preterm infants, SGA showed a slight but non-significant increase in AR risk compared to preterm AGA infants. Neither prematurity nor SGA was linked to food allergy development during follow-up.
Cumulative incidence of atopic diseases
Figures 1 and 2 present the cumulative incidence curves for atopic diseases across study groups. AD was primarily diagnosed before two years of age, as indicated by the steepest rise in cumulative incidence early in life. Term AGA infants consistently had the highest cumulative incidence of AD throughout the follow-up period.Fig. 1. Cumulative incidence of each atopic disease in male infants. Kaplan-Meier survival curves showing the cumulative incidence of asthma, atopic dermatitis (AD), allergic rhinitis (AR), and food allergy in male infants
Asthma diagnoses peaked between two and five years of age, after which the cumulative incidence curve flattened. Preterm infants had a higher cumulative incidence of asthma than term infants, with the largest gap emerging after age five. Among preterm infants, preterm SGA had the highest cumulative incidence of asthma, followed by preterm AGA, term SGA, and term AGA controls.Fig. 2. Cumulative incidence of each atopic disease in female infants. Kaplan-Meier survival curves showing the cumulative incidence of asthma, atopic dermatitis (AD), allergic rhinitis (AR), and food allergy in female infants
The incidence of AR followed a similar trend, with most diagnoses occurring between two and five years of age. Preterm infants had higher cumulative incidence of AR than term AGA controls, with preterm SGA infants showing the highest risk.
For food allergy, the highest cumulative incidence was observed in term SGA infants, though the small number of cases suggests that this finding should be interpreted with caution.
Discussion
Prematurity and atopic diseases
In this study, prematurity was associated with an increased risk of asthma and AR in childhood but a decreased risk of AD. These findings align with results from other nationwide databases and systematic reviews, which demonstrate a stronger association between prematurity and atopic diseases as gestational age decreases [10, 19–21]. Although the mechanisms underlying prematurity-associated asthma are beyond the scope of this study, multiple contributing factors have been proposed. These include underdeveloped airways, increased antibiotic exposure, heightened susceptibility to viral infections, reduced breastfeeding rates, and an altered gut microbiota [22]. Conversely, the association between prematurity and a lower risk of AD may be linked to increased skin permeability in preterm infants, early antigen exposure in the neonatal intensive care unit, and differences in skin microbiota composition [21]. Preterm infants are born with a thinner stratum corneum and fewer cornified layers; although postnatal skin maturation accelerates after birth, elevated transepidermal water loss often persists until around 34 to 35 weeks of gestation [23]. This compromised skin barrier may lead to earlier and more frequent antigen exposure, potentially inducing immune tolerance through the activation of regulatory T cells and tolerogenic dendritic cells [24]. In contrast, term infants, with a more functionally intact barrier, may encounter environmental antigens later in infancy, which may favor Th2-skewed sensitization and increase the risk of AD. Experimental studies suggest that the timing of antigen exposure is a critical determinant of immune outcomes, with early exposure promoting tolerance and delayed exposure favoring allergic sensitization [25].
The relationship between prematurity and AR remains controversial in the literature. Some studies suggest that prematurity increases AR risk during childhood but may become a protective factor in adulthood [26, 27]. One possible explanation for these inconsistencies is the varying follow-up durations across studies. Atopic diseases often manifest at different stages of childhood, with environmental exposures and immune maturation playing a role in disease development. Over time, medical interventions such as vaccination, inhalers, allergy medications, and immunotherapy, as well as evolving environmental exposures, may modify disease risk. Additionally, asthma and AR share common inflammatory pathways, as evidenced by eosinophilic infiltration in the bronchial mucosa of AR patients, even in the absence of asthma [28]. The “one airway, one disease” concept further supports the close relationship between these two conditions, reinforcing the importance of simultaneous evaluation and treatment [29].
SGA and atopic diseases
SGA status showed no significant association with atopic diseases in term infants, and only a weak, non-significant association with AR in preterm infants. Prior studies examining fetal growth restriction and atopic diseases have reported conflicting results. For example, a large cohort study from Denmark, Sweden, and Finland found that SGA was associated with a slightly increased risk of asthma-related hospitalization in term infants, whereas a UK-based cohort linked prenatal growth faltering to atopic eczema development in infancy [11, 30]. However, these associations were modest despite large sample sizes and were inconsistent with findings from other research [31].
One potential reason for these discrepancies is the heterogeneous nature of SGA. Fetal growth restriction can manifest as asymmetrical intrauterine growth restriction (IUGR)—often caused by extrinsic factors such as placental insufficiency—or symmetrical IUGR, which may result from intrinsic factors such as chromosomal abnormalities or early intrauterine infections. These varying etiologies may influence immune development differently, complicating the relationship between SGA and atopic diseases. Additionally, IUGR infants are frequently born prematurely, often before SGA status can be fully assessed, which may further obscure associations [32].
Maternal complications such as preeclampsia and gestational hypertension, both strongly linked to fetal growth restriction [33, 34], have also been associated with increased atopic disease risk in offspring [35, 36]. In this study, mothers of SGA infants—especially preterm SGA infants—had higher rates of preeclampsia and gestational hypertension, which may have influenced disease risk despite statistical adjustments. Furthermore, maternal atopic history, a key hereditary risk factor for atopic diseases, is often associated with increased risks of both prematurity and fetal growth restriction [37]. This interplay between maternal health, fetal growth, and atopic disease risk suggests that SGA alone may not be a sufficient marker for developmental exposures influencing atopic disease outcomes.
Although prematurity itself is not a modifiable risk factor, several early-life interventions may help mitigate the risk of allergic diseases in this vulnerable population. These include promoting breastfeeding, early and appropriate introduction of complementary foods, enhancement of the skin barrier through regular emollient use in high-risk neonates, and probiotic supplementation [2, 38, 39]. In addition, environmental strategies such as reducing exposure to indoor and outdoor air pollutants may also be beneficial [40]. These approaches align with emerging evidence favoring microbial diversity and immune training over allergen avoidance. Implementing such preventive measures, along with early screening in high-risk groups like preterm infants, may offer meaningful improvements in long-term atopic outcomes.
Strengths and limitations
This study has several strengths. It is the first nationwide cohort study in Taiwan to examine the relationship between preterm birth, SGA status, and atopic diseases, leveraging data from a highly representative healthcare system. The large sample size enhances statistical power, and the robust linkage between maternal and child health records enables a comprehensive analysis of perinatal risk factors. The findings provide valuable insights into early-life risk factors for atopic diseases, supporting the development of prevention and screening strategies.
However, certain limitations should be acknowledged. First, some potential confounders, including the severity of SGA, maternal atopic history, and specific environmental exposures, were not available in the dataset, which may have influenced the observed associations. Although limited maternal health data are accessible, atopic diagnoses in adults often lack consistent information on timing, severity, and clinical progression, which limits their utility in this context. Several other known risk factors for childhood atopic diseases, such as maternal smoking exposure, maternal weight, breastfeeding, and family history of atopy, were not available in the NHIRD and therefore could not be included in the analysis. Although viral infections and antibiotic use may be present in claims data, their ubiquity in infancy and close association with medical care in preterm infants complicate meaningful interpretation. The absence of these variables may contribute to residual confounding and should be addressed in future research using more detailed clinical or cohort datasets. Second, our disease definitions requiring at least three outpatient visits or one hospitalization may underestimate the true incidence, as some mild or self-managed cases, particularly those treated through traditional Chinese medicine or over-the-counter remedies, may not be captured in the claims data. Third, the database does not account for participants’ mobility or activity patterns, limiting our ability to assess actual environmental exposures beyond urbanization level. Lastly, While the study covers the full pediatric period, the follow-up duration may be insufficient to fully capture long-term disease progression, particularly for children born in more recent years who had shorter follow-up time. As a result, we did not perform age-specific incidence analyses or stratification by attained age. Future research should explore the age-dependent effects of prematurity and SGA on the development of atopic diseases, including the potential evolution of risk across childhood in relation to the atopic march. As children grow older, additional environmental exposures and lifestyle factors may further influence the associations between early-life risk factors and atopic outcomes.
Previous studies suggest that maternal fish oil supplementation may reduce early-life allergic sensitization and the severity of AD, though the long-term clinical significance remains uncertain [41, 42]. Given Taiwan’s high seafood consumption and potentially higher omega-3 intake, this may represent an unmeasured confounder. However, based on current evidence, its impact on our results is likely limited.
Conclusion
This study suggests that prematurity is associated with an increased risk of asthma and AR and a reduced risk of AD in Taiwanese children. These findings highlight the need for integrated prevention and early screening strategies tailored to preterm infants. In contrast, SGA was not significantly associated with atopic diseases in term infants, though it may modestly increase the risk of AR in preterm infants. Future research should explore alternative fetal growth indicators, such as the Ponderal Index, to better understand the complex interplay between fetal growth and immune system development. Further investigations are needed to elucidate underlying mechanisms and establish causal relationships between perinatal factors and atopic disease risk. To our knowledge, this is the first large-scale, nationwide cohort study in an Asian population to simultaneously examine prematurity and SGA in relation to multiple atopic outcomes across the pediatric age range. The findings contribute novel insights into early-life risk stratification for allergy prevention in clinical and public health settings.
Supplementary Information
Supplementary Material 1.