Epidemiological Assessment of Benzodiazepine Dependence via Pharmacist-Led EMR Review in Pain and Palliative Care Institution
Carlos Eduardo Estrada-De La Rosa, Felipe Alexis Avalos-Salgado, Daniel Osmar Suárez-Rico, Martin Zermeño-Ruiz, César Ricardo Cortez-Álvarez, Raymundo Escutia-Gutiérrez

TL;DR
Pharmacists analyzing electronic medical records found that nearly 60% of patients in pain and palliative care showed benzodiazepine dependence, with longer use duration being a key risk factor.
Contribution
This study demonstrates the critical role of pharmacists in identifying benzodiazepine dependence through EMR reviews, revealing dependence patterns and risk factors in a high-volume clinical setting.
Findings
59.7% of patients met criteria for benzodiazepine dependence based on EMR review.
Longer duration of benzodiazepine use was the strongest predictor of dependence, not daily dose.
Alprazolam was disproportionately prescribed in higher-dependence categories compared to clonazepam.
Abstract
Background/Objectives: Benzodiazepines (BZDs) are used routinely in cases requiring sedation for anxiety, insomnia, and procedures that require pain management, and daily use of these agents may extend over several months; therefore, monitoring patients is essential to reduce the risk of developing dependence. However, the high patient volume in pain and palliative-care settings often limits physicians’ ability to both conduct consultations and perform comprehensive evaluations. In this context, the pharmacist plays a key role in supporting patient care by contributing professional activities that enhance patient well-being, such as conducting systematic reviews of electronic medical records. This pharmacist-led EMR assessment enables the identification of benzodiazepine dependence patterns and supports a more robust epidemiological evaluation within the institution. Methods: A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
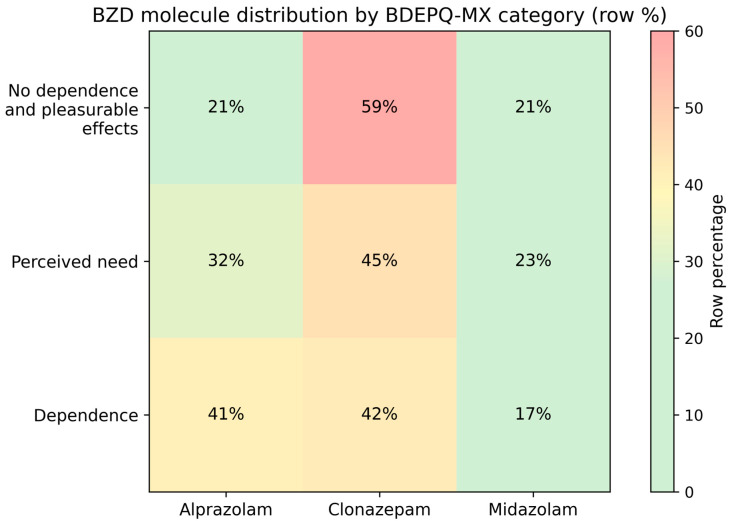 Figure 1
Figure 1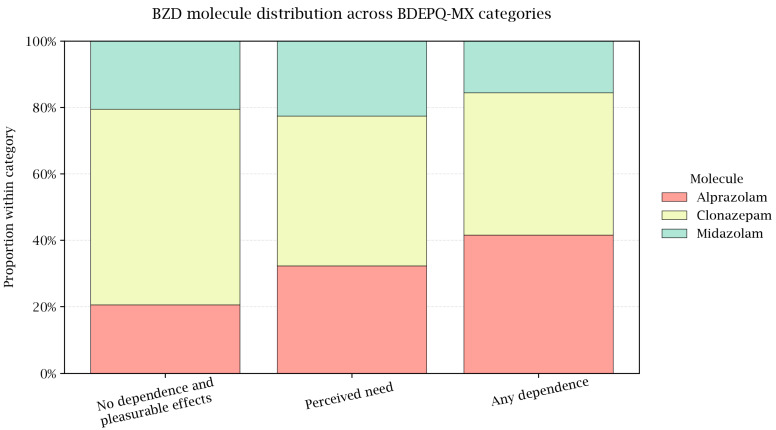 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and related disorders · Opioid Use Disorder Treatment · Pharmaceutical Practices and Patient Outcomes
1. Introduction
Benzodiazepines (BZDs) remain widely prescribed for anxiety and insomnia, yet long-term use is common despite guidance favoring short courses. Prolonged exposure is associated with daytime sedation, psychomotor slowing, cognitive impairment, falls, and clinically significant dependence—especially in older adults and women [1,2]. Real-world studies consistently show higher use in females and late-life patients, frequent chronic use beyond recommended durations, and a preference for a small subset of agents (e.g., alprazolam, lorazepam, clonazepam) [3,4]. In Latin America, population studies similarly document sustained BZD and Z-agent consumption with demographic gradients that align with international trends [5].
Patient perceptions and routine practice patterns help explain the persistence. Qualitative syntheses report that many long-term users view BZDs as essential for daily functioning, minimize or feel resigned to long-term risks, and anticipate physician-led guidance before reducing or stopping; psychological dependence and limited support for tapering further entrench continued use [6,7]. In outpatient samples, self-identified “dependence” often reflects the inability to down-titrate without discomfort, which users distinguish from “addiction/abuse,” complicating risk communication and deprescribing efforts [8]. At the system level, prescribing and dispensing studies highlight gaps in initiation/review processes (e.g., suboptimal documentation of indication and duration, limited planned discontinuation), which correlate with longer exposure and higher dependence risk [9,10].
Accurate measurement of BZD-related dependence phenomena is therefore central to clinical care and epidemiology. The Benzodiazepine Dependence Questionnaire (BDEPQ) was developed to quantify dependence on a continuum across three core dimensions—Perceived need, Pleasant effects, and general Dependence—complementing (but not replacing) the assessment of acute withdrawal [11]. In Mexico, the BDEPQ-MX (Mexican adaptation/validation of the Benzodiazepine Dependence Questionnaire) demonstrated a stable three-factor structure, excellent internal consistency, and strong diagnostic performance versus SCID-I, supporting a pragmatic cut-off for clinical screening in psychiatric outpatients [12]. However, data on BZD dependence in pain relief and palliative-care services—where anxiety, insomnia, and procedural sedation needs are common and daily BZD use may extend over months—remain sparse [13,14,15].
In pain and palliative-care settings, clinicians frequently work under significant time pressure, which limits their ability to conduct the comprehensive monitoring required for safe benzodiazepine use. Evidence shows that many physicians report needing more time than allotted to properly evaluate their patients, and that shortened consultations compromise the detection of treatment-related risks [16,17]. The objective of this study was to assess BZD dependence via an EMR review, which would allow us to demonstrate that, beyond the medical consultation, it is possible to identify and estimate the prevalence of different degrees of benzodiazepine dependence through a systematized review of validated questionnaires applied during medication dispensing. This approach would enable institutions to design strategies to support their patients and to train healthcare personnel accordingly.
2. Materials and Methods
We performed a descriptive observational study of outpatients seen at the Jalisco Institute for Pain Relief and Palliative Care (Zapopan, Mexico) between January 2022 and May 2025. The institute is a state public health facility providing multidisciplinary care for chronic pain and palliative-care patients.
Database elaboration: The questionnaire BDEPQ-MX was administered during BZD agents dispensing by the pharmacists in charge of the service to patients; the indications for which benzodiazepines were prescribed are listed as follows: insomnia, anxiety disorder, affective disorder, mixed anxiety–depressive disorder, and major depressive disorder. No patients in a palliative-care setting requiring these medications were identified at our center. The data were subsequently entered into the patient’s electronic medical record, the “Health Record System” (Sistema de Registro en Salud, SRS). Through a subsequent systematized review of patients with a history of benzodiazepine prescription, we screened consecutive outpatients with an active benzodiazepine (BZD) prescription documented in the electronic medical record (EMR) during the study window.
Inclusion criteria: (i) age ≥ 18 years; (ii) at least one follow-up visit during which the BDEPQ-MX was administered; (iii) available data on BZD drug and daily dose.
Exclusion criteria: (i) missing BDEPQ-MX total score; (ii) incomplete key covariates (sex or age); (iii) documented severe cognitive impairment precluding valid questionnaire completion. Of the screened patients, n = 181 met criteria and formed the analytic sample. For these patients, an Excel database was created using the information collected from the aforementioned electronic and manual records, which was then used for the corresponding analysis.
The BDEPQ-MX was selected because it was validated in Mexican patients with good psychometric performance versus a structured clinical interview; categorical interpretations followed the published validation framework [15]. Evidence from the brief/French adaptation supports stability of the underlying dimensions across settings [14].
Clinical and prescribing data were abstracted from the EMR and prescription registry using a standardized form. Our demographic and clinical covariates were as follows:
- Sex (female/male), age (years), employment (paid employment vs. not), comorbidities (any documented medical comorbidity; coded as present/absent for analyses).
- Primary BZD indication (insomnia; anxiety; affective disorder; mixed anxious–depressive), as recorded in the EMR.
- Prescribed BZD agents included alprazolam, clonazepam, and midazolam, which were the only benzodiazepines available at the institution. In rare instances, some patients were prescribed lorazepam; however, these cases were excluded due to its low frequency of use (n = 3).
- Daily dose (mg/day), taken from the prescription (“mg per 24 h”).
- Duration of BZD use (months), calculated from start date to the index BDEPQ-MX visit.
The BDEPQ-MX yields a total score (continuous) and categorical classifications reflecting the instrument’s four dimensions: No dependence, Pleasurable effects, Perceived need, and Dependence. In our first exploratory analysis, we dichotomized the scores into No dependence (both patients that scored “No dependence” and “Pleasurable effects”) and Any dependence (both patients that scored “Perceived need” and “Dependence”). In our second analysis, we explored differences between the four categories.
For regression analyses, we defined a binary endpoint “any dependence” (Perceived need or Dependence) versus No dependence (“No dependence” and “Pleasurable effects”); the continuous BDEPQ-MX total served as the outcome for the general linear model.
This was the census of eligible patients in the period; no a priori sample size calculation was performed. Missingness for model covariates was low; we used complete-case analysis. Sparse categories for BZD agents were combined into others to avoid quasi-separation.
We summarized continuous variables as mean ± SD and categorical variables as n (%). Group comparisons used the following:
- χ^2^ tests (or Fisher’s exact when appropriate) for categorical variables;
- Student’s t test for two-group comparisons of continuous variables;
- One-way ANOVA for comparisons across > 2 groups, followed by Tukey’s post hoc tests when indicated.
Effect sizes were reported as Cramer’s V (χ^2^) and partial η^2^ (ANOVA). Two multivariable models were specified a priori:
- Logistic regression with any dependence as the dependent variable and the following covariates: age, sex, employment, comorbidity (present/absent), duration of BZD use (months), daily dose (mg/day), and BZD drug. We present adjusted odds ratios (aORs) with 95% CIs.
- General linear model (GLM) with BDEPQ-MX total score as the dependent variable and the same covariates; given the clinical interest, we explored interaction terms (sex × employment, sex × comorbidity, employment × comorbidity, and sex × employment × comorbidity). We report F statistics, p values, and partial η^2^.
Model assumptions were checked: normality/homoscedasticity of residuals for the GLM; linearity of the logit for continuous predictors, influential observations, and multicollinearity (variance inflation factor < 5) for the logistic model. Two-sided α = 0.05 defined statistical significance. Analyses were conducted in SPSS v26 (IBM Corp., Armonk, NY, USA) with cross-checks in Python v3.10, (Python Software Foundation, Beaverton, OR, USA) for reproducibility.
3. Results
During the study period, 181 outpatients completed the BDEPQ-MX. The distribution of BDEPQ-MX categories is shown in Figure 1. Dependence was the most frequent category, followed by No dependence and Perceived need, with Pleasurable effects representing the smallest subgroup (Figure 1). For bivariate comparisons and multivariable models, complete-case analyses comprised 181 patients.
Compared with patients without any dependence, those with any BDEPQ-MX dependence were more often female and had a higher burden of comorbidities (both χ^2^, p < 0.001 and p = 0.006, respectively). Age, employment, and the distribution of clinical indications (insomnia, anxiety, affective, mixed anxious–depressive) did not differ significantly between groups (all p > 0.05). By contrast, duration of BZD use (months) showed a marked difference, with higher intake among those with any dependence (mean ± SD 22.6 ± 11.5 vs. 5.9 ± 4.9; p < 0.001). Daily dose (mg/day) did not differ between groups (p = 0.6). Regarding benzodiazepine medications, alprazolam was more frequent among patients with any dependence (38.9% vs. 20.5%; p = 0.009), whereas clonazepam was less frequent (43.5% vs. 58.9%; p ≈ 0.03); midazolam did not differ (p = 0.6) (Table 1).
3.1. Gradients Across BDEPQ-MX Categories
When the sample was stratified by ordered BDEPQ-MX categories, a clear exposure gradient emerged (Table 2). The proportion of women increased from the No dependence group and Pleasurable effects to Perceived need and Dependence (p < 0.001), and comorbidities became more prevalent across the same gradient (p = 0.015). Age, employment, and primary indication again showed no significant differences (all p > 0.05). The duration of BZD use (months) rose stepwise across categories (p < 0.001), whereas the daily dose did not vary (p = 0.7) (Table 2). Consistent with the two-group comparison, the drug mix shifted toward alprazolam in higher-dependence categories (p = 0.031), with a corresponding decrease in clonazepam (p ≈ 0.02), while midazolam remained similar (p = 0.5). These distributional patterns are visualized in row-percentage heatmap (Figure 2), which together show a higher share of alprazolam within Perceived need and Dependence and a lower share of clonazepam.
3.2. Multivariable Analyses
In the logistic regression for any dependence (Table 3), the male sex was independently associated with lower odds of dependence (aOR 0.29; 95% CI 0.11–0.76; p = 0.013), while the duration of BZD use (months) was strongly and positively associated with dependence (aOR 1.32 per month; 95% CI 1.20–1.45; p < 0.001). Age, employment, comorbidity, and daily dose were not significant predictors in the adjusted model (all p > 0.05).
In the general linear model with the continuous BDEPQ-MX total score as the outcome (Table 4), the duration of BZD use was again the dominant contributor (F = 203.26; p < 0.001; partial η^2^ = 0.545). No main effects were observed for age, daily dose, sex, employment, or comorbidity. Among interaction terms, only the sex × employment × comorbidity interaction reached statistical significance (F = 3.997; p = 0.047), with a small effect size (partial η^2^ = 0.023).
Overall, the results consistently indicate that longer exposure—rather than daily dose or nominal indication—is the key driver of BZP-related dependence phenomena in this outpatient pain and palliative-care population, with a sex effect favoring lower odds among men. Visualizations mirror the tabular contrasts, and multivariable models corroborate the central role of the duration of use.
4. Discussion
In our study, 59.7% of patients showed dependence on BZD agents with a mean use of 22.6 ± 11.5 months. Compared against the general population, BZD dependence levels are lower, between 6.6 and 6.8% [18]; however, in clinical settings where BZD agents are used to treat pain like our population, levels tend to be higher. Voyer P et al. screened BZD dependence levels in older adults in Quebec, observing a more similar prevalence to ours of 43% [19]. In another study performed in Spain in patients who reported using BZD for at least 1 month, De la Cuevas C. and Juan de la Fuente Emilio reported a dependence prevalence of 47% [20]. Only in one study, higher prevalence was reported: Kan C. et al. analyzed outpatient BZD users in the Netherlands, divided by users from the general practice and self-help patients; the first group have a prevalence of dependence of 40%, but in the second group, dependence levels reached up to 97% [21].
Factors associated with dependence we observed in our study were female sex, presence of chronic diseases, and length of usage (months). The female sex has been associated as a risk factor of dependence in other studies [20,22,23]. De la Cuevas C. and Juan de la Fuente Emilio also found that dependence was more prevalent in patients using BZD for more time [20]. Alongside Marriott S. and Tyrer P. also reported that longer therapies were risk factors associated with dependence [24]. An important risk factor commonly reported [25,26] that was not identified in our study was higher BZD dose; this could be due to the fact that all patients in our study were under a regime of a mean dose of 2 mg per day. It must be noted that emotional spectrum was not accounted for in our study as a risk factor, although it has been found to be a risk factor to BZD dependence by Kanopka A et al. which observed that introversion and adverse life events were risk factors [25], or the study performed by Ching-Fang Sun et al., where they observed that depressive disorder along with substance abuse were associated with BZD dependence [27].
The duration we observed in our study is similar to the broader literature. Systematic and cohort analyses identify persistence beyond 4–12 weeks as a key threshold after which dependence, tolerance, and withdrawal become increasingly likely, and a sizable fraction of new users transition to long-term use if treatment is not time-limited [28]. Current geriatric and safety guidelines, therefore, recommend restricting BZD courses to the short term, which can also be observed in our results, where shorter usage terms reflected less dependence prevalence [29].
Our drug-specific pattern—a higher share of alprazolam among dependence categories—has pharmacologic plausibility. Reviews note more severe and rapid-onset withdrawal with alprazolam than with many other BZDs, likely related to its short half-life/high potency and interdose withdrawal, which can reinforce continued use and dose-timing behaviors [30]. Notably, some cohorts link specific BZDs to transitioning into long-term use (e.g., nitrazepam, temazepam, lorazepam, clonazepam), underscoring that drug effects are context-dependent [31]. In our clinic, drug shifting was limited due to having only three BZD agents available at the pharmacy to prescribe.
Methodologically, strengths include the use of a validated instrument (BDEPQ-MX) to quantify dependence dimensions in a real-world population—in this case, patients with sleep and/or emotional disorders [15]—alongside the inclusion of a large number of patients using BZD for almost 2 years. Weaknesses in our study consider the lack of record regarding concomitant drugs used by the patient and low reliability of information due to use of EMR. Methodological limitations include the single-center nature of the study, the descriptive design, which does not allow causal inferences regarding BZD dependence, and the reliance on self-reported data obtained through the BDEPQ-MX questionnaire. Consequently, reporting bias may be present due to stigma, fear, or misunderstanding of the questionnaire items.
5. Conclusions
In this outpatient descriptive observational study conducted in a pain relief and palliative care institute, pharmacist-led BDEPQ-MX screening identified a substantial burden of benzodiazepine (BZD)-related dependence phenomena, with more than half of the evaluated patients meeting dependence criteria. The principal risk factor associated with dependence was the duration of BZD exposure, underscoring the importance of prioritizing treatment duration when assessing the dependence risk in clinical settings. The conduct of this study highlights an area for improvement within healthcare institutions, where the identification of conditions that place patients’ health at risk can be achieved through medical record review. Future research should focus on interventional and deprescribing programs for patients using benzodiazepines, led by pharmacists, thereby promoting the distribution of responsibilities within the multidisciplinary healthcare team.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zetsen S.P.G. Schellekens A.F.A. Paling E.P. Kan C.C. Kessels R.P.C. Cognitive Functioning in Long-Term Benzodiazepine Users Eur. Addict. Res.20222837738110.1159/00052598836041417 · doi ↗ · pubmed ↗
- 2Soyka M. Wild I. Caulet B. Leontiou C. Lugoboni F. Hajak G. Long-Term Use of Benzodiazepines in Chronic Insomnia: A European Perspective Front. Psychiatry 202314121202810.3389/fpsyt.2023.121202837599882 PMC 10433200 · doi ↗ · pubmed ↗
- 3Maumus-Robert S. Jarne-Munoz A. Tournier M. Bégaud B. Pariente A. Trajectories of Benzodiazepine Use among Older Adults from a Concordance-with-Guidelines Perspective: A Nationwide Cohort Study Drugs Aging 20234091993110.1007/s 40266-023-01057-x 37552414 · doi ↗ · pubmed ↗
- 4Pétein C. Spinewine A. Henrard S. Trends in Benzodiazepine Receptor Agonists Use and Associated Factors in the Belgian General Older Population: Analysis of the Belgian Health Interview Survey Data Ther. Adv. Psychopharmacol.2021112045125321101187410.1177/2045125321101187434104414 PMC 8161882 · doi ↗ · pubmed ↗
- 5Freire M.D.B.O. Silva B.G.C.D. Bertoldi A.D. Fontanella A.T. Mengue S.S. Ramos L.R. Tavares N.U.L. Pizzol T.D.S.D. Arrais P.S.D. Farias M.R. Utilização de Benzodiazepínicos Em Idosos Brasileiros: Um Estudo de Base Populacional Rev. Saúde Pública 2022561010.11606/s 1518-8787.202205600374035319670 PMC 8926397 · doi ↗ · pubmed ↗
- 6Kelley C.J. Niznik J.D. Ferreri S.P. Schlusser C. Armistead L.T. Hughes T.D. Henage C.B. Busby-Whitehead J. Roberts E. Patient Perceptions of Opioids and Benzodiazepines and Attitudes Toward Deprescribing Drugs Aging 2023401113112210.1007/s 40266-023-01071-z 37792262 PMC 10768261 · doi ↗ · pubmed ↗
- 7Balon R. Who’s Afraid of Benzodiazepines?Psychother. Psychosom.20229129129410.1159/00052520735679836 · doi ↗ · pubmed ↗
- 8Cooper R.E. Ashman M. Lomani J. Moncrieff J. Guy A. Davies J. Morant N. Horowitz M. “Stabilise-Reduce, Stabilise-Reduce”: A Survey of the Common Practices of Deprescribing Services and Recommendations for Future Services P Lo S ONE 202318 e 028298810.1371/journal.pone.028298836920968 PMC 10016688 · doi ↗ · pubmed ↗