Functional Near-Infrared Spectroscopy (fNIRS) in Objective Audiometry: A Scoping Review and Clinical Perspectives
Tomáš Mimra, Martin Augustynek, Marek Penhaker, Lukáš Klein

TL;DR
This review explores how fNIRS could help assess hearing in infants and others who can't cooperate with traditional tests, but more research is needed before it can replace current methods.
Contribution
The paper provides a scoping review of fNIRS as a potential supplementary method in objective audiometry, highlighting its advantages and limitations.
Findings
fNIRS can detect cortical responses to complex auditory stimuli like speech.
fNIRS is more motion-tolerant than BERA and suitable for pediatric and cochlear implant populations.
Standardized protocols and large-scale validation are needed before fNIRS can replace BERA.
Abstract
Background: The objective assessment of hearing in non-cooperative populations, such as neonates, remains a challenge. While Brainstem Evoked Response Audiometry (BERA) is the gold standard, its sensitivity to motion artifacts necessitates alternatives. Objective: This scoping review maps the current literature on functional near-infrared spectroscopy (fNIRS) as a supplementary method in objective audiometry. Data Synthesis: fNIRS shows potential to detect cortical hemodynamic responses, particularly to complex stimuli like speech, which BERA cannot fully assess. Key advantages include motion tolerance and suitability for pediatric and cochlear implant populations. However, the literature reveals significant heterogeneity in stimulation protocols and data processing. Evidence suggests fNIRS is better suited for assessing higher-level auditory processing rather than replacing BERA for…
Click any figure to enlarge with its caption.
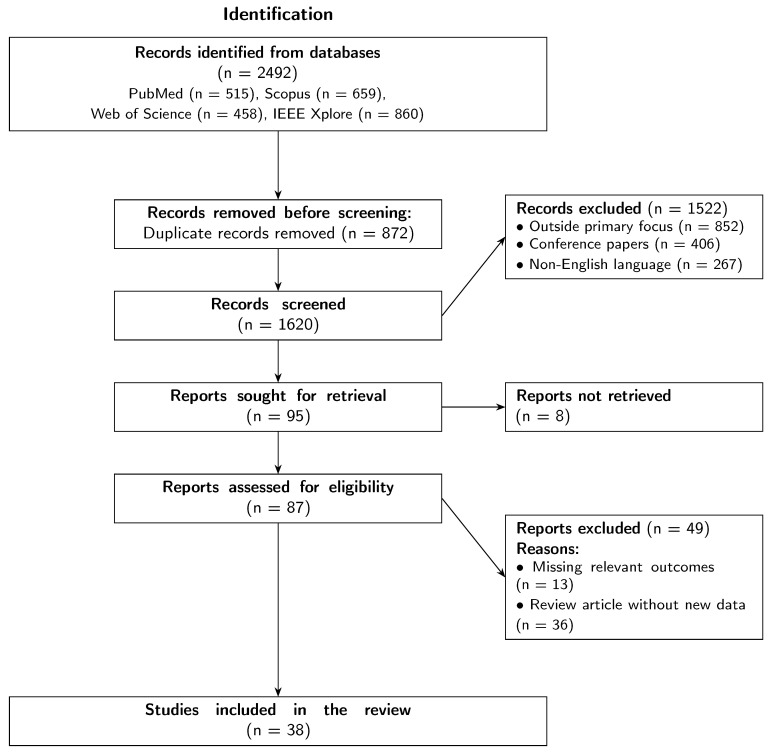 Figure 1
Figure 1- —European Union
- —Biomedical Engineering Systems XXI
- —VSB—Technical University of Ostrava
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOptical Imaging and Spectroscopy Techniques · Photoreceptor and optogenetics research · Neonatal and fetal brain pathology
1. Introduction
Modern clinical audiology faces the persistent challenge of objectively and reliably assessing auditory function. This need is particularly urgent in populations whose ability to cooperate actively is limited, such as neonates, young children, or patients with cognitive or neurological disorders. For decades, the gold standard in this field has been Brainstem Evoked Response Audiometry (BERA), a method based on Electroencephalography (EEG) recording [1]. Despite its established position, BERA suffers from a number of well-documented limitations that significantly reduce its clinical utility and drives the search for more robust alternatives [2].
Among the most significant drawbacks of BERA are its high time consumption (often 30–60 min) [3], a considerable degree of subjectivity in the visual interpretation of results [4,5], and, above all, extreme sensitivity to motion and muscle artifacts. This problem is so fundamental that in uncooperative patients, especially children, it often necessitates performing the examination under sedation or general anesthesia. However, this procedure inevitably carries anesthesiological risks, increases the invasiveness of the procedure, and presents an additional logistical and financial burden [6,7]. These limitations define a clear research gap: the need for an objective, less artifact-sensitive, and more patient-friendly method.
In this context, Functional Near-Infrared Spectroscopy (fNIRS) is an exceptionally promising technology. fNIRS is a non-invasive optical neuroimaging technique that measures changes in the concentration of hemoglobin in the cerebral cortex associated with neural activity. Owing to its non-invasiveness, high tolerance to motion artifacts, and silent operation, fNIRS offers the potential to overcome many of the limitations of BERA [8,9].
While BERA assesses neural integrity at the brainstem level, fNIRS reflects cortical hemodynamic processing. Therefore, this review does not aim to present fNIRS as a direct competitor to BERA in terms of latency precision or threshold estimation, but rather to evaluate its capacity to provide supplementary functional information where BERA is limited.
Although several reviews have addressed fNIRS in specific sub-domains (e.g., solely in cochlear implants or autism), this paper aims to synthesize findings across these fields to provide a holistic view of its potential clinical integration as a complement to standard electrophysiological methods.
The aim of this article is to map and analyze the current state of knowledge on the use of fNIRS in objective audiometry. The paper reviews the theoretical foundations, analyzes key findings from recent studies, and critically discusses the clinical potential, limitations, and future directions.
2. Methodology
This study was conducted as a scoping review to map the available evidence on fNIRS in audiometry. The methodology followed the general principles of the PRISMA 2020 statement [10] for the search and selection process. A comprehensive and systematic search of the PubMed, Scopus, Web of Science, and IEEE Xplore electronic databases was performed in August 2025 to identify relevant studies published between January 2010 and August 2025. The search strategy employed a combination of keywords and Medical Subject Headings (MeSH) terms, where applicable, linked with Boolean operators (AND/OR). The specific search query included the following: ((“functional near-infrared spectroscopy” OR “fNIRS”) AND (“auditory” OR “hearing” OR “audiometry” OR “cochlear implant” OR “hearing aid” OR “auditory evoked potentials” OR “BERA”)).
The initial database search yielded 2492 records, as detailed in the PRISMA flow diagram (Figure 1). The breakdown of these records by database was as follows: PubMed (n = 515), Scopus (n = 659), Web of Science (n = 458), and IEEE Xplore (n = 860). Following the identification phase, all records were imported into a reference management software, and 872 duplicate records were removed. The remaining 1620 unique records underwent a title and abstract screening process conducted independently by two reviewers. The inclusion criteria for this stage were as follows: original research articles, review articles, or meta-analyses published in English that investigated the use of fNIRS for assessing auditory function in human subjects.
Relevant outcomes were defined as follows: (1) detection of significant hemodynamic changes (HbO/HbR) in response to auditory stimuli; (2) correlation of fNIRS responses with behavioral hearing thresholds; (3) identification of biomarkers for cortical plasticity (e.g., lateralization changes).
As shown in Figure 1, a total of 1522 records were excluded during this screening phase because they were outside the primary focus of the review (n = 852), were conference papers without an available full text (n = 406), or were not published in English (n = 267).
Following the initial screening, 95 reports were sought for full-text retrieval to determine eligibility. Of these, 8 reports could not be retrieved, leaving 87 full-text articles for detailed eligibility assessment, as illustrated in the “Eligibility” phase of Figure 1. The same two reviewers independently assessed these articles against the predefined inclusion criteria. Any disagreements between the reviewers at any stage of the selection process were resolved through discussion and consensus, with a third reviewer available for arbitration if necessary. During the full-text assessment, 49 reports were excluded. The primary reasons for exclusion were a lack of relevant outcomes (n = 13) and articles being review papers that did not contribute new data pertinent to this synthesis (n = 36). This rigorous selection process resulted in a final cohort of 38 studies that were included in the review. The entire workflow, from initial identification to final inclusion, is visually represented in Figure 1.
3. Theoretical Foundations of Imaging Methods
To understand the clinical potential of fNIRS in audiometry, it is essential to distinguish between the physiological mechanisms targeted by traditional methods and optical neuroimaging. This section outlines the fundamental operating principles of both electrophysiological and hemodynamic assessments, highlighting how their distinct temporal and spatial characteristics contribute to a more comprehensive evaluation of the auditory pathway.
Complementarity of BERA and fNIRS
Auditory Evoked Potentials (AEP) and BERA provide direct insight into the functional state of the auditory pathway, focusing on early responses (within 10 ms) generated in the brainstem. The result is a characteristic waveform reflecting neural conduction integrity [11,12]. In contrast, fNIRS operates on the principle of neurovascular coupling, measuring hemodynamic changes (HbO/HbR) in the cortex that peak 6–8 s after stimulation [13,14].
The fundamental difference lies in their resolution and scope. BERA offers precise temporal resolution (milliseconds) and vertical localization (brainstem nuclei), whereas fNIRS provides superior spatial resolution of cortical topography. Thus, BERA answers “WHEN” and “IF” the signal reaches the brain, while fNIRS answers “WHERE” and “HOW MUCH” the cortex processes the signal [15]. Their combination provides a comprehensive view of brain function [16]. Table 1 summarizes these differences.
4. Current State of Research: Key Areas and Findings
The literature analysis reveals several key areas where fNIRS demonstrates its potential in audiological research and clinical applications. A summary of studies included in this review is provided in Table 2 and Table 3. It should be noted that these tables exclusively list the original research articles that met the inclusion criteria for data synthesis (n = 38). References cited solely for theoretical background, methodological guidelines, or clinical context are excluded from this summary to strictly focus on the analyzed empirical evidence.
4.1. Demographic Distribution: Adults vs. Pediatric Population
The primary parameter of the analysis is the distribution of studies between adult and pediatric populations. This ratio serves as a critical indicator of the clinical maturity of the method. While adult populations often serve for the validation of principles and normative studies, the pediatric population represents the target demographic for which fNIRS is primarily being developed, largely due to the potential to avoid sedation (Table 4).
Trend Analysis: The data indicates a significant prevalence of studies involving the adult population. A depth analysis of citations reveals that the “Adults” category also includes a specific subgroup of geriatric patients (e.g., [12,17]), where the effects of aging on central auditory processing (Central Presbycusis) are investigated. Pediatric studies are specifically concentrated in two areas: hearing screening in neonates and developmental disorders in older children. This disproportion suggests that while clinical demand is oriented towards children, methodological development is still primarily conducted on adult volunteers.
4.2. Experimental Paradigm: Block Design vs. Event-Related Design
The choice of experimental design is critical in fNIRS due to the slow hemodynamic response (peaking 6–8 s post-stimulus). The analysis of methodologies reveals a clear preference.
Trend Analysis: In contrast to EEG/BERA, where the Event-Related design dominates (to capture ERP waves such as N1, P2), fNIRS shows a clear predominance of Block Design. Citations such as [1,18] illustrate this contrast. While Martin describes “Speech-Evoked Potentials” (Event-Related), fNIRS studies like Bell et al. [19] utilize blocks of continuous speech. This dominance is a direct consequence of the physiology of neurovascular coupling—the metabolic change is too slow to effectively track rapid sequences of short stimuli without signal saturation (Table 5).
4.3. Types of Acoustic Stimuli: Speech vs. Tones vs. Noise
Citation analysis reveals that fNIRS is shifting from simple tone detection to more ecologically valid stimuli (Table 6).
Trend Analysis: The high volume of studies utilizing speech (natural, reversed, or in noise) supports the hypothesis that fNIRS is more suitable for assessing “higher” auditory functions. Studies by Bálint [20] and Mai [17] explicitly utilize “Speech-in-Noise” combinations, which are considered the most sensitive tests in modern audiology for detecting Hidden Hearing Loss and evaluating hearing aid benefits.
4.4. Compensatory Aids: Cochlear Implants (CIs) vs. Hearing Aids (HAs)
This represents one of the most significant categories where fNIRS demonstrates superiority over EEG (Table 7).
Trend Analysis: The data unequivocally indicates that fNIRS is the “technology of choice” for the Cochlear Implant (CI) population. Citations by Chen [21] and Basura [22] are pivotal in this regard. They demonstrate the ability to monitor cortical neuroplasticity with the implant activated, which is practically impossible with other methods (fMRI is often contraindicated or requires magnet explantation; EEG is artifact-ridden).
4.5. Specific Pathologies: Autism and Developmental Disorders
The final category concerns applications in neurodevelopmental disorders, where patient cooperation is limited (Table 8).
Trend Analysis: Although the absolute number of studies is lower, their clinical impact is high. The study by Lai et al. [23] identifies biomarkers (atypical lateralization) that could serve for early diagnosis. The low number of studies reflects the extreme difficulty of recruitment and testing in this specific population, rather than a lack of potential for the method.
4.6. Influence of Stimulation Protocols and Stimulus Types
One of the most crucial findings is that the successful detection of a response using fNIRS is critically dependent on the type and duration of the stimulus. The majority of studies indicate that while short, rapid stimuli like the “clicks” used in BERA are insufficient to elicit a robust hemodynamic response, more complex and longer-lasting stimuli lead to significant and well-detectable results. The hemodynamic response appears to be more sensitive to the complexity and semantic content of the sound. For instance, stimuli such as continuous speech, music, or complex tone sequences reliably evoke detectable hemodynamic changes in the auditory cortex and related association areas [18].
Research further indicates differences in cortical activation depending on stimulus specifics:
- Speech vs. Non-speech Stimuli: Comparing responses to speech (e.g., sentences, words) and acoustically similar but unintelligible sounds (e.g., reversed speech) allows for the isolation of areas specifically involved in language processing. Typically, stronger activation is observed in the left temporal lobe for intelligible speech.
- Frequency and Intensity Dependence: A subset of studies examining responses to pure tones of different frequencies and intensities helps map the tonotopic organization of the auditory cortex and objectively estimate the hearing threshold, albeit with less precision than BERA for rapid changes.
- Listening in Noise: Paradigms where a target stimulus (e.g., speech) is presented against a background of noise are particularly valuable. They allow measurement not only of auditory cortex activation but also the engagement of prefrontal areas, reflecting listening effort and cognitive load.
These findings suggest that fNIRS is better suited for evaluating higher cortical processes associated with sound perception and comprehension than for testing the basic integrity of the auditory pathway.
4.7. Applications in Pediatric Audiology
The strengths of fNIRS are particularly apparent in pediatric applications. Its non-invasiveness and motion tolerance permit the examination of young children without the need for sedation. For example, studies in children with autism spectrum disorders using fNIRS have revealed atypical hemispheric lateralization during speech processing [23]. Innovative approaches even combine fNIRS with virtual acoustic environments to investigate speech understanding in noise in children with hearing aids, offering new insights into neural mechanisms in simulated real-world conditions [19]. Further research utilizes fNIRS for the objective assessment of hearing abilities in newborns and infants, where traditional methods fail or are difficult to perform [24,25].
4.8. Utilization in Cochlear Implant and Hearing Aid Users
fNIRS is becoming a valuable tool for the objective evaluation of the benefits of hearing aids and for investigating central auditory plasticity following hearing loss, both in cochlear implant users and in patients with tinnitus [22]. It allows, for example, for the tracking of cortical neuroplasticity. A study in older adults, most with mild-to-moderate hearing loss, used fNIRS to assess the neuroplasticity of speech-in-noise processing after targeted training. The results showed that neural changes (e.g., reduced response in the left auditory cortex and increased functional connectivity) appeared even before significant behavioral improvement, demonstrating the method’s sensitivity for detecting neuroplastic changes [17].
In the context of cochlear implants (CIs), studies show that patterns of cross-modal reorganization (the engagement of the auditory cortex in processing other senses, e.g., vision, before implantation) can serve as predictors of clinical outcomes after CI placement [21].
Furthermore, fNIRS detects compensatory mechanisms and increased cognitive load during listening in challenging conditions, which helps to optimize implant settings [20,26,27].
Recent literature underscores the critical role of fNIRS in monitoring auditory cortical development. A 2025 review on pediatric audiology highlights that fNIRS is particularly effective in tracking cortical plasticity in children with cochlear implants, identifying biomarkers of cross-modal reorganization that correlate with speech perception outcomes [28]. These findings suggest that fNIRS can serve as a predictor of implantation success by monitoring how the auditory cortex adapts to electrical stimulation over time.
4.9. Multimodal Approaches (fNIRS-EEG)
A growing number of studies are using simultaneous EEG and fNIRS recordings to obtain a more comprehensive picture of auditory processing [16,29]. This approach allows for the correlation of fast electrical responses (e.g., the N1 wave) with slow hemodynamic changes, thus providing a better understanding of the relationship between neural activity and its metabolic impact [18,30]. Multimodal imaging thereby contributes to the identification of more robust biomarkers for neurological and psychiatric disorders [31].
5. Challenges, Limitations, and Future Directions
While the reviewed literature demonstrates the capacity of fNIRS to detect cortical responses to sound, several technical and methodological barriers impede its widespread transition from the research laboratory to routine clinical practice. The following subsections critically examine the quality of the current evidence, identify systemic issues regarding standardization, and outline the necessary steps for future technological development.
5.1. Quality of Evidence and Study Heterogeneity
While the reviewed studies highlight the potential of fNIRS, it is crucial to interpret these findings with caution. A significant limitation of the current body of literature is the high heterogeneity in study designs, particularly regarding stimulation protocols (block vs. event-related), probe placement, and signal processing pipelines. Many of the included studies report on relatively small sample sizes (n < 20) or lack robust control groups, which may inflate the perceived reliability of fNIRS findings. Furthermore, the absence of standardized reporting for signal-to-noise ratios and artifact rejection methods makes it difficult to assess the true effect sizes across studies.
Unlike previous reviews that focused on isolated clinical populations, this synthesis reveals that the lack of standardized protocols is a systemic issue affecting the entire field of objective audiometry, not limited to specific subgroups. Consequently, statements regarding the “reliability” of fNIRS should be understood in the context of research settings rather than established clinical utility.
5.2. Standardization and Robustness
A major obstacle is the lack of standardized stimulation protocols and analytical procedures. This includes the need for consensus on optimal stimulus parameters (e.g., duration, intensity, inter-stimulus interval), experimental designs (e.g., block versus event-related), and data processing pipelines, particularly for motion artifact correction and statistical analysis [32,33]. To ensure comparability of results between laboratories, a consensus on optimal measurement and data processing parameters is necessary. The fNIRS signal is also susceptible to contamination by motion and physiological artifacts (heartbeat, respiration). Their removal requires advanced signal processing methods, which are crucial for obtaining reliable data. Commonly used techniques include the following:
- Frequency Filtering: Application of a band-pass filter (typically 0.01–0.1 Hz) to remove slow drifts and high-frequency noise, including physiological signals such as heart rate (>0.8 Hz) and respiration (∼0.25 Hz).
- Short-Channel Signal Regression: Modern systems use optodes with a short separation (<1 cm) that primarily measure the signal from superficial tissues (scalp). This signal is subsequently used to “clean” the signal from long channels that measure brain activity, thereby effectively removing systemic physiological interference.
- Blind Source Separation Methods: Advanced algorithms like Independent Component Analysis (ICA) can decompose the signal into individual components, allowing for the identification and removal of those corresponding to artifacts [8,34].
Lack of Direct Comparative Studies: A significant gap in the current literature is the scarcity of studies directly comparing BERA and fNIRS sensitivity within the same patient cohort during a single diagnostic session. Most existing research focuses on validating fNIRS against behavioral thresholds or in isolation, rather than correlating it specifically with brainstem responses. Future research should aim to bridge this gap to establish clinical concordance between these two modalities.
Review Limitations: It should be noted that a significant number of potential studies (n = 264) were excluded due to language barriers (non-English). While this is common in systematic reviews, it may exclude valuable regional data or alternative protocols developed in non-English speaking countries. Future reviews should consider using advanced translation tools to include this “gray literature” for a more global perspective.
In addition to technical and methodological challenges, practical and economic barriers also hinder the wider clinical adoption of fNIRS. The acquisition costs for high-quality fNIRS systems, especially those with high-density optode arrays, are still relatively high and can exceed the price of standard EEG equipment [35]. A key obstacle is also the lack of reimbursement from health insurance providers, as the method is still perceived as experimental in most countries and lacks established billing codes [36]. Lastly, although the measurement itself is comfortable for the patient, the interpretation of complex hemodynamic data requires specialized personnel and time-consuming analysis, placing increased demands on resources and staff training [37].
5.3. Future Directions
Future research will focus on several key areas. Firstly, on the development and validation of robust, ideally automated, algorithms for real-time artifact correction [9,38]. Secondly, on the use of machine learning and artificial intelligence methods for the objective classification of responses, which would reduce subjectivity and accelerate the diagnostic process [39,40,41]. Thirdly, on conducting large-scale clinical validation studies to confirm the diagnostic accuracy of fNIRS in large patient cohorts. Furthermore, other promising directions are emerging:
- Wearable fNIRS Technology: The miniaturization of systems allows for the development of lightweight, portable devices that could monitor auditory processing in the patient’s natural environment (e.g., at home, at school), which would significantly increase the ecological validity of the measurements. However, these wearable systems also introduce challenges related to lower signal-to-noise ratios and the need for more advanced, robust algorithms to handle motion artifacts in unconstrained environments.
- Integration with Other Modalities: Combining fNIRS with other sensors, such as eye-tracking, can provide a more comprehensive view of the cognitive processes associated with listening, such as attention and listening effort.
These innovations promise to move fNIRS from the research laboratory closer to standard clinical practice.
6. Conclusions
This scoping review highlights that functional near-infrared spectroscopy and electroencephalography are not competing but rather complementary methods. While EEG/BERA remains an indispensable tool for the temporally precise assessment of auditory pathway integrity at the brainstem level, fNIRS is emerging as a powerful and viable technique for the objective evaluation of cortical sound processing.
A pivotal finding is that when using appropriately designed, complex, and sufficiently long acoustic stimuli, fNIRS can reliably and robustly capture cortical hemodynamic activity. Its key advantages—non-invasiveness, tolerance to motion, and silent operation—make it eminently suitable for clinical use in situations where traditional methods like BERA fail or are difficult to perform. This is particularly true for pediatric audiology, diagnostics in patients with neurodevelopmental disorders, and the objective evaluation of the benefits of hearing aids.
Work in the field is moving towards further standardization, the development of advanced analytical tools, and clinical validation. fNIRS has the potential to become a standard part of the diagnostic arsenal and to contribute to the development of personalized and more precise medicine, not only in audiology but also in related fields such as neurology and developmental psychology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Martin B.A. Tremblay K.L. Korczak P. Speech Evoked Potentials: From the Laboratory to the Clinic Ear Hear.20082928531310.1097/AUD.0b 013e 3181662 c 0e 18453883 · doi ↗ · pubmed ↗
- 2Swami H. Kumar S. Comparison of frequency-Specific hearing thresholds between pure-tone audiometry and auditory steady-state response Indian J. Otol.2019255910.4103/indianjotol.INDIANJOTOL_97_18 · doi ↗
- 3Chawda U. Chaudhari M. Meena M.K. Jha S. A comparative study of OAE (OTO acoustic emission) and BERA (brainstem evoked response audiometry)/ASSR (auditory steady state response) as a screening of hearing loss among the children (<12 years of age) for hearing assessment in ENT OPDIP Indian J. Anat. Surg. Head Neck Brain 2023811511810.18231/j.ijashnb.2022.028 · doi ↗
- 4Karmacharya S. Shrestha B.L. K.C.A.K. Pradhan A. Shrestha A. Ghimire S.B. Comparative study of Automated Auditory Brainstem Response (AABR) and Brainstem Evoked Response Audiometry (BERA) for Hearing Loss Detection in High Risk Infants delivered in Dhulikhel Hospital Janaki Med. Coll. J. Med. Sci.20231161110.3126/jmcjms.v 11i 1.56845 · doi ↗
- 5Ramachandran V. Lewis J.D. Mosstaghimi-Tehrani M. Stach B.A. Yaremchuk K.L. Communication Outcomes in Audiologic Reporting J. Am. Acad. Audiol.20112223124110.3766/jaaa.22.4.621586258 · doi ↗ · pubmed ↗
- 6Elgendy H. Ahmed D. Elmorsy S. Aboloyoun A. Variation of Anesthetic Sedation Requirements in Children Undergoing Auditory Brainstem Response (ABR) Test: A Retrospective Cross-sectional Study J. Anesth. Clin. Res.2016767010.4172/2155-6148.1000670 · doi ↗
- 7Urfali S. Urfali B. Sarac E.T. Koyuncu O. Safety and Complications of Sedation Anesthesia during Pediatric Auditory Brainstem Response Testing ORL 20218418819210.1159/00051715634252904 · doi ↗ · pubmed ↗
- 8Klein F. Optimizing spatial specificity and signal quality in f NIRS: An overview of potential challenges and possible options for improving the reliability of real-time applications Front. Neuroergon.20245128658610.3389/fnrgo.2024.128658638903906 PMC 11188482 · doi ↗ · pubmed ↗