Behçet-like Syndromes: A Comprehensive Review
Gaia Mancuso, Igor Salvadè, Adam Ogna, Brenno Balestra, Helmut Beltraminelli

TL;DR
This review summarizes Behçet-like syndromes, which mimic Behçet’s disease but stem from other conditions like genetic defects or infections, emphasizing the need for accurate diagnosis and treatment.
Contribution
The study compiles and analyzes all published cases of Behçet-like syndromes up to 2024, revealing distinct clinical and genetic patterns that differentiate them from Behçet’s disease.
Findings
Behçet-like syndromes are associated with genetic disorders in 70% of cases and show distinct clinical features like skin lesions and intestinal involvement.
Treatments vary by etiology, with glucocorticoids and anti-TNF biologics being most common, and allogeneic stem cell transplantation used in some myeloproliferative cases.
The study highlights the importance of distinguishing Behçet-like syndromes from Behçet’s disease to guide appropriate therapeutic strategies.
Abstract
Behçet-like syndromes (BLSs) are conditions that present with symptoms similar to Behçet’s disease—such as oral and genital ulcers, fever, skin lesions, joint pain, and intestinal involvement—but arise in association with other underlying disorders. These include monogenic immune defects, myeloproliferative diseases, infections, or reactions to specific medications. Because BLS can resemble Behçet’s disease but requires different treatments, recognizing the underlying cause is essential for proper management. In this review, we summarize all published cases of BLS up to January 2024, highlighting their clinical features, genetic findings, and therapeutic approaches. Understanding BLS as a distinct group of conditions may also provide insights into the mechanisms that drive Behçet’s disease itself. Background: Behçet-like syndrome (BLS) refers to the presence of Behçet’s disease (BD)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
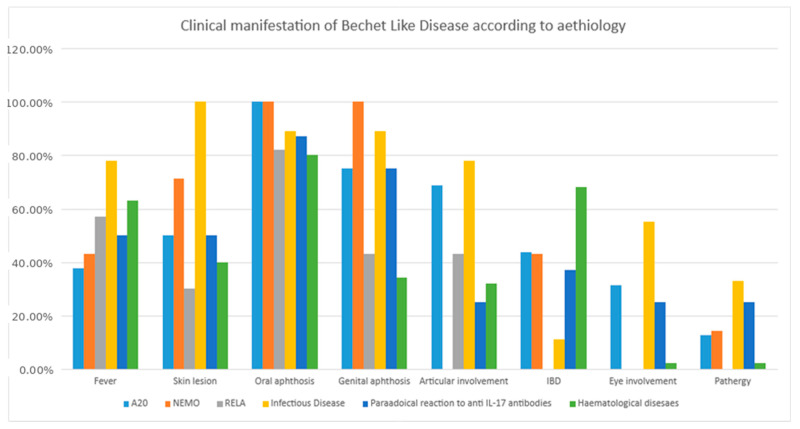 Figure 1
Figure 1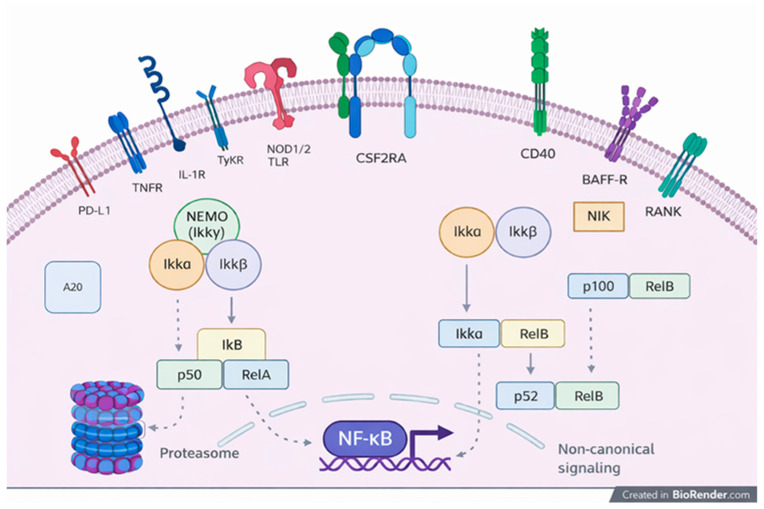 Figure 2
Figure 2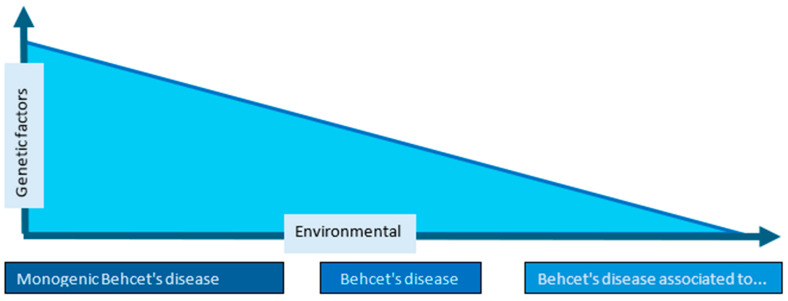 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · Autoimmune and Inflammatory Disorders · Otitis Media and Relapsing Polychondritis
1. Introduction
Behçet-like syndrome (BLS) is defined as the presence of Behçet syndrome features, or Behçet disease (BD), occurring in association with a distinct clinical and/or pathological defined entity, such as various inborn errors of immunity (IEI), including autoinflammatory conditions related to dysregulation of the nuclear factor kappa B (NF-κB) pathway (e.g., TNFAIP3, NFKB1, RELA, IKK gamma mutations) or DADA2, CSF2, and LIG4 mutations [1]. BLS has also been largely described in association with myeloproliferative and myelodysplastic disorders [1,2]. Moreover, some microbial infections, such as Mycobacterium Tuberculosis (MT) and viral infections, can trigger the onset of BLS in genetically susceptible subjects [3]. The development of a BLS has even been reported following drug administration [4].
The clinical symptoms in BLS—such as oral and genital aphthous ulcers, fever, skin lesions, arthralgia/arthritis, ocular inflammation, gastrointestinal ulceration, and vascular involvement—may occur before the onset of the associated diseases [5,6,7] or later on in the disease course [8,9], further expanding the phenotypic spectrum of the associated entities.
BLS does not exhibit specific or pathognomonic histopathological features. As in classical BD, biopsy findings are often nonspecific and may include neutrophilic infiltrates, lymphocytic vasculitis, or ulceration, but none of these patterns reliably distinguish BLS from BD or from other inflammatory or ulcerative conditions. For this reason, the diagnosis of BLS cannot rely on histopathology alone. Instead, it requires the coexistence of Behçet-like clinical manifestations together with a clearly identifiable underlying condition—such as a monogenic autoinflammatory disorder, myelodysplastic syndrome, infection, or drug-related immune dysregulation. Histopathology may support the exclusion of mimickers (e.g., pyoderma gangrenosum, Lipschütz ulcer), but it does not define BLS.
The treatment strategy of BLS differs based on the underlying aetiology: NSAIDs or traditional immunosuppressive therapies frequently fail to relieve the symptoms of BLS [10,11,12,13,14,15,16,17]. Thus, it is essential to distinguish BLS from primary BD in order to ensure appropriate treatment.
This review highlights the clinical characteristics, genetic alterations, and therapeutic approaches of all clinical cases of BLS and associated conditions published up to January 2024, aiming to better define the key features of BLS, particularly those linked to monogenic diseases. Such extensive analysis could enhance our understanding of the pathogenesis of BD and pave the way for further research into its pathophysiology and potential therapeutic targets.
2. Methods
We conducted a literature review of all relevant reports on patients affected by Behçet-like syndrome (BLS) and associated diseases by searching the PubMed, Scopus, and Embase databases in January 2024. The search terms included “Behçet-like syndrome”, “Behçet-like disease”, and “Pseudo-Behçet disease”, with a language restriction to English. We retrieved and reviewed all potentially relevant abstracts and examined the references of the obtained publications to identify additional reports. Non-peer-reviewed reports were excluded. We included only patients with a clearly defined etiological entity and Behçet-like disease, which was defined by the presence of at least two of the International Criteria for Behçet’s Disease (ICBD) [9] and/or a combination of gastrointestinal involvement, oral and/or genital aphthous ulcers, thrombosis, and/or the absence of demonstrated recurrence over time.
We excluded: (1) patients fulfilling full ISG or ICBD criteria for Behçet’s disease (BD) [9]; (2) pediatric cases < 12 years; (3) reports lacking a clearly defined underlying etiology; (4) non-English publications; (5) conference abstracts without sufficient clinical detail. We collected data on sex, age at diagnosis, underlying genetic disorders, clinical manifestations, diagnostic procedures, and treatments. Specifically, we gathered information on the following clinical features: non-infectious fever, skin abnormalities, arthritis, ocular manifestations, gastrointestinal symptoms, peripheral or central neurological involvement, venous or arterial thrombosis, associated diseases, diagnostic procedures, and treatments. Laboratory data were included, when available, encompassing blood counts, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), serum creatine kinase levels, hepatitis C virus (HCV) and HIV serologies, immunological markers (anti-neutrophil cytoplasmic and antinuclear antibodies, cryoglobulinemia), and human leukocyte antigen B51 (HLA-B51) status. We also reviewed endoscopic abnormalities and histopathological findings. Because the evidence consisted exclusively of case reports and small case series, we assessed risk of bias using adapted CARE and JBI criteria, focusing on clarity of case definition, completeness of clinical description, diagnostic certainty, and reporting of outcomes. Given the descriptive nature of the data, no cases were excluded based on quality, but reporting limitations were considered when interpreting results.
Descriptive statistics were employed to ascertain the frequencies and central tendencies of the cohort. Data are expressed as median (interquartile range [IQR]: 25° and 75° percentiles) for quantitative variables and number (percentage) for categorical variables. To compare continuous variables across etiologic groups, we adopted the Kruskal–Wallis test, while for the categorical variables we used the Chi-square test.
3. Results
The database search identified 679 publications, of which 53 met the inclusion and exclusion criteria, reporting a total of 100 patients with Behçet-like syndrome (Table 1).
Characteristics of Patients with Behçet-like Syndrome
The 100 patients included in this review illustrate that BLS represent a heterogeneous group of disorders sharing a Behçet-like phenotype but differing substantially in their underlying mechanisms and clinical expression. The median age at diagnosis was 44 years (IQR 22–52), with symptoms often beginning much earlier (median onset 25 years). Women were more frequently affected (61%), and over half of the cohort originated from non-European countries, particularly Turkey and Japan. Despite this geographic distribution, no ethnicity-specific clinical patterns emerged, and NF-κB–related mutations (A20, NEMO, RELA) appeared evenly distributed across populations.
A defined genetic abnormality was identified in 70% of cases, most commonly involving the NF-κB pathway (TNFAIP3, NFKB1, RELA, IKBKG), but also ADA2, CSF2, and LIG4. HLA-B51 positivity was uncommon (10%), supporting the notion that BLS differs immunogenetically from classical Behçet disease.
Fever was the most frequent systemic manifestation (56%), but its distribution varied markedly by etiology (Table 2 and Table 3). Fever was notably less frequent in the NEMO group and had a higher incidence in infectious diseases when compared to other etiologies.
Mucocutaneous involvement was nearly universal, but its expression varied:
Oral ulcers (including aphthous lesions) occurred in 88% of patients and were particularly prominent in monogenic NF-κB–related disorders (A20, NEMO, RELA).
Genital ulcers were less frequent (57%) but tended to cluster in NEMO-related and infection-associated BLS.
Skin lesions (68%) were dominated by pseudofolliculitis-like eruptions and erythema nodosum. Erythema nodosum was more common in infection-related BLS, reflecting a reactive inflammatory pattern. No cases of urticaria were reported, helping differentiate BLS from other autoinflammatory or allergic conditions. Pathergy was uncommon (11%) and did not distinguish etiologic groups. Joint involvement (43%) showed one of the clearest etiologic patterns:
A20 haploinsufficiency was strongly associated with arthromyalgia and polyarthritis (p = 0.030 and p = 0.010), suggesting a more systemic autoinflammatory phenotype.
NEMO-related BLS showed minimal articular involvement, reinforcing its mucocutaneous predominance. Gastrointestinal involvement was common across the cohort but showed a striking concentration in patients with hematologic disorders:
Inflammatory bowel disease–like features were present in 43% of all patients.
Trisomy 8–associated myelodysplastic syndromes showed the highest rates of intestinal ulceration, bleeding, and stenosis/obstruction.
A20-related disease also showed a tendency toward intestinal ulcers, though less severe than in hematologic BLS.
Ocular involvement (19%) was disproportionately represented in infection-related BLS, particularly tuberculosis-associated cases.
Neurologic manifestations (14%) were scattered across etiologies without a clear pattern.
Thrombosis occurred in 16% of patients, but reports rarely specified whether histopathology resembled classical Behçet vasculitis, limiting interpretation.
A minority of patients (6%) exhibited benign inflammatory lymphoproliferation mimicking PFAPA (Periodic Fever, Aphthous Stomatitis, Pharyngitis, Adenopathy), highlighting the overlap between autoinflammatory syndromes.
Table 2 and Table 3 highlight the distribution of symptoms and signs across the etiologic groups.
A total of 83% of patients received treatment. Glucocorticoids were administered to 65% of patients, and the conventional disease-modifying antirheumatic drugs (cDMARDs) were used in 32%, including colchicine, 5-aminosalicylic acid (5-ASA)/mesalazine, mycophenolate mofetil, dapsone, apremilast, and methotrexate. Some patients (9%) received antiviral and antibiotic therapy, whilst chemotherapy (azacitidine, venetoclax) was necessary in 15% of cases. The biologic disease-modifying antirheumatic drugs (bDMARDs) were used in 22% of patients, primarily anti-TNF-α (16 cases), followed by anti-IL1 (3 cases), anti-IL17 (2 cases), anti-IL23 (1 case), and anti-CD20 (1 case). Allogeneic hematopoietic stem cell transplantation was required in two cases due to trisomy 8 myelodysplastic syndrome.
4. Discussion
This review demonstrates that BLS encompasses a heterogeneous group of conditions that mimic BD but arise from distinct pathogenic mechanisms. Recognizing these patterns is essential because management differs substantially from classical BD.
Despite our systematic review of the literature and the broad heterogeneity of the reported clinical presentations, we were unable to propose a unified or universally applicable definition of Behçet-like syndrome (BLS). The conditions described share clinical features reminiscent of Behçet disease but do not fulfill PEDBD, ISG, or ICBD diagnostic criteria and occur in association with a wide range of underlying disorders. This variability currently prevents the formulation of formal diagnostic criteria or a standardized definition.
We support the current conceptualization of BLS as a clinical condition in which features typical or compatible with Behçet disease—such as recurrent oral or genital aphthosis, cutaneous lesions, arthritis, uveitis, vasculitis, or intestinal ulceration—occur in patients who do not fulfill established diagnostic criteria for BD and who present a clearly identifiable underlying etiology [9,56]. These etiologies include monogenic autoinflammatory disorders, inborn errors of immunity, myelodysplastic or myeloproliferative diseases, infections, or paradoxical reactions to biologic therapies [1,2,3,4,5,6]. The present literature review allows us to describe different subgroups of BLS, associated with different underlying aetiological mechanisms. Interestingly, each subgroup seems to have some distinctive clinical features (Figure 1). We discuss below the features of 4 different groups of BLS. In this framework, BLS represents a secondary or syndromic entity, heterogeneous in its causes and pathogenic mechanisms, yet unified by a clinical phenotype that resembles BD without constituting a primary form of the disease.
4.1. Genetically Related Behçet-like Syndrome
Genetic mutations play a significant role in the pathogenesis of BD, and several monogenic conditions mimic its clinical manifestations. The NF-κB signaling pathway is central to immune cell activation and inflammation (Figure 2). Genetic mutations affecting the NF-κB pathway, notably in genes like A20, NEMO, and RELA, are key contributors to BLS. Mutations in A20, a protein essential for suppressing NF-κB activity, lead to an imbalance in immune responses, causing spontaneous inflammation and an increased response to TNF-α, IL-1β, and IL-18, exacerbating inflammatory processes in BLS patients [12,13].
Monogenic disorders affecting the NF-κB pathway (A20, NEMO, RELA) can closely mimic BD. These mutations disrupt immune regulation and promote exaggerated responses to TNF-α, IL-1β, and IL-18 [12,13,14,15,16], resulting in a Behçet-like inflammatory phenotype. In our synthesis, A20 haploinsufficiency emerged as the most clinically expressive condition, with a combination of recurrent oral ulcers, genital aphthosis, polyarthritis, and gastrointestinal ulceration. The prominence of articular involvement in A20-related disease suggests a systemic autoinflammatory signature that differs from classical BD.
NEMO-related disease, in contrast, tended to present with mucocutaneous features and relatively limited systemic inflammation. RELA haploinsufficiency [13,15,18,19,21,52,57,58,59,60,61,62,63] showed an intermediate phenotype, with mucosal ulceration as the dominant feature. These observations reinforce the need to consider monogenic causes in early-onset, familial, or treatment-refractory Behçet-like presentations, as the therapeutic approach may differ substantially from BD-oriented immunosuppression.
Similarly, mutations in the ADA2 gene, underlying DADA2 disease, could also lead to recurrent oral/genital ulcers and other BD-like symptoms, complicating the diagnostic process and underscoring the need for genetic testing in atypical cases [20,64,65].
For monogenic BD-like diseases, particularly those involving NF-κB pathway mutations, therapies targeting inflammatory cytokines such as TNF-α or IL-1 may be beneficial. In cases where genetic mutations like A20, NEMO, DADA2 or RELA are identified, tailored therapies that modulate the immune response to prevent excessive inflammation should be prioritized [66].
4.2. Infection-Related Behçet-like Syndrome
Infections caused by viruses and mycobacteria can act as triggers for Behçet-like manifestations, particularly in genetically predisposed individuals. This observation supports the molecular mimicry hypothesis, whereby pathogens such as Mycobacterium tuberculosis (MT) and herpes simplex virus (HSV) share antigenic homology with host proteins, including heat shock protein 60 (HSP60), which is overexpressed in active BD lesions and may function as an autoantigen [3,6,67]. In this context, infectious agents may amplify innate immune activation and precipitate a Behçet-like phenotype, especially in individuals carrying susceptibility factors such as HLA-B51.
MT-associated BLS represents the best-documented infectious subgroup. These cases predominantly affect women, with a median onset age of approximately 45 years, and typically present with bipolar aphthosis, erythema nodosum, joint involvement, and ocular inflammation. The temporal relationship between tuberculosis and BLS varies considerably: symptoms may arise concurrently with active infection, years after its onset, or—less commonly—precede the diagnosis of MT infection. This variability highlights the need to consider occult or past infections when evaluating Behçet-like presentations.
Several viral pathogens—including HIV, EBV, HSV, and SARS-CoV-2—have also been implicated in BLS [31,32,33,34,68]. Compared with MT-related cases, viral BLS tends to have a shorter latency between infection and symptom onset. Fever, oral aphthosis, and pseudofolliculitis-like lesions were consistently reported across viral cases, while ocular inflammation was frequent, but major organ involvement was generally absent. The predominance of mucocutaneous and systemic inflammatory features suggests that viral infections may act as potent but transient immune triggers.
From a clinical perspective, these findings underscore the importance of identifying infectious etiologies before initiating immunosuppression. In most cases, targeted antimicrobial therapy leads to improvement of Behçet-like symptoms, confirming the reactive nature of the inflammatory process. However, persistent inflammation after pathogen eradication may require adjunctive immunomodulation, and TNF inhibitors have been used successfully in selected cases [47,68]. Recognizing infection-related BLS is therefore essential to avoid misdiagnosis, prevent inappropriate treatment, and ensure timely management of the underlying infection.
4.3. Myeloproliferative Disorders-Related Behçet-like Syndrome
Proinflammatory cytokines, including IL-1β, TNF-α, and IL-18, play a pivotal role in the pathogenesis of BD [2,5,44,46,69]. In myeloproliferative neoplasms (MPN), which are frequently associated with BD-like symptoms, there is a significant increase in inflammatory cytokine production [70,71], contributing to the chronic inflammatory state observed in affected patients. The interaction between myelodysplastic cells and T-cells may also play a key role in the development of autoimmune features in MPN-associated BLS. Forty-four cases of hematologic neoplasms with BLS have been reported, predominantly in Japanese patients (median age: 68 years). Most cases exhibited an incomplete BD phenotype [42,43,49,72,73,74,75], particularly the intestinal variant, frequently associated with trisomy 8 in myelodysplastic syndrome (MDS). Intestinal involvement (68%) was complicated by obstructions or stenosis in 18% of cases [45,50].
Chemotherapeutic treatment and immunosuppressive therapy, including prednisolone, cyclosporine A, TNF-α inhibitors, and mesalazine, provided symptom relief but were often insufficient for complete disease control. Allogeneic hematopoietic stem cell transplantation (allo-HSCT) successfully treated both MDS and BD-like symptoms in two cases, suggesting its potential as a curative option. Moreover, the literature data report that immunosuppressive therapies such as ruxolitinib may alleviate BLS symptoms in MPN patients [7,51,76,77,78,79,80,81,82]. Overall, these findings emphasize that gastrointestinal Behçet-like disease in older adults—particularly when accompanied by cytopenias or systemic inflammation—should prompt evaluation for underlying MDS or MPN. Early recognition is essential, as management differs substantially from classical BD and may require hematologic intervention.
4.4. BLS, Paradoxical Reactions, and BD Exacerbations Induced by Biological Therapies
Cytokine imbalance may also underlie paradoxical Behçet-like reactions induced by biologic therapies [3,4,48,83,84]. De novo BD or exacerbations of pre-existing BD have been reported following treatment with several biologic agents, particularly anti-IL-17 therapies such as secukinumab and ixekizumab [22,23,24,25,29,85,86,87,88,89,90]. Similar Behçet-like presentations have been described as immune-related adverse events (irAEs) associated with immune checkpoint inhibitors [3,30,91], reflecting the profound immune modulation induced by these treatments.
Clinical manifestations in paradoxical BLS are heterogeneous but frequently include fever and skin lesions (50%), as well as oral and genital ulcers (87% and 75%, respectively). Anterior uveitis and gastrointestinal involvement were reported in 25% and 37.5% of cases, respectively, indicating that paradoxical reactions may reproduce the full spectrum of BD-like inflammation.
These observations have important clinical implications. Patients receiving biologic therapies should be monitored closely for new mucocutaneous or ocular symptoms, as early recognition and timely discontinuation of the offending agent can prevent progression and reduce morbidity [4,22,23,25,29]. Corticosteroids remain the mainstay of treatment and lead to symptom resolution in most cases [12,13,14,15,25]. In selected situations, switching to an alternative biologic class may be necessary to maintain control of the underlying disease while avoiding recurrence of Behçet-like manifestations.
4.5. Strengths and Limitations
This review is, to our knowledge, the first to comprehensively synthesize all published cases of BLS up to January 2024. Despite the heterogeneity of the included reports, the aggregated data offer valuable insights into the mechanisms that generate Behçet-like phenotypes and help delineate clinically relevant subgroups.
However, the evidence is inherently limited. All data derive from case reports and small case series, which are subject to publication bias, incomplete reporting, and variability in diagnostic work-up. Clinical features were not uniformly described, and histopathologic confirmation was often lacking. As a result, frequency estimates and inter-group comparisons should be interpreted cautiously, and causal relationships cannot be inferred.
The overlap between BD and BLS also raises conceptual questions. The low prevalence of HLA-B51 positivity and the incomplete penetrance observed in familial BD suggest that genetic background alone does not determine phenotype [17,18,19,20,21,52,56,57,58,59,60,61,62,63,64,65,92]. Environmental triggers, infections, hematologic disorders, and cytokine dysregulation likely modulate disease expression, supporting the idea of a spectrum rather than a strict dichotomy (Figure 3).
4.6. Practical Recommendations for Clinicians
Based on the patterns identified in this review, several practical considerations emerge:
Suspect BLS rather than BD when Behçet-like features occur with cytopenias, recurrent infections, early-onset autoinflammation, or recent exposure to biologics.
Investigate monogenic autoinflammatory diseases (A20, RELA, DADA2, NEMO) in early-onset or familial cases with prominent mucocutaneous involvement.
Evaluate for myelodysplastic syndromes, particularly trisomy 8, in patients with intestinal ulcers, unexplained cytopenias, or poor response to BD-oriented therapy.
Consider infectious triggers—especially tuberculosis and chronic viral infections—when fever and erythema nodosum predominate.
Tailor treatment to the underlying etiology, as management differs substantially from classical BD.
Monitor for paradoxical reactions in patients receiving IL-17 inhibitors or immune checkpoint inhibitors.
Recognizing BLS as a distinct clinical construct is essential to avoid misdiagnosis, prevent inappropriate immunosuppression, and guide targeted therapy. Moreover, the study of BLS may provide valuable insights into BD pathogenesis and help identify new therapeutic targets.
5. Conclusions
This extensive literature review highlights the characteristics of the different entities included in BLS, related to classical and recently described autoinflammatory syndromes, myeloproliferative diseases, viral and mycobacterial infections, as well as paradoxical reactions secondary to drug treatment. The typical clinical manifestations of BD help us to conceptualize that BD is the expression of a complex cytokine balance disorder, in the context of a genetic predisposition, sometimes influenced by environmental factors, and with possible interactions with other inflammatory pathways.
Given the potential severity of BLS, being aware of the different BLS entities described in this article is fundamental for the correct management of patients. Furthermore, the development of effective therapeutic strategies remains an urgent priority. Future research focusing on the molecular mechanisms underlying immune dysregulation in BLS is essential to identify optimal targeted treatments and improve patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Perazzio S.F. Allenspach E.J. Eklund K.K. Varjosalo M. Shinohara M.M. Torgerson T.R. Seppänen M.R.J. Behçet disease (BD) and BD-like clinical phenotypes: NF-κB pathway in mucosal ulcerating diseases Scand. J. Immunol.202092 e 1297310.1111/sji.1297332889730 · doi ↗ · pubmed ↗
- 2Koba S. Sekioka T. Takeda S. Miyagawa-Hayashino A. Nishimura K. Imashuku S. Acute Monocytic Leukemia Masquerading Behçet’s Disease-Like Illness at Onset in an Elderly Female Case Rep. Hematol.20162016423127610.1155/2016/423127627610252 PMC 5004031 · doi ↗ · pubmed ↗
- 3Yazici Y. Hatemi G. Bodaghi B. Cheon J.H. Suzuki N. Ambrose N. Yazici H. Behçet syndrome Nat. Rev. Dis. Primers.202176710.1038/s 41572-021-00301-134531393 · doi ↗ · pubmed ↗
- 4Dincses E. Yurttas B. Esatoglu S.N. Melikoglu M. Hamuryudan V. Seyahi E. Secukinumab induced Behçet’s syndrome: A report of two cases Oxf. Med. Case Rep.20192019 omz 04110.1093/omcr/omz 04131198577 PMC 6544425 · doi ↗ · pubmed ↗
- 5Ishikawa Y. Sasaki R. Ishiwata A. Hatakeyama S. Matsumura M. Sato T. A case of Behçet’s-like disease associated with trisomy 8-positive myelodysplastic syndrome carrying MEFV E 148Q variant presented with periodic fever Mod. Rheumatol. Case Rep.2023747047410.1093/mrcr/rxad 01536881672 · doi ↗ · pubmed ↗
- 6Zhang D. Su G. Zhou Z. Lai J. Clinical characteristics and genetic analysis of A 20 haploinsufficiency Pediatr. Rheumatol. Online J.2021197510.1186/s 12969-021-00558-634030699 PMC 8147020 · doi ↗ · pubmed ↗
- 7Hatemi G. Seyahi E. Fresko I. Talarico R. Uçar D. Hamuryudan V. Behçet’s syndrome: One year in review 2024 Clin. Exp. Rheumatol.2024421999200710.55563/clinexprheumatol/fqao 1639404479 · doi ↗ · pubmed ↗
- 8Taskiran E.Z. Sonmez H.E. Kosukcu C. Tavukcuoglu E. Yazici G. Esendagli G. Batu E.D. Kiper P.O.S. Bilginer Y. Alikasifoglu M. A Novel Missense LIG 4 Mutation in a Patient with a Phenotype Mimicking Behçet’s Disease J. Clin. Immunol.2019399910510.1007/s 10875-018-0587-730617623 · doi ↗ · pubmed ↗