Case Report of Overlap of Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in a 5-Year-Old with New-Onset Type 1 Diabetes Mellitus: Diagnostic and Management Considerations
Filippos Filippatos, Georgios Themelis, Maria Dolianiti, Christina Kanaka-Gantenbein, Konstantinos Kakleas

TL;DR
A 5-year-old child with new-onset type 1 diabetes presented with a rare overlap of diabetic ketoacidosis and hyperosmolar hyperglycemic state, requiring careful management to avoid neurological complications.
Contribution
This case report highlights the diagnostic and therapeutic challenges of DKA/HHS overlap in children and emphasizes osmolality-guided treatment strategies.
Findings
The patient's condition was managed successfully with osmolality-guided fluids and insulin therapy.
The case demonstrates the importance of early identification and careful monitoring to prevent cerebral edema.
The patient recovered fully without neurological complications.
Abstract
Background and Clinical Significance: Overlap of diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) in children is a rare but life-threatening metabolic emergency. The coexistence of hyperosmolality and ketoacidosis increases neurologic vulnerability and complicates fluid and insulin management. Early identification and osmolality-guided therapy are essential to prevent cerebral edema and other complications. This case describes a 5-year-old boy with new-onset type 1 diabetes mellitus (T1D) presenting with DKA/HHS overlap two weeks after influenza vaccination—an unusual temporal association without proven causality. Case Presentation: A previously healthy 5-year-old presented with progressive polyuria, polydipsia, nocturnal enuresis, fatigue, and drowsiness. Two weeks earlier, he had received the influenza vaccine. Examination revealed moderate dehydration without…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
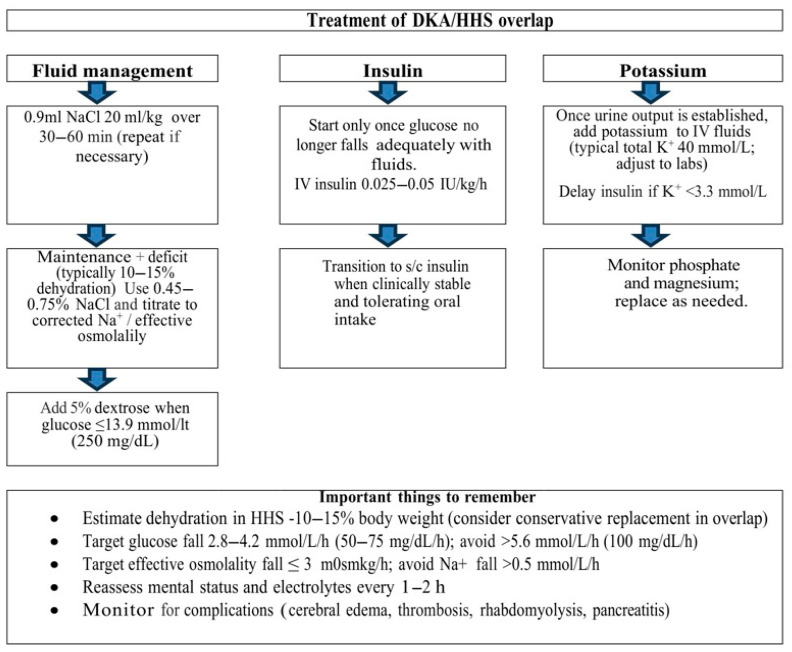 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes and associated disorders · Diabetes Management and Research · Pancreatic function and diabetes
1. Introduction and Clinical Significance
In childhood, HHS remains uncommon, but it is reported more often in youth with obesity and type 2 diabetes mellitus (T2D) than in those with type 1 diabetes mellitus (T1D) [1,2].
We present the unusual case of a previously healthy 5-year-old boy with newly diagnosed autoimmune type 1 diabetes who met criteria for overlap diabetic ketoacidosis and hyperosmolar hyperglycemic state (DKA/HHS)—a phenotype rarely reported in preschool-age children and more often described in adolescents. This report emphasizes three practical points: (i) confirmation of hypertonicity using corrected sodium and osmolality rather than glucose alone, (ii) an osmolality-guided fluid strategy with conservative correction targets, and (iii) delayed, low-dose insulin initiation once glucose decline plateaus with fluids to reduce the risk of rapid osmotic shifts. Severe hypertriglyceridemia at presentation is discussed as a marker of profound insulin deficiency and a potential source of laboratory artifacts. The temporal proximity to influenza vaccination is reported as a clinical detail; no causal relationship is inferred.
2. Case Presentation
The patient was a previously healthy 5-year-old boy who developed several weeks of progressive polyuria, polydipsia, nocturnal enuresis, fatigue, and reduced oral intake. Two weeks before presentation, he received the seasonal influenza vaccine; there was no history of intercurrent febrile illness, gastrointestinal symptoms, abdominal pain, recent steroid exposure, or other medications. Family history was negative for diabetes or autoimmune disease, and immunizations were otherwise up to date.
At presentation, vital signs were notable for tachycardia, age-appropriate blood pressure and respiratory rate, and normal oxygen saturation on room air. On examination in the emergency department, the child appeared dehydrated yet alert and interactive. He had dry mucous membranes and delayed capillary refill, with otherwise normal work of breathing and no Kussmaul respirations. No focal neurologic deficits were detected, and cardiopulmonary and abdominal examinations were unremarkable. Point-of-care glucose exceeded the meter range, prompting confirmation with laboratory testing.
Laboratory evaluation confirmed a mixed DKA/HHS presentation. Venous blood gas showed severe hyperglycemia (45.9 mmol/L [826 mg/dL]; reference 3.9–7.8 mmol/L), acidemia (pH 7.29; reference 7.35–7.45), and low bicarbonate (12 mmol/L; reference 22–26 mmol/L), with moderate ketonuria (50 mg/dL) consistent with DKA. Measured serum osmolality was 344 mOsm/kg (reference 275–295 mOsm/kg), and serum sodium was 129 mmol/L (reference 135–145 mmol/L; corrected 143 mmol/L), indicating marked hypertonicity and meeting the HHS criteria. Effective osmolality (calculated as 2 × Na^+^ [mmol/L] + glucose [mg/dL]/18; target fall ≤ 3 mOsm/kg/h) and corrected sodium (using +1.6 mEq/L per 100 mg/dL glucose above 100 mg/dL) were closely monitored, and therapy prioritized gradual osmolar correction to mitigate neurologic risk.
Ancillary evaluation included serial monitoring of glucose, electrolytes, and acid–base status. The trajectory of effective osmolality was closely tracked (target fall ≤ 3 mOsm/kg/h), and sodium was corrected to avoid a decline >0.5 mmol/L/h. Autoimmune testing supported new-onset T1D (IA-2 antibody positive) with low C-peptide (0.109 nmol/L; reference 0.26–0.63 nmol/L) and markedly elevated HbA1c (16%; reference < 5.7%).
Initial management followed a DKA protocol. The patient received a 20 mL/kg bolus of 0.9% NaCl over the first 30–60 min, with the option to repeat if hemodynamic instability persisted. He was started on maintenance fluids plus 5% estimated dehydration with 0.9% NaCl. Once full laboratory results confirmed marked hyperosmolality and hypertonicity, the diagnosis was refined to mixed DKA/HHS. Intravenous insulin, initially commenced at 0.07 IU/kg/h, was temporarily stopped, and fluids were adjusted to maintenance plus approximately 10% deficit using 0.45–0.75% NaCl supplemented with potassium (starting potassium concentration 40 mmol/L in the infusate), titrated to the corrected sodium and effective osmolality trajectory. This regimen continued with frequent monitoring until blood glucose, which initially fell with fluids alone, plateaued at approximately 22.4 mmol/L (403 mg/dL). At that point, intravenous insulin was reintroduced at approximately 0.03 IU/kg/h and subsequently increased to 0.05 IU/kg/h. When blood glucose reached 13.9 mmol/L (250 mg/dL), dextrose 5% was added to the intravenous fluids to prevent an excessive fall in glucose and osmolality. Electrolytes—particularly potassium, phosphate, and magnesium—were monitored frequently and supplemented according to serial measurements and urine output. Bedside glucose and effective osmolality were checked at short intervals to maintain the planned rate of correction. The patient responded well to fluid and insulin administration.
Characteristics and diagnostic criteria for DKA, HHS, and DKA/HHS overlap are summarized in Table 1. Treatment recommendations are schematically illustrated in Figure 1, and key biochemical values and treatment milestones during the initial resuscitation are summarized in Table 2.
Neurologic status remained stable without headache, irritability, or mental-status change. Ketosis resolved, and effective osmolality normalized over 24–48 h. He transitioned to a subcutaneous basal–bolus regimen, received structured diabetes education (sick-day rules and ketone monitoring), and was discharged in stable condition with a diagnosis of T1D. Early outpatient follow-up documented good clinical recovery, no recurrent decompensation, and intact neurologic examination.
3. Discussion
This case illustrates an uncommon but clinically significant presentation of hyperglycemic crisis in a preschool child, with overlap between DKA and HHS. It emphasizes practical points for recognition and osmolality-guided management. The child presented severe hyperglycemia, metabolic acidosis/ketonuria, and hyperosmolality, thereby fulfilling the features of both entities. Framing the evaluation around effective serum and corrected sodium was pivotal because these metrics more closely track neurologic risk than glucose alone and directly inform fluid tonicity and the timing/intensity of insulin therapy.
DKA/HHS overlap in pediatrics is under-recognized and can be missed when attention centers solely on acidosis or on absolute glucose levels. There is one previous similar case of DKA/HHS overlap reported in a 14-year-old adolescent girl in the setting of hypernatremic dehydration due to cognitive impairment and inability to express fluid intake needs [4]. There are a few other reported cases in the literature of older children with HHS following T1D, but this is the first report in a preschool child [5,6,7,8]. A structured approach—documenting pH/HCO_3_^−^, quantitative ketones, corrected Na^+^, measured/effective osmolality, and serial neurologic assessments—reduces the risk of delayed diagnosis or misclassification. In our patient, the combination of hyperglycemia, metabolic acidosis, ketonuria, and hyperosmolality established the overlap diagnosis and justified management targets that prioritized controlled osmolar correction.
A uniform consensus on the diagnostic criteria and treatment of mixed DKA/HHS remains challenging due to limited pediatric data [9]. DKA is typically defined by hyperglycemia (blood glucose > 11 mmol/L (>200 mg/dL)), a venous pH < 7.30, serum bicarbonate concentration < 18 mmol/L, and the presence of ketonemia or ketonuria, whereas HHS is characterized by blood glucose > 33.3 mmol/L (>600 mg/dL), arterial pH > 7.30 or venous pH > 7.25, serum bicarbonate concentration > 15 mmol/L, mild ketonuria, mild or absent ketonemia, and serum osmolality > 320 mOsm/kg [1]. Zahran et al. have pointed out distinct characteristics and diagnostic criteria for HHS and DKA in children and proposed a practical framework for recognizing HHS and mixed presentations [10]. Based on these criteria, our patient, with undiagnosed diabetes mellitus, blood glucose > 33.3 mmol/L (>600 mg/dL), serum osmolality > 320 mOsm/kg, and ketoacidosis, was best categorized as having DKA/HHS overlap [10].
The overlap phenotype can be conceptualized as severe insulin deficiency with concomitant hyperosmolar dehydration from prolonged osmotic diuresis [9,11]. Even modest ketogenesis, when superimposed on marked hypertonicity, amplifies neurologic vulnerability [9,11]. In addition to cerebral edema, other reported complications of HHS and mixed DKA/HHS include venous and arterial thrombosis, rhabdomyolysis, pancreatitis, and acute kidney injury, underscoring the need for meticulous monitoring of fluid balance, coagulation status, muscle enzymes, and organ function [1,12]. This dual process explains why fluid strategy, tonicity selection (0.9% vs. 0.45% NaCl), and the tempo of correction are as critical as insulin dosing. Our patient’s favorable outcome underscores the value of titrating therapy to physiology-based targets rather than fixed formulas.
The treatment of HHS is based on prompt recognition and appropriate fluid management, insulin administration, and electrolyte monitoring. In 2022, ISPAD published recommendations for the management of DKA, HHS, and mixed DKA/HHS [1]. Fluid losses in HHS usually range between 110 and 220 mL/kg, corresponding to an estimated deficit of roughly 10–15% of body weight and approximately twice that in DKA [3,13]. In our patient, we initially administered a 20 mL/kg bolus of 0.9% NaCl, followed by maintenance fluids and an estimated 10% deficit. Because of the mixed DKA/HHS presentation, we chose a conservative approach to deficit replacement, using 0.45–0.75% NaCl for ongoing maintenance and deficit correction, together with potassium supplementation (starting concentration 40 mmol/L in the infusate). Fluid management was guided by reducing effective osmolality at a rate < 3 mOsm/kg/h and by avoiding a plasma sodium decline > 0.5 mmol/L/h to minimize the risk of cerebral edema [1,14]. There is variability in guidelines regarding NaCl tonicity: some recommend 0.9% NaCl during initial resuscitation, particularly when the patient is hemodynamically unstable, followed by more hypotonic solutions (0.45–0.75% NaCl) once the circulation has stabilized and hyperosmolality persists, to avoid overcorrection and brain edema [1,3,15]. However, extensive pediatric data suggest that neither the rate of fluid administration nor the sodium chloride content alone significantly affects neurological outcome when modern protocols are followed [16].
We initially started intravenous insulin according to a DKA protocol, but this was subsequently stopped once the diagnosis of DKA/HHS overlap was established. Current pediatric guidance recommends delaying exogenous insulin administration in HHS and mixed DKA/HHS until circulation has stabilized. Fluid therapy alone no longer produces an adequate fall in blood glucose, because the combination of improved renal perfusion with glucosuria and the hypoglycemic effect of insulin can otherwise result in a rapid fall in plasma glucose, circulatory collapse, and thrombosis [1,3]. In addition, in DKA/HHS overlap, ketosis is often less pronounced than in isolated DKA, so a short delay in insulin initiation is usually not detrimental, provided careful fluid resuscitation and monitoring are in place. We restarted insulin at approximately 0.03 IU/kg/h and subsequently titrated towards 0.05 IU/kg/h, consistent with guidelines that recommend an infusion rate of about 0.025–0.05 IU/kg/h when plasma glucose levels fail to decrease by at least 2.8–4.2 mmol/L/h (50–75 mg/dL/h) with fluid administration alone [3,11].
Overall, management of mixed DKA/HHS should be individualized, integrating the child’s biochemical profile, hemodynamic status, and comorbidities, and guided by clinical judgment informed by evidence from the management of isolated DKA and isolated HHS [1,9,11].
An additional notable feature was severe hypertriglyceridemia (14.0 mmol/L [1238 mg/dL]) at presentation. Marked hypertriglyceridemia can accompany insulin deficiency through increased lipolysis and reduced lipoprotein lipase activity. From a practical standpoint, lipemia may also contribute to pseudohyponatremia when sodium is measured by indirect ion-selective electrodes, potentially underestimating true tonicity; therefore, sodium trends should be interpreted alongside measured osmolality (or direct ISE sodium) in overlap presentations. Triglycerides > 11.3 mmol/L (>1000 mg/dL) should also prompt clinical vigilance for pancreatitis and other complications, guided by symptoms and local protocols [17].
The presentation occurred two weeks after the influenza vaccination. While temporal association is factual, causality cannot be inferred from a single case, especially given weeks of antecedent polyuria/polydipsia consistent with evolving autoimmune β-cell failure. Alternative explanations (undiagnosed type 1 diabetes trajectory, intercurrent subclinical infection, variable intake) remain plausible. We therefore present vaccination timing as a clinical detail rather than a precipitating cause. This cautious framing avoids over-interpretation and aligns with best practices for case reports. Prior reports describe transient dysglycemia after influenza vaccination in some individuals with diabetes, typically resolving within 72 h; such observations do not establish a causal pathway to severe hyperglycemic crises [12]. Larger epidemiologic data would be needed to evaluate whether vaccination may, at most, act as a nonspecific stressor that unmasks pre-existing insulin deficiency rather than causing it.
Published pediatric series and case descriptions highlight that HHS and DKA/HHS overlap, although less frequently than classic DKA, and that both carry a higher risk of fluid-electrolyte derangements and neurologic complications [11]. Consistent themes include delayed recognition, underestimation of dehydration, and overly rapid osmolar shifts during treatment. Our experience reinforces three actionable lessons: (i) calculate and track effective osmolality at the bedside; (ii) defer or minimize early insulin in hyperosmolar presentations until fluids have begun to restore perfusion and dilute glucose safely; and (iii) institute standardized neurologic monitoring regardless of initial mental status.
For emergency and pediatric teams, we recommend an osmolality-first checklist in any child with glucose > 33.3–39.0 mmol/L (600–700 mg/dL): record measured and effective osmolality, corrected Na^+^, and set explicit hourly targets for glucose and osmolality decline. Quality-improvement work could test whether such checklists reduce variability in care and neurologic complications. At the research level, multicenter registries should better define the incidence, precipitating contexts, and outcomes of pediatric DKA/HHS overlap and validate physiology-based titration rules prospectively.
As a single-patient case, generalizability is constrained. We lacked immediate serum β-hydroxybutyrate quantification at presentation (qualitative ketonuria was available), and we did not perform neuroimaging because serial examinations remained normal. Nonetheless, the quantitative mapping to diagnostic thresholds, explicit therapeutic targets, and transparent reporting of calculations provide practical value.
4. Conclusions
This case underscores that pediatric DKA/HHS overlap can be managed safely when diagnosis is anchored to osmolality and sodium physiology and when fluids, insulin, and dextrose are titrated to conservative correction targets under close neurologic and biochemical surveillance. In a preschool child with new-onset type 1 diabetes, severe hypertriglyceridemia may be an additional clue to profound insulin deficiency and may complicate sodium interpretation; integrating measured osmolality can help prevent underestimation of hypertonicity. The temporal proximity to influenza vaccination is noted but non-causal. Clear reporting of calculations and targets may help standardize care and improve outcomes in this high-risk pediatric presentation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Glaser N. Fritsch M. Priyambada L. Rewers A. Cherubini V. Estrada S. Wolfsdorf J.I. Codner E. ISPAD Clinical Practice Consensus Guidelines 2022: Diabetic ketoacidosis and hyperglycemic hyperosmolar state Pediatr. Diabetes 20222383585610.1111/pedi.1340636250645 · doi ↗ · pubmed ↗
- 2Rosenbloom A.L. Hyperglycemic Hyperosmolar State: An Emerging Pediatric Problem J. Pediatr.201015618018410.1016/j.jpeds.2009.11.05720105637 · doi ↗ · pubmed ↗
- 3Ng S.M. Edge J. Hyperglycaemic Hyperosmolar State (HHS) in children: A practical guide to management Paediatr. Child Health 20172717117510.1016/j.paed.2017.01.002 · doi ↗
- 4Parra Villasmil M.G. Patel S. Tansey M. Badheka A. Chegondi M. A Rare Presentation of New-Onset Type 1 Diabetes Mellitus in a Developmentally Delayed Child with an Overlap of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State Cureus 202214 e 2898310.7759/cureus.2898336237743 PMC 9548379 · doi ↗ · pubmed ↗
- 5Cho Y.M. Park B.S. Kang M.J. A case report of hyperosmolar hyperglycemic state in a 7-year-old child: An unusual presentation of first appearance of type 1 diabetes mellitus Medicine 201796 e 736910.1097/MD.000000000000736928640151 PMC 5484263 · doi ↗ · pubmed ↗
- 6Chun S.H. Lee H.S. Hwang J.S. Hyperosmolar hyperglycemic state as the first manifestation of type 1 diabetes mellitus in an adolescent male: A case report Ann. Pediatr. Endocrinol. Metab.202227697210.6065/apem.2142002.00134670070 PMC 8984746 · doi ↗ · pubmed ↗
- 7Watanabe S. Kido J. Ogata M. Nakamura K. Mizukami T. Hyperglycemic hyperosmolar state in an adolescent with type 1 diabetes mellitus Endocrinol. Diabetes Metab. Case Rep.2019201918013110.1530/EDM-18-013130836328 PMC 6432974 · doi ↗ · pubmed ↗
- 8Shahramian I. Ostad Rahimi P. Radvar S. Hyperosmolar hyperglycemic state in children: Case report and review of the literature J. Klin. Endokrinol. Stoffwechs.202215606210.1007/s 41969-022-00164-135669285 PMC 9152644 · doi ↗ · pubmed ↗