Robotic-assisted radical cystoprostatectomy and intracorporeal ileal conduit formation in a patient with prior total colectomy and J-pouch
Grace S Sutherland, Jodie M McDonald, Amanda C Chung, Justin V Vass, Ahmed G Goolam, Matthew R Winter

TL;DR
This paper describes a successful robotic surgery for bladder cancer in a patient with prior bowel surgery, highlighting new techniques to manage complex anatomy.
Contribution
The paper presents the first reported case of robotic-assisted cystoprostatectomy in a patient with prior total colectomy and J-pouch.
Findings
The surgery was completed without complications using intraoperative strategies like rectal indocyanine green and a short discard segment.
The patient had favorable oncologic and functional outcomes postoperatively.
The case outlines technical considerations for cystectomy in patients with prior large bowel resection.
Abstract
We present the first reported case of robotic-assisted radical cystoprostatectomy and ileal conduit formation in a patient with prior total colectomy and J-pouch. The anatomy posed significant technical risk due to end artery pouch perfusion and changes in the posterior plane. Intraoperative strategies, including rectal indocyanine green and a short discard segment when constructing the conduit enabled successful outcomes. The procedure was completed without complication, and the patient had a favourable oncologic and functional status postoperatively. This case demonstrates the technical considerations of cystectomy in patients with previous large bowel resection and reconstruction, and the outlined strategies are relevant across multiple clinical settings.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
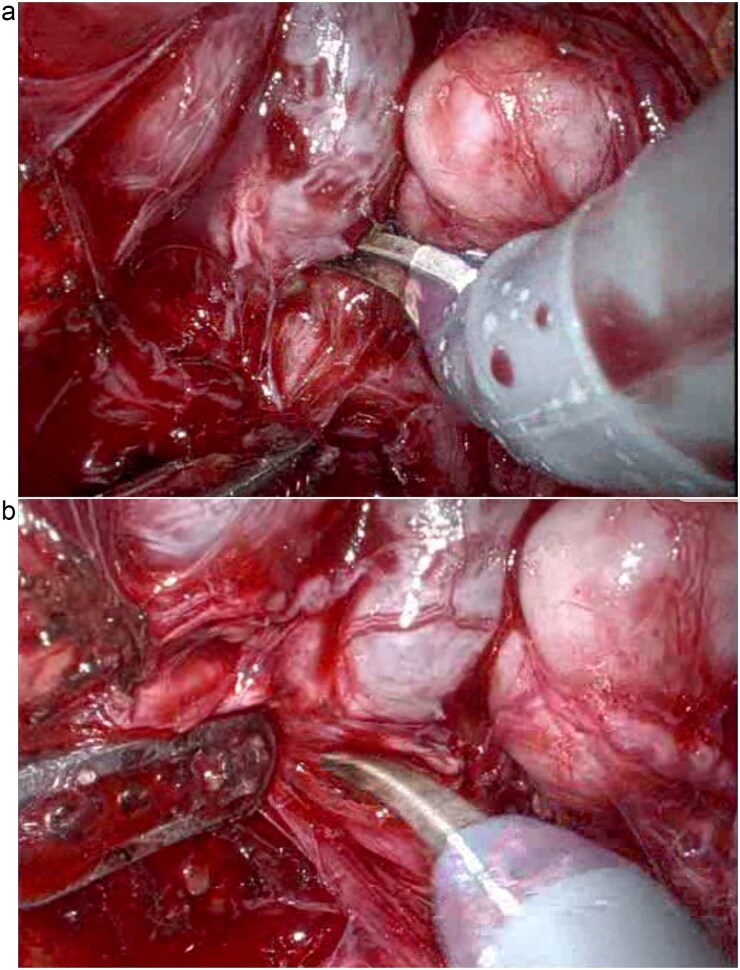 Figure 1
Figure 1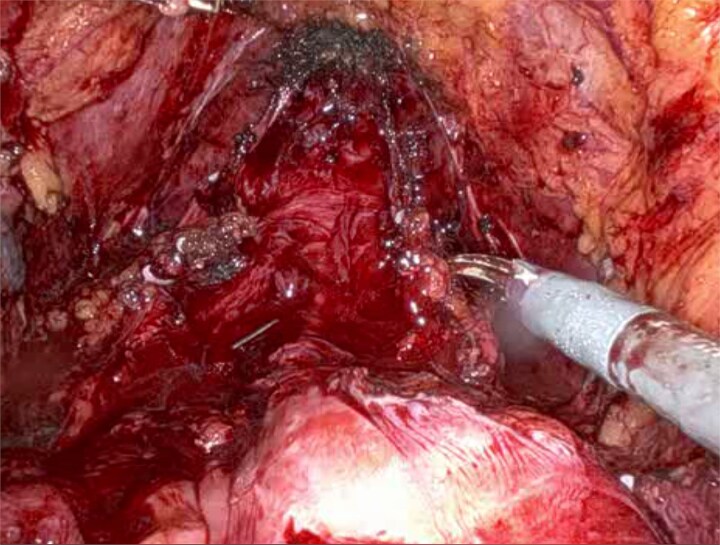 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Ureteral procedures and complications · Diverticular Disease and Complications
Introduction
Previous surgery alters vascular anatomy creating challenging conditions in subsequent pelvic surgery. In patients who have undergone large bowel surgery necessitating ligation of the inferior mesenteric artery, collateral blood supply is disrupted [1]. Following total proctocolectomy with ileal pouch–anal anastomosis (J-pouch), perfusion of the J-pouch depends primarily on the superior mesenteric artery, particularly the ileocolic branch [2]. The absence of collateral supply leaves the J-pouch reliant on end arteries, placing it at high risk of revascularization [2]. These anatomical changes, combined with dense adhesions and scarring from prior surgery can create a challenging environment during any subsequent pelvic surgery [3].
Radical cystectomy with pelvic lymph node dissection for muscle-invasive bladder cancer remains the standard of care for achieving long-term disease control in organ-confined disease [4]. Urinary diversion is achieved commonly via ileal conduit formation [5]. Robotic-assisted techniques are now widely adopted in urological surgery, providing enhanced vision, precision, and ergonomics [6].
To our knowledge, this is the first reported case of robotic radical cystectomy in a patient with prior total colectomy and J-pouch. These patients present a uniquely high-risk scenario due to end-artery pouch perfusion without arterial collateralization and altered pelvic anatomy. Together, these factors significantly increase the risk of unintentional pouch revascularization, making successful robotic dissection and preservation of pouch integrity technically demanding.
Case presentation
A 58-year-old man with a history of familial adenomatous polyposis and previous total colectomy and J-pouch presented with muscle-invasive bladder cancer. Following four cycles of neoadjuvant chemotherapy, he underwent robotic-assisted radical cystoprostatectomy, bilateral pelvic lymph node dissection, and ileal conduit formation. Surgical entry was achieved via a modified Hasson technique and robotic port placement. Careful dissection, particularly in the posterior plane (Fig. 1), was required due to altered pelvic anatomy. Indocyanine green was injected directly into the J-pouch via a rectal tube to access perfusion and anatomical planes. Subsequent ligation with vessel sealer of the vascular pedicles was performed, and the bladder and prostate were removed en bloc (Fig. 2). Extensive adhesiolysis was necessary to mobilize sufficient small bowel to form the conduit and reach the anterior abdominal wall without tension. A 15 cm segment of small bowel proximal to the J-pouch was isolated using an Echelon stapler, and a distal 5-cm discard segment was taken to ensure adequate distal perfusion of the conduit and aid mobility for stoma formation. Bowel continuity was restored with a stapled side to side anastomosis. The ileal conduit was formed intracorporeally and delivered through the abdominal wall.
Posterior pelvic dissection demonstrating the challenging plane in the absence of normal perirectal fat (a and b).
Intraoperative view showing the J-pouch after removal of the bladder and prostate.
Indocyanine green was given intravascularly to assess ureteric perfusion, with excision of any distal devascularized segments. The ureters were then anastomosed to the conduit using the Bricker technique with interrupted 4–0 vicryl sutures. Haemostasis was achieved with vessel sealer, with minimal clipping and suturing near the J-pouch. There were no intraoperative complications, and total estimated blood loss was 150 ml.
Postoperative recovery was uncomplicated. Bowel function returned on postoperative day four. Ureteric stents and surgical drains were removed on Day 6, and the patient was discharged home on Day 7. Final histopathology showed complete treatment response (pT0) of urothelial carcinoma with clear surgical margins and incidental ISUP grade group 3 prostate adenocarcinoma.
Discussion
Robotic-assisted radical cystectomy with intracorporeal ileal conduit formation in patients with prior total colectomy and J-pouch reconstruction involves significant technical difficulty and vascular risk due to dense adhesions and the pouch’s reliance on end-artery perfusion. The changes in the posterior plane secondary to the loss of the usual perirectal fat and denonvilliers fascia, as well as the pouch being comprised of thin walled small bowel, make this dissection particularly challenging (Fig. 1). Additionally, remaining length of small bowel has a functional consideration and short gut syndrome has to be considered. To our knowledge, this is the first reported case of such a procedure.
Few reports describe pelvic robotic surgery following major colorectal procedures. Siddiqui et al. found that among patients undergoing robotic prostatectomy, those with prior colectomy had the highest rates of adhesiolysis and the longest operative times compared to all other types of previous abdominal surgery [7]. Mustafa et al. concluded that robotic radical prostatectomy is feasible and safe after previous colorectal surgery, despite increased technical complexity due to altered pelvic anatomy [8]. Watanabe et al. described a case of robotic cystectomy following low anterior resection, in which dense adhesions from prior surgery significantly complicated pelvic dissection [3].
Other studies support the feasibility of robotic pelvic surgery in patients with prior abdominal operations. Yuh et al. found that while previous lower abdominal surgery increased postoperative complications, it did not prevent successful robotic completion [9]. Similarly, Park et al. showed that prior abdominal surgery, including gynaecologic procedures, did not adversely affect outcomes in robotic colorectal surgery [10].
Conclusion
This case demonstrates that robotic cystoprostatectomy with intracorporeal ileal conduit formation is technically achievable in patients with prior total colectomy and J-pouch. With appropriate intraoperative strategies, such as direct indocyanine green injection into the J-pouch and a distal discard segment when constructing the conduit, safe dissection, and pouch preservation can be accomplished despite complex pelvic anatomy and vascular constraints.
Learning points
Prior colectomy and J-pouch reconstruction significantly alter pelvic vascular anatomy.Direct indocyanine green injection into the pouch helps delineate planes and assess perfusion.A distal discard segment during conduit isolation aids conduit mobility and perfusion.Robotic techniques enable precise dissection in anatomically distorted pelvises.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sakorafas GH, Zouros E, Peros G. Applied vascular anatomy of the colon and rectum: clinical implications for the surgical oncologist. Surg Oncol 2006;15:243–55.17531744 10.1016/j.suronc.2007.03.002 · doi ↗ · pubmed ↗
- 2Helavirta J, Haapamäki MM, Koskensalo S, et al. Vascular considerations in ileal pouch surgery: a review. Tech Coloproctol 2020;24:935–42.32385673
- 3Watanabe S, Kobayashi H, Hiroe N, et al. Robot-assisted radical cystectomy for bladder cancer after low anterior resection: a case report. Asian J Endosc Surg 2024;17:e 13345.38943367 10.1111/ases.13345 · doi ↗ · pubmed ↗
- 4Patel VG, Oh WK, Galsky MD. Treatment of muscle-invasive and advanced bladder cancer in 2020. CA Cancer J Clin 2020;70:404–23.32767764 10.3322/caac.21631 · doi ↗ · pubmed ↗
- 5Lee RK, Abol-Enein H, Artibani W, et al. Urinary diversion after radical cystectomy for bladder cancer: options, patient selection, and outcomes. BJU Int 2014;113:11–23.24330062 10.1111/bju.12121 · doi ↗ · pubmed ↗
- 6Rassweiler JJ, Autorino R, Klein J, et al. Future of robotic surgery in urology. BJU Int 2017;120:822–41.28319324 10.1111/bju.13851 · doi ↗ · pubmed ↗
- 7Siddiqui SA, Krane LS, Bhandari A, et al. The impact of previous inguinal or abdominal surgery on outcomes after robotic radical prostatectomy. Urology 2010;75:1079–82.19896178 10.1016/j.urology.2009.09.004 · doi ↗ · pubmed ↗
- 8Mustafa M, Pettaway CA, Davis JW, et al. Robotic or open radical prostatectomy after previous open surgery in the pelvic region. Korean J Urol 2015;56:131–7.25685300 10.4111/kju.2015.56.2.131PMC 4325117 · doi ↗ · pubmed ↗