Long-term mortality in pediatric sepsis: a systematic review and meta-analysis
Yongbiao Lv, Jiayi Zheng, Junxiang Cai, Jingwei Shui, Yuntao Liu, Zhongde Zhang

TL;DR
This study finds that 11% of children who survive sepsis die in the long term after discharge, highlighting the need for better post-discharge care.
Contribution
The first meta-analysis quantifying long-term mortality in pediatric sepsis survivors.
Findings
Pooled long-term mortality after pediatric sepsis is 11%.
Significant heterogeneity (I² = 98.2%) was observed across studies.
Post-discharge mortality remains high regardless of follow-up period or setting.
Abstract
Pediatric sepsis represents a significant factor in the mortality rates among children, with survivors remaining highly fragile during the period following discharge. While in-hospital and short-term mortality have been widely studied, the long-term mortality of pediatric sepsis is not adequately synthesized or appreciated. This study aims to estimate the long-term mortality associated with pediatric sepsis, providing a basis for optimizing post-discharge surveillance and care protocols. This systematic review and meta-analysis followed PRISMA guidelines and was registered in PROSPERO (CRD420251137504). Exhaustive searches were conducted in PubMed, Embase, the Cochrane Library, and Web of Science for studies published from the inception of each database to June 30, 2025. Studies reporting long-term mortality in pediatric sepsis patients diagnosed using international consensus criteria…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
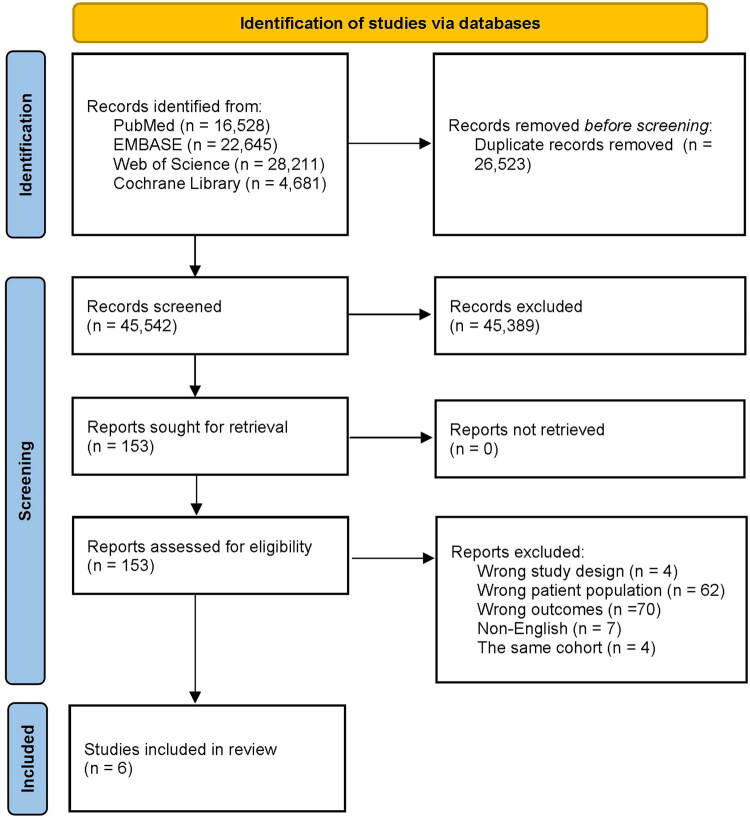 Figure 1
Figure 1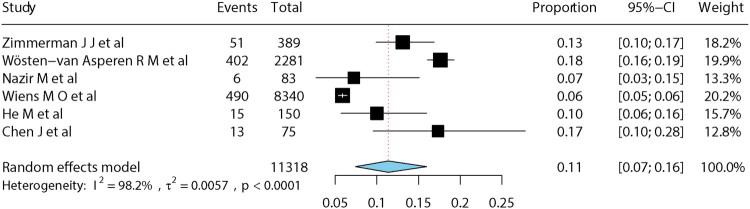 Figure 2
Figure 2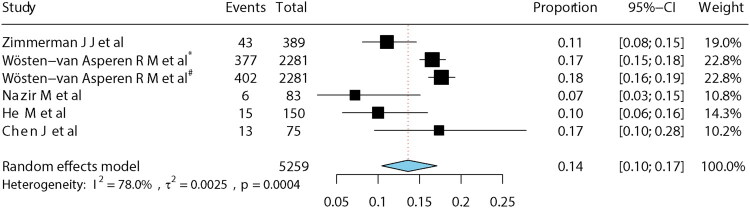 Figure 3
Figure 3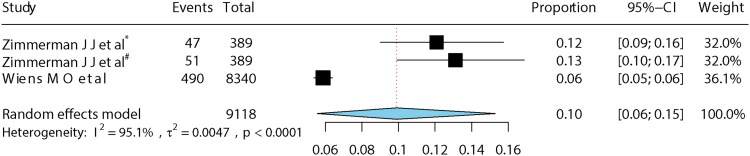 Figure 4
Figure 4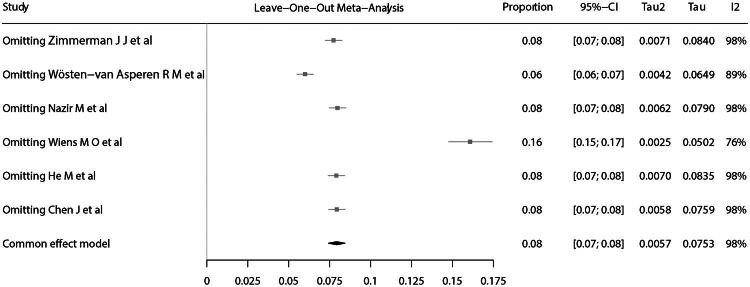 Figure 5
Figure 5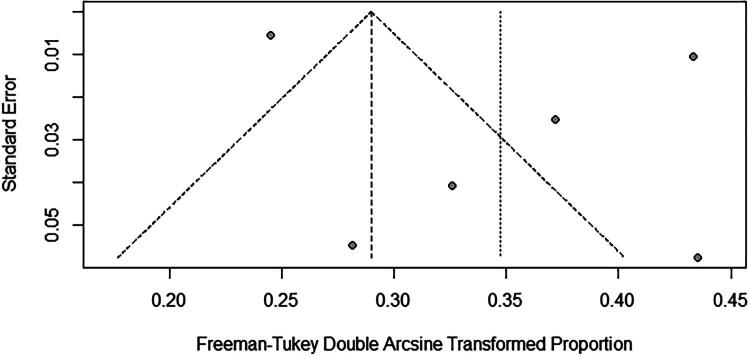 Figure 6
Figure 6| Author/year | Country | Study design | Study period | Multicenter | Sample size | Mortality |
|---|---|---|---|---|---|---|
| Zimmerman J J et al. 2020 [ | USA | Prospective | 2014–2017 | Yes | 389 | 1, 3, 6, and 12 Months |
| Wösten-van Asperen R M et al. 2023 [ | Multinational | Retrospective | 2012–2020 | Yes | 2281 | 1, 2, 3 Months |
| Nazir M et al. 2019 [ | India | Prospective | 2015–2016 | No | 83 | 2 Months |
| Wiens M O et al. 2024 [ | Uganda | Prospective | 2012–2021 | Yes | 8340 | 6 Months |
| He M et al. 2024 [ | China | Retrospective | 2020–2024 | No | 150 | 3 Months |
| Chen J et al. 2024 [ | China | Retrospective | 2015–2021 | No | 75 | 2 months |
- —Guangdong Provincial Key Laboratory of Research on Emergency in TCM
- —National Administration of Traditional Chinese Medicine Innovative Team and Talent Cultivation Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Neonatal and Maternal Infections · Immune Response and Inflammation
Background
Pediatric sepsis is defined as a Phoenix Sepsis Score of at least 2 points with suspected or confirmed infection in children under 18 years, excluding neonates or newborns with a postconceptional age younger than 37 weeks [1]. In 2017, global estimates reported that approximately 25 million children experienced sepsis, resulting in over 3 million fatalities [2]. Recent studies indicate a consistent decline in both the incidence and mortality of sepsis among individuals younger than 14 years from 1990 to 2021 [3]. Specifically, the number of post-neonatal infant cases decreased from 27.1 million in 1990 to 13.3 million in 2021, and the proportion of sepsis-related deaths among neonates declined from 53.9 to 44.4% of all deaths during the same period [3]. The median hospitalization cost per pediatric sepsis case was 7.31 billion, accounting for 18.1% of national pediatric hospitalization costs in 2019 [4]. Despite the case-fatality rates of pediatric severe sepsis and septic shock having declined over time, the fatality rate was higher in the developing countries than in the developed countries during the same period [5]. Nevertheless, many pediatric sepsis survivors demonstrate persistent sequelae clinically manifested by elevated post-discharge healthcare resource utilization [6].
The expanding cohort of pediatric sepsis survivors has engendered heightened clinical focus on their multidimensional long-term health trajectories, particularly encompassing physical, cognitive, and emotional health [7]. A cohort study of critically ill children revealed that 20% of sepsis survivors manifested new-onset or exacerbation of target conditions [8]. In one systematic review, pediatric sepsis survivors are more at risk for cognitive delay, visual impairment, hearing impairment, and cerebral palsy [9]. In addition, the 28-day mortality rate in children with septic shock is reaching 67%, and health-related quality of life decline by greater than 10% occurred in 31.0% children surviving septic shock [10].
Sustainable Development Goal 3.2 seeks to eradicate preventable fatalities of newborns and children under 5 years of age by 2030 [11]. The vast majority of research on pediatric sepsis looked at either 28-day mortality or in-hospital mortality, while the long-term mortality remains unappreciated [12]. However, post-discharge mortality accounted for 50.8% of all pediatric sepsis-related fatalities, with 7.9% of sepsis survivors in the 0–6 month age cohort experiencing mortality following hospital discharge [13]. These finding underscores that pediatric sepsis survivors remain highly vulnerable during the post-discharge period.
Despite emerging studies on long-term mortality after pediatric sepsis, the absence of comprehensive systematic reviews has resulted in fragmented evidence and inadequate synthesis. The purpose of this systematic review and meta-analysis is to estimate the long-term mortality risks associated with pediatric sepsis, providing a basis for optimizing post-discharge surveillance and care protocols.
Methods
This review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines[14] (Supplementary Table 1). The study protocol was registered in PROSPERO (CRD420251137504).
Data sources and search strategy
We systematically searched PubMed, Embase, the Cochrane Library, and Web of Science for studies published from the inception of each database to 30 June, 2025. The search combined Medical Subject Headings (MeSH) and free-text terms using Boolean operators, including terms such as ‘sepsis’, ‘child’, ‘mortality’, and ‘follow-up study’. The full electronic search strategy for each database is provided in Supplementary Table 2.
Inclusion and exclusion criteria
Eligible studies fulfilled all the following criteria: (1) Population: pediatric sepsis patients diagnosed using international consensus definitions [1,15]. (2) Outcome: reporting long-term mortality, defined as mortality at least 30 days after sepsis diagnosis or hospital discharge. (3) Study design: cohort, cross-sectional, or randomized controlled trials in humans.
Studies were excluded if they met all of the following criteria: (1) Focus on adults (≥18 years), preterm neonates (<37 weeks’ gestation at birth), or mixed populations without pediatric-specific data. (2) Lack of extractable data on long-term mortality. (3) Were case reports, reviews, editorials, comments, letters, biographies, books, news items, conference abstracts, expressions of concern, retractions, or animal studies. (4) Duplicate or overlapping reports from the same cohort. (5) Not published in English.
Selection process
After deduplication using EndNote X9, two independent reviewers (YL and JZ) screened titles/abstracts and subsequently assessed full texts for eligibility. Discrepancies were resolved through consultation with a third reviewer (JS).
Data extraction
From each included study, we extracted the following data: first author, publication year, country, population characteristics, study period, research period, follow-up duration, loss-to-follow-up rate, mortality, and data source.
Quality assessment
Study quality was independently evaluated by two reviewers (YL and JZ) using the Newcastle-Ottawa scale (NOS) [16]. Disagreements were adjudicated by a third reviewer (JS). The NOS assessed three domains: selection (0–4 points), comparability (0–2 points), and outcome assessment (0–3 points). For studies lacking comparison groups, a modified NOS (0–6 points) was applied. A NOS score <4 was considered indicative of high risk of bias.
Statistical analyses
All statistical analyses were performed in R (version 4.4.2). Pooled long-term mortality rates were estimated using a meta-analysis of proportions with the meta package [17]. Proportions were transformed using the Freeman-Tukey double arcsine transformation to stabilize variances and improve normality. Heterogeneity was evaluated using Cochran’s Q and I^2^ statistics [18]. Given anticipated heterogeneity, pooled estimates were calculated using a random-effects model.
Results are presented as forest plots showing individual study estimates with 95% confidence intervals (CI) and study weights. To minimize the excessive influence of individual studies on the pooled effect size, sensitivity analysis was conducted by iteratively excluding each study to assess its impact on the pooled estimate. Subgroup analyses were conducted to assess robustness and explore sources of heterogeneity. Publication bias was evaluated by inspection of funnel plot symmetry and quantified with Egger’s test [19].
Results
Study selection
A total of 72,065 records were identified through database searching. After removing 26,676 duplicates, 45,389 articles were excluded based on title and abstract screening. Following full-text review, six studies met eligibility criteria and were included in the meta-analysis. The detailed screening process is shown in Figure 1.
PRISMA flow diagram of study selection.
Study characteristics
The meta-analysis included six studies comprising 11,318 pediatric sepsis patients from diverse regions. Among the included studies, Nazir et al. were the first to prospectively collect 60-day mortality data in children with septic shock in India [20]. Zimmerman et al. conducted a 12-month follow-up multicenter study in the United States between 2013 and 2017 to investigate the long-term mortality trajectories in this population [21]. Wösten-van Asperen and colleagues reported 90-day mortality among pediatric cancer patients with sepsis in a multicenter retrospective cohort study across Europe and the Americas [22]. Wiens et al. performed the largest multicenter prospective study in Uganda involving children under five years of age with suspected sepsis and reported six-month mortality rates [23]. In contrast, the studies by He et al. and Chen et al. were both retrospective studies conducted in China with relatively small sample sizes [24,25]. Key characteristics are summarized in Table 1.
Quality evaluation
Overall study quality was acceptable, with Newcastle-Ottawa Scale (NOS) scores ranging from 4 to 6 (Supplementary Table 3). All studies lost points in the comparability domain and in the selection of a non-exposed cohort because of the absence of suitable control groups. Additionally, certain studies received lower scores due to limited generalizability from highly specific populations and follow-up rates of less than 90%.
Long-term mortality
For the meta-analysis, we used each study’s longest reported follow-up time point. The pooled long-term mortality among pediatric sepsis patients was 11% (95% CI: 7–16%). Substantial heterogeneity was present (I^2^ = 98.2%, p < 0.001) (Figure 2).
Forest plot of pooled long-term mortality in pediatric sepsis.
Sensitivity analysis and publication bias
Because follow-up duration varied across studies, subgroup analyses were performed for studies with follow-up ≤3 months and those with follow-up of 6–12 months. The pooled long-term mortality was 14% (95% CI: 10–17%) for follow-up ≤3 months and 10% (95% CI: 6–15%) for follow-up of 6–12 months (Figures 3 and 4). In leave-one-out sensitivity analysis, exclusion of one study [23] reduced heterogeneity but increased pooled mortality to 16% (15–17%) (Figure 5). The funnel plot showed a slight asymmetry (Figure 6), while Egger’s test (p = 0.39) suggested no potential publication bias.
*Mortality at 1–3 months. Note: Mortality in 2 months, #mortality in 3 months
*Mortality at 6–12 months. Note: Mortality in 6 months, #mortality in 12 months.
Leave-one-out sensitivity analysis.
Funnel plot.
Discussion
To our knowledge, this is the first meta-analysis to quantify long-term mortality after pediatric sepsis. Our pooled estimate of 11% (95% CI: 7–16%) post-discharge mortality highlights a clinically significant burden, with rates remaining broadly consistent across follow-up durations despite inter-study variability.
Long-term outcomes after hospital discharge remain an important but often underappreciated aspect of sepsis care. More than one-sixth of pediatric sepsis survivors are rehospitalized within 30 days, compared with about one in five among adult sepsis survivors [26,27]. In low-middle-income countries, nearly 50% of discharged children die within 6 months, with over half occurring outside healthcare facilities [28,29]. Reported post-acute mortality among adult sepsis survivors was 16.1%, higher than the pooled estimate for children in our analysis [30]. These findings collectively underscore persistent vulnerabilities among sepsis survivors, irrespective of age.
The drivers of post-discharge mortality in pediatric sepsis are multifactorial, including discharges against medical advice, residual underlying conditions, risky home environments, limited caregiver resources, and fragile healthcare infrastructure impeding follow-up care [29,31,32]. Mechanistic studies in adults reveal a persistent increase of inflammatory and immunosuppressive biomarkers correlating with late mortality [33], yet equivalent pediatric investigations remain scarce. The long-term physical, cognitive, and psychosocial sequelae in children have received less attention than in adults. Recent international guidance for adult sepsis increasingly emphasizes post-discharge assessment and follow-up, while such recommendations are notably lacking in pediatric sepsis guidelines [34]. Therefore, there is an urgent need to strengthen clinical care and follow‑up for pediatric sepsis survivors, aiming to reduce preventable post‑discharge deaths and other adverse outcomes.
This study is limited by several factors. First, limited studies precluded extensive subgroup analyses. Second, substantial heterogeneity inherent to proportional meta-analyses complicates generalizability [35]. Third, the absence of control cohorts restricts conclusions to associative observations, rather than causal inference or direct comparison to non-sepsis pediatric populations. Fourth, although funnel plot and Egger’s test showed no significant bias, its reliability is limited to fewer than 10 studies, and English-language restrictions may exclude relevant data, potentially leading to publication bias.
Conclusion
This systematic review and meta-analysis identified an 11% long-term mortality rate following pediatric sepsis, underscoring the persistent risk of mortality after hospital discharge. High-quality longitudinal studies are urgently needed to determine modifiable risk factors and to inform improvements in evidence-based follow-up and individualized care.
Supplementary Material
Supplementary material.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schlapbach LJ, Watson RS, Sorce LR, et al. International consensus criteria for pediatric sepsis and septic shock. JAMA. 2024;331(8):665–674. doi: 10.1001/jama.2024.0179.38245889 PMC 10900966 · doi ↗ · pubmed ↗
- 2Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–211. doi: 10.1016/s 0140-6736(19)32989-7.31954465 PMC 6970225 · doi ↗ · pubmed ↗
- 3Collaborators GGS. Global, regional, and national sepsis incidence and mortality, 1990–2021: a systematic analysis. Lancet Glob Health. 2025;13(12):e 2013–e 26. doi: 10.1016/s 2214-109x(25)00356-0.41135560 · doi ↗ · pubmed ↗
- 4Carlton EF, Barbaro RP, Iwashyna TJ, et al. Cost of pediatric severe sepsis hospitalizations. JAMA Pediatr. 2019;173(10):986–987. doi: 10.1001/jamapediatrics.2019.2570.31403673 PMC 6692673 · doi ↗ · pubmed ↗
- 5Tan B, Wong JJ-M, Sultana R, et al. Global case-fatality rates in pediatric severe sepsis and septic shock: a systematic review and meta-analysis. JAMA Pediatr. 2019;173(4):352–362. doi: 10.1001/jamapediatrics.2018.4839.30742207 PMC 6450287 · doi ↗ · pubmed ↗
- 6Maddux AB, Zimmerman JJ, Banks RK, et al. Health resource use in survivors of pediatric septic shock in the United States. Pediatr Crit Care Med. 2022;23(6):e 277–e 88. doi: 10.1097/pcc.0000000000002932.35250001 PMC 9203867 · doi ↗ · pubmed ↗
- 7Minogue J, Schlapbach LJ, Keogh S, et al. Long-term outcomes after paediatric sepsis (LOTUS)-a protocol for an Australian cohort study. Nurs Crit Care. 2024;29(2):438–443. doi: 10.1111/nicc.12938.37300332 · doi ↗ · pubmed ↗
- 8Carlton EF, Gebremariam A, Maddux AB, et al. New and progressive medical conditions after pediatric sepsis hospitalization requiring critical care. JAMA Pediatr. 2022;176(11):e 223554. doi: 10.1001/jamapediatrics.2022.3554.36215045 PMC 9552050 · doi ↗ · pubmed ↗