‘Cough and sneeze into your elbow’: a field study testing the effects of persuasive messages on compliance with behavioral measures to prevent the spread of respiratory viruses
Amy van der Heijden, Anne Vos, John de Wit, Daniëlle Timmermans, Bas van den Putte

TL;DR
This study examines how persuasive messages influence people's compliance with behaviors like coughing into the elbow and staying home when sick to prevent respiratory virus spread.
Contribution
The study provides empirical evidence on how different message framings affect behavioral compliance with pandemic prevention measures.
Findings
Persuasive messages positively influenced behavioral determinants like intention and self-efficacy.
Compliance with staying home when ill had lower odds compared to coughing/sneezing into the elbow.
Demographic and psychological factors significantly affected compliance outcomes.
Abstract
Effective persuasive messages can contribute to enhancing pandemic preparedness and public health. An essential requirement for this is an excellent understanding of the effects of exposure to persuasive messages on compliance with behavioral measures against the spread of respiratory viruses. This field study tested the effects of persuasive messages on compliance with two behavioral measures to prevent the spread of viruses that cause respiratory infections such as COVID-19 and the flu: coughing/sneezing into the elbow and staying home when ill with respiratory infection symptoms. A field study with an observational pre-post design was conducted at four educational institutions representing all common post-secondary school educational levels in the Netherlands. Data were collected among students and employees via online questionnaires before (n = 2096) and after (n = 1098) exposure…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1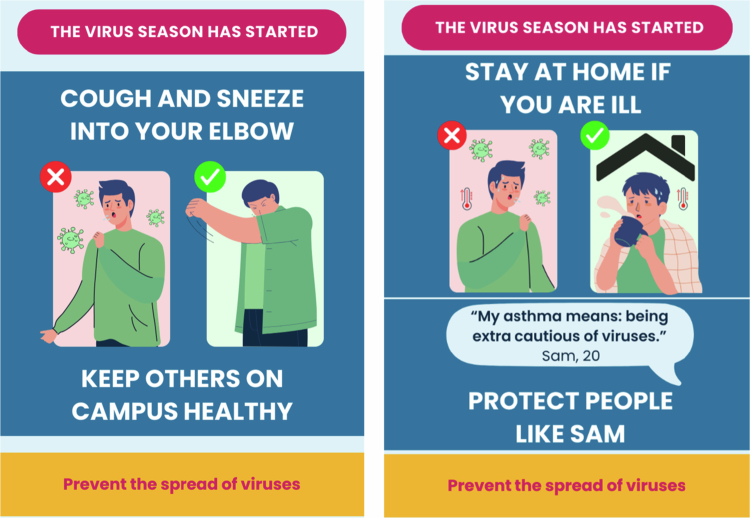 Figure 2
Figure 2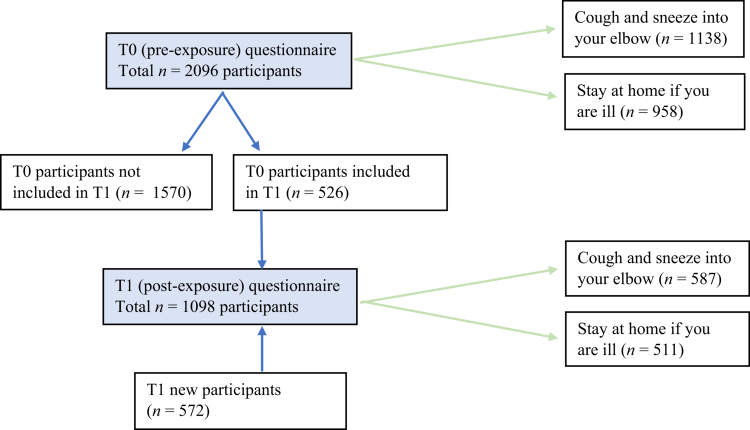 Figure 3
Figure 3| T0 (pre-exposure) | Role | Gender | Age ( | Ethnic background1
|
|---|---|---|---|---|
| Total ( | Student: 1922 (91.7%) | Men: 552 (26.3%) | Netherlands: 829 (39.6%) | |
| University A( | Student: 1267 (95.3%) | Men: 314 (23.6%) | Netherlands: 356 (26.8%) | |
| University B ( | Student: 353 (90.5%) | Men: 116 (29.7%) | Netherlands: 206 (52.8%) | |
| University of applied sciences ( | Student: 192 (75.9%) | Men: 74 (29.2%) | Netherlands: 179 (70.8%) | |
| Intermediate vocational education ( | Student: 110 (88.7%) | Men: 48 (38.7%) | Netherlands: 88 (71.0%) | |
| T1 (post-exposure) | Role | Gender | Age ( | Ethnic background1
|
| Total ( | Student: 751 (68.4%) | Men: 257 (23.4%) | Netherlands: 565 (51.5%) | |
| University A ( | Student: 454 (83.5%) | Men: 128 (23.5%) | Netherlands: 173 (31.8%) | |
| University B ( | Student: 170 (60.7%) | Men: 62 (22.1%) | Netherlands: 184 (65.7%) | |
| University of applied sciences ( | Student: 72 (34.1%) | Men: 50 (23.7%) | Netherlands: 160 (75.8%) | |
| Intermediate vocational education ( | Student: 55 (87.3%) | Men: 17 (27.0%) | Netherlands: 48 (76.2%) |
| Exposure frequency | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 times ( | 1–2 times ( | 3–4 times ( | 5 + times ( | ||||||||
| M | (SD) | M | (SD) | M | (SD) | M | (SD) |
| ηp2 | ||
| Intention | 3.51 | 1.23 | 3.79 | 1.20 | 3.66 | 1.29 | 3.66 | 1.21 | 1.98 | .116 | .005 |
| Attitude | 4.14 | 0.81 | 4.20 | 0.84 | 4.13 | 0.80 | 4.04 | 0.90 | 2.03 | .108 | .006 |
| Social norm |
| 0.92 |
| 0.83 |
| 0.83 | 3.20 | 0.89 | 2.77 | .041 | .008 |
| Moral norm | 3.30 | 1.10 | 3.51 | 1.04 | 3.48 | 0.98 | 3.36 | 1.03 | 2.38 | .068 | .006 |
| Self-efficacy | 3.51 | 1.18 | 3.77 | 1.06 | 3.60 | 1.17 | 3.59 | 1.11 | 2.19 | .088 | .006 |
| Response efficacy | 4.36 | 0.79 | 4.41 | 0.74 | 4.42 | 0.71 | 4.37 | 0.72 | 0.62 | .604 | .002 |
| Perceived risk COVID-19 |
| 0.61 |
| 0.55 |
| 0.62 | 3.05 | 0.62 | 5.04 | .002 | .014 |
| Perceived risk flu |
| 0.58 |
| 0.53 |
| 0.57 | 2.92 | 0.53 | 3.97 | .008 | .011 |
| Exposure frequency | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 times ( | 1–2 times ( | 3–4 times ( | 5 + times ( | Total ( | |||||||||
| M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | ||||
|
| |||||||||||||
| Intention | 4.17 | 1.01 | 4.23 | 1.05 | 4.40 | 0.89 | 4.18 | 1.04 | 4.23 | 1.00 | |||
| Attitude | 4.55 | 0.67 | 4.50 | 0.68 | 4.53 | 0.63 | 4.42 | 0.76 | 4.52 | 0.68 | |||
| Social norm | 3.25 | 0.91 | 3.45 | 0.78 | 3.51 | 0.73 | 3.42 | 0.77 | 3.36 | 0.84 | |||
| Moral norm | 3.48 | 1.02 | 3.69 | 1.00 | 3.70 | 0.92 | 3.53 | 0.99 | 3.57 | 1.00 | |||
| Self-efficacy | 4.33 | 0.67 | 4.31 | 0.71 | 4.34 | 0.77 | 4.21 | 0.69 | 4.31 | 0.70 | |||
| Response efficacy | 4.20 | 0.80 | 4.28 | 0.74 | 4.28 | 0.76 | 4.29 | 0.73 | 4.24 | 0.77 | |||
| Perceived risk COVID-19 | 2.93 | 0.64 | 3.07 | 0.53 | 3.17 | 0.61 | 3.07 | 0.61 | 3.02 | 0.61 | |||
| Perceived risk flu | 2.85 | 0.57 | 3.03 | 0.53 | 3.06 | 0.57 | 2.97 | 0.53 | 2.94 | 0.56 | |||
|
| |||||||||||||
| Intention |
| 1.05 |
| 1.15 |
| 1.14 | 2.92 | 1.06 | 2.90 | 1.09 | |||
| Attitude | 3.72 | 0.72 | 3.81 | 0.86 | 3.66 | 0.71 | 3.50 | 0.79 | 3.70 | 0.76 | |||
| Social norm | 2.94 | 0.90 | 3.01 | 0.82 | 3.02 | 0.87 | 2.90 | 0.96 | 2.97 | 0.89 | |||
| Moral norm | 3.11 | 1.14 | 3.27 | 1.04 | 3.21 | 0.99 | 3.12 | 1.05 | 3.16 | 1.09 | |||
| Self-efficacy |
| 0.97 |
| 1.02 |
| 0.94 |
| 0.99 | 2.75 | 0.98 | |||
| Response efficacy | 4.53 | 0.75 | 4.57 | 0.70 | 4.59 | 0.61 | 4.48 | 0.70 | 4.55 | 0.71 | |||
| Perceived risk COVID-19 | 2.94 | 0.58 | 3.04 | 0.58 | 3.02 | 0.64 | 3.03 | 0.63 | 2.98 | 0.60 | |||
| Perceived risk flu | 2.87 | 0.58 | 2.94 | 0.54 | 2.90 | 0.56 | 2.86 | 0.54 | 2.89 | 0.57 | | | |
|
|
|
| |||||||||||
| Intention | 319.70 | <.001** | 0.227 | ||||||||||
| Attitude | 272.65 | <.001** | 0.200 | ||||||||||
| Social norm | 52.30 | <.001** | 0.046 | ||||||||||
| Moral norm | 33.21 | <.001** | 0.030 | ||||||||||
| Self-efficacy | 656.26 | <.001** | 0.376 | ||||||||||
| Response efficacy | 28.56 | <.001** | 0.026 | ||||||||||
| Perceived risk COVID-19 | 1.67 | .196 | 0.002 | ||||||||||
| Perceived risk flu | | | | | | | | | | 4.86 | .028* | 0.004 | |
|
|
|
| |||||||||||
| Intention | 2.84 | .037* | .008 | ||||||||||
| Attitude | 0.96 | .412 | .003 | ||||||||||
| Social norm | 0.94 | .422 | .003 | ||||||||||
| Moral norm | 0.16 | .926 | .000 | ||||||||||
| Self-efficacy | 2.94 | .032* | .008 | ||||||||||
| Response efficacy | 0.33 | .805 | .001 | ||||||||||
| Perceived risk COVID-19 | 0.95 | .418 | .003 | ||||||||||
| Perceived risk flu | 1.45 | .228 | .004 | ||||||||||
| Moderator |
| Wilks' Λ | |
|---|---|---|---|
| Educational institution (university; uni. of appl. sciences; interm. voc. edu.) | <.001** | 0.959 | |
| Role (student or employee) | <.001** | 0.963 | |
| Participation in T0 (yes or no) | =.007** | 0.981 | |
| Gender (man or woman) | <.001** | 0.957 | |
| Age (16–24; 25–39; 40–59; 60 + years) | <.001** | 0.942 | |
| Ethnic background (Netherlands; Non-western migration background; Western migration background) | <.001** | 0.913 | |
| Knowledge of respiratory viruses and preventive measures (low or high) | <.001** | 0.939 | |
| Trust in government (low or high) | =.015* | 0.983 | |
| Prosocial orientation (self or others) | <.001** | 0.967 | |
| Perceived health status (bad or good) | <.001** | 0.944 |
| Moderator | Outcome measureb |
|
| Effect specification | |||
|---|---|---|---|---|---|---|---|
| Educational institution (university; uni. of appl. sciences; interm. voc. edu.) | Social norm | .003** | 0.011 | Interm. voc. edu. ( | |||
| Gender (man or woman) | Intention | <.001** | 0.010 | Women ( | |||
| Gender × exposure frequency (man or woman; 0, 1–2, 3–4, 5+ times) | Intention | .005** | 0.012 | Women: | |||
| Age (16–24; 25–39; 40–59; 60+ years) | Social norm | .022* | 0.009 | Aged 16–24 years ( | |||
| Ethnic background (Netherlands; Non-western migration background; Western migration background) | Social norm | .002** | 0.011 | Netherlands ( | |||
| Ethnic background * exposure frequency (Netherlands; Non-western migration background; Western migration background; 0, 1–2, 3–4, 5+ times) | Perc. risk COVID-19 | .005** | 0.017 | Netherlands: | |||
| Role (student or employee) | Intention | .003** | 0.008 | Employee ( | |||
| Participation in T0 (yes or no) | Moral norm | .036* | 0.004 | Yes ( | |||
| Knowledge of respiratory viruses and preventive measures (low or high) | Intention | .006** | 0.007 | High ( | |||
| Trust in government (low or high) | Response efficacy | <.001** | 0.012 | High ( | |||
| Prosocial orientation (self or others) | Response efficacy Perc. risk COVID-19 | .007** | 0.007 | Other-oriented ( | |||
| Perceived health status (bad or good) | Perc. risk COVID-19 | <.001** | 0.037 | Bad ( | |||
| Independent variablea |
|
| OR (95% CI) |
|---|---|---|---|
| Exposed 0 times | 1.00 | ||
| Constant | 0.36 (0.12) | .002 | 1.432 |
| Exposed 1-2 times | 0.12 (0.20) | .544 | 1.129 (0.764, 1.667) |
| Exposed 3-4 times | 0.33 (0.20) | .103 | 1.393 (0.935, 2.076) |
| Exposed 5+ times | −0.06 (0.24) | .794 | 0.939 (0.587, 1.504) |
| Low-risk situation intention (current situation, T1) | Hypothetical high-risk situation intention | ||||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M difference |
| ||
|
|
| 1.00 |
| 0.78 | 0.11 | .005 | |
|
|
| 1.09 |
| 0.97 | 0.73 | <.001 | |
|
|
| 1.24 |
| 0.94 | | ||
| |
|
|
| ||||
|
| 112.99 | <.001** | 0.093 | ||||
- —ZonMw10.13039/501100001826
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBehavioral Health and Interventions · Psychology of Social Influence · Vaccine Coverage and Hesitancy
Introduction
The COVID-19 pandemic had major impact on societies worldwide. The World Health Organization (WHO) reported that 776 million people globally became infected with the coronavirus since the start of the outbreak in late 2019, resulting in the death of over 7 million people. In Europe, the cumulative number of infections and deaths is 280 million and over 2 million, respectively (WHO, 2024). The pandemic put a lot of pressure on healthcare systems (Trentini et al., 2022; Van Giessen et al., 2020), posed a large economic burden (Faramarzi et al., 2024; Richards et al., 2022), and had major impact on individuals' mental health (COVID-19 Mental Disorders Collaborators, 2021).
Behavioral and environmental measures were implemented by governments across countries in attempts to curb the number of infections, including physical distancing, wearing face masks, regular and appropriate hand washing, self-isolation, and closing public institutions and buildings such as schools and work places (e.g. Talic et al., 2021). It is shown that combinations of implemented measures in the Netherlands were effective in reducing the number of infections, while acknowledging that the effectiveness of each individual measure is difficult to specify, and while also concluding that people's compliance with behavioral measures is essential for their effectiveness (Wallinga et al., 2024).
Prior research investigated effects of various types of communication strategies, such as different ways of framing, on behavioral determinants and compliance with COVID-19 preventive measures (e.g. Gillman et al., 2022; Hong & Hashimoto, 2021; Jiang & Amponsah Dodoo, 2021). A recent literature review showed that communication can have a major impact on compliance, but that several strategies had mixed effects (Williams et al., 2023). The review also noted that communication is itself a multi-faceted construct which makes it difficult to separate the impact of any one communication strategy, and to distinguish the effects of communication from voluntary and enforced behavioral recommendations and changes in the physical environment (Williams et al., 2023).
Prior research also explored effects of repeated exposure to information on behavioral determinants. Exposure to messages more frequently than desirable can lead to message fatigue, i.e. exhaustion and boredom after prolonged and repeated exposure to similar messages over time (So et al., 2016). While exposure to messages is essential to induce changes in determinants and behavior (Hornik, 2002), the relationship between message exposure and behavioral determinants is shown to take an inverted U-shape (So et al., 2016). More frequent exposure first leads to an increase, and then a decrease in behavioral determinants such as intention to perform specific behaviors. The optimal exposure length and frequency are still opaque. Meanwhile, health communication studies have shown that message fatigue may indeed induce resistance to promoted behavioral measures such as COVID-19 vaccine uptake (Cho & Salmon, 2007; Okuhara et al., 2023; Shen et al., 2022; Skurka & Keating, 2024; Zhao et al., 2023).
Although prior studies provided essential insights into the effects of various communication strategies, they were typically conducted in controlled environments such as online settings or labs. Evidence on effects of persuasive messages on compliance with measures to prevent respiratory virus spread in real-life practice is scarce, yet indispensable to enhance pandemic preparedness. Some field studies have been conducted, and these provide indications regarding if and how persuasive communication can enhance compliance in real life. For instance, a field study on a university campus in the Netherlands showed that interventions arousing empathy may enhance physical distancing (De Ridder et al., 2021). Another field study in the Netherlands showed that nudging and boosting effectively improved hand hygiene compliance in hospital nurses (Van Roekel et al., 2021). Although these prior studies are informative, the evidence base remains scarce. This is especially the case considering that each prior study deployed different intervention and communication strategies, targeting different behaviors among different study populations and in different contexts. A comprehensive understanding of the effects of exposure to persuasive messages on compliance with measures to prevent the spread of respiratory viruses in real-life is lacking, yet essential to effectively enhance pandemic preparedness.
This study
The present study addresses this critical knowledge gap by exploring the effects of exposure to persuasive messages in real-life educational settings on (behavioral determinants of) compliance with two behavioral measures to prevent the spread of viruses that cause respiratory infections, notably: coughing and sneezing into the elbow, and staying home when ill with respiratory infection symptoms. These measures continue to be advised by the Dutch government in the current low-risk pandemic context to prevent the spread of a range of respiratory viruses, including COVID-19 and the flu (Government of the Netherlands, n.d.). Compliance and behavioral determinants were measured before and after exposure to persuasive messages about the two measures. Compliance with these behavioral measures following exposure to persuasive messages in a hypothetical high-risk pandemic situation was also explored.
The following hypotheses and exploratory research questions are addressed:
H1. Participants who are more frequently exposed to persuasive messages have a higher intention to comply with behavioral measures than participants who are less frequent or not exposed.
H2. Participants who are more frequently exposed to persuasive messages comply with behavioral measures more often than participants who are less frequent or not exposed.
RQ1. To what extent does the effect of more frequent exposure to persuasive messages (vs. less frequent or no exposure) on intention to comply with behavioral measures and other behavioral determinants differ as a function of:
- behavioral measure (coughing and sneezing into the elbow, or staying home when ill with respiratory infection symptoms)?
- educational institution (research university, university of applied sciences, intermediate vocational education), and role (student or employee)?
- demographic characteristics: age, gender, and ethnic background?
- personal characteristics: trust in government, prosocial orientation, perceived health status, and knowledge of respiratory viruses and preventive measures?
RQ2. To what extent do changes in intention and other behavioral determinants between pre- and post-exposure measurement differ as a function of exposure frequency?
RQ3. To what extent does participants' intention to comply with behavioral measures following exposure to persuasive messages in a hypothetical high-risk pandemic situation, differ from their intention to comply in the current low-risk situation?
Materials and methods
Study design, procedures and participant eligibility
A field study with an observational pre-post design was conducted at two research universities, a university of applied sciences, and an intermediate vocational education institution in the Netherlands. Data were collected from students and employees in November–December 2023 via self-administered online questionnaires before (pre-exposure, T0) and after (post-exposure, T1) exposure to persuasive messages about coughing and sneezing into the elbow, and staying home when ill with respiratory infection symptoms (Figure 1). Messages were disseminated simultaneously in Dutch and English, digitally and physically, via participating educational institutions' newsletters, websites, apps for students and staff, and in educational buildings via narrowcasting screens, billboards in elevators, and bulletin boards. Links to the questionnaires were distributed via the same channels, and by on-site by research assistants who asked students and employees in the educational buildings to participate via a QR-code. Participants at the research universities and the university of applied sciences were randomly allocated to answer questions related to either of the two behavioral measures. Participants at the intermediate vocational education institution only received questions about coughing and sneezing into the elbow, as they were also only exposed to messages about this measure, per request of the educational institution.
*Field study design. Note: The time frame for filling in the T0 and T1 questionnaires at the intermediate vocational education institution was one rather than two weeks, due to limited time to conduct the study at this institution.
Participants were eligible when they were ≥16 years of age and affiliated as either student or employee with one of the participating educational institutions. No other exclusion criteria were applied. Participants received either study credits, entry to a gift voucher lottery, or a snack, depending on institution and role. Students and employees were encouraged to participate in both the pre- and post-exposure surveys, but could also complete only one (or none). Therefore, participants in T1 included individuals who completed both T0 and T1, as well as those who only participated in T1. A sample size calculation using G*Power (Faul et al., 2009) indicated that 1000 participants per measurement point were required to detect a small effect size of .10 at the standard .05 alpha error probability and a power of ß = .80.
Informed consent was obtained digitally on the first page of the questionnaire, which provided detailed study information and contact details of the researchers. The study was pre-registered at the Open Science Framework (Van der Heijden et al., 2023b), and approved by the Faculty Ethics Review Board of the Faculty of Social and Behavioral Sciences, University of Amsterdam (reference number FMG-4416).
Materials: persuasive messages
Six persuasive messages were designed in a poster format (Figure 2 and Supplementary File 1). Three messages related to coughing/sneezing into the elbow, and three to staying home when ill. Messages conveyed either risk information about (non-)compliance (the risk of non-compliance and the risk reduction of compliance), positive social outcomes of compliance (keeping others on campus healthy), or aimed to arouse empathy for vulnerable people on campus (protect people with fragile health). All posters had the same layout that stated the health hazard on top (‘the virus season has started’), followed by directions to comply with one of the two behavioral measures (either cough and sneeze into your elbow, or stay at home if you are ill), accompanied by a visualization. Then one of the three persuasive strategies followed (risk information, positive social outcomes, or arousing empathy), and finally the main goal was stated at the bottom of the poster (‘prevent the spread of viruses’).
Examples of the posters conveying persuasive messages.
Message phrasing and poster design were done in consultation with policy and communication staff from the Netherlands Ministry of Public Health, Welfare and Sports, to ensure close resemblance to messages used in practice by the government during the COVID-19 pandemic, and to maximize potential practical usability in the future. Students from one of the participating educational institutions also provided input via informal review to ensure message understandability and attractiveness. The three persuasive information strategies in the messages were selected based on the results of an online experiment conducted prior to the field study in which seven information types were tested (manuscript in preparation; study publicly pre-registered at the Open Science Framework (Van der Heijden et al., 2023a)).
Measures
Variables were measured at both the pre- and post-exposure questionnaires, unless noted otherwise. A complete overview of all measures, including example items and substantiation, is included in Supplementary File 2. Recall of exposure frequency (measured only post-exposure; pragmatically categorized as 0, 1–2, 3–4, or 5+ times exposed) was the main independent variable. Outcome measures were assessed using five-point Likert scales or semantic differential scales (unless otherwise indicated) and encompassed intention to comply with the allocated behavioral measure; attitude, social norms, moral norm, self-efficacy, and response efficacy regarding the behavioral measure; actual compliance with this measure (answer options dichotomized into ‘compliant’ or ‘not compliant’); and perceived risk of COVID-19 and the flu. Intention to comply with the behavioral measure in a hypothetical high-risk pandemic situation was also assessed at the post-exposure questionnaire.
Assessed potential effect modifiers included trust in government, prosocial orientation (self- or other-oriented), perceived health status, knowledge of respiratory viruses and preventive measures (six statements that could be answered with ‘true’, ‘not true’ and ‘don’t know’), demographic characteristics (gender, age, ethnic background), educational institution, role (student/employee), behavioral measure type the participant was allocated to in the questionnaire, and whether the participant completed both T0 and T1 questionnaires or only T1.
Data analysis
Outcome measures and effect modifiers were included as continuous variables (scale scores comprised the mean of scale items), except behavioral compliance which was categorical (compliant or not). For knowledge, the sum of correct answers was used. Effect modifiers were dichotomized before inclusion in the analyzes or otherwise categorized (all categories displayed in results tables). Reliability of all multi-item scales was established for all measures assessed with Likert or semantic differential response scales. All showed sufficient internal consistency, Cronbach's α ranging from .721 to .937.
Two-way multivariate analyzes of variance (MANOVA) were conducted to test the main effect of exposure frequency to persuasive messages on intention to comply (main outcome) and other behavioral determinants at T1, including the potential interaction effect with behavioral measure type. Interaction effects with other potential effect modifiers were examined through eleven additional MANOVAs. Logistic regression analysis assessed whether behavioral compliance at T1 was related to exposure frequency. Repeated measures ANOVA compared participants' intention to comply in the present low-risk pandemic situation (T1) to their anticipated intention to comply in a hypothetical high-risk situation. For participants who completed both T0 and T1, repeated measures MANOVA explored the extent to which changes in intention and behavioral determinants between T0 and T1 differed as a function of exposure frequency. Behavioral measure type was included as covariate in all analyzes. All analyzes were conducted using data of participants without any missing values on the relevant variables. Due to forced responses in the questionnaires (i.e. participants could only proceed after providing an answer to the previous question), there were very few missing variables per questionnaire.
Effects were considered statistically significant at p < .05. If a multivariate main or interaction effect on the combined outcome measures was found, this effect was further explored with univariate analyzes of the individual outcome measures. Due to space limitations, concise results are presented. Full information on all models, including descriptives and test statistics, is included in Supplementary File 3.
Results
Participant characteristics
Characteristics of participants who completed the pre- (T0, n = 2096) and post-exposure (T1, n = 1098) questionnaires are shown in Table 1, stratified by educational institution. Of the T1 participants, n = 572 participated only at T1; n = 526 had also participated at T0. Of the participants who completed both questionnaires, n = 197 answered questions about the same behavioral measure at both times (randomly allocated). Figure 3 displays the participant flow and allocation to behavioral measures in the T0 and T1 questionnaires. The majority of participants were women (74.1% at T1), students (68.4% at T1), and 16–24 years of age (63.0% at T1). Just over half of participants at T1 (51.5%) had a Dutch background, 28.7% had a background from another Western country, and 19.5% had a background from a non-Western country. The composition of participants regarding age groups and ethnic background was significantly different in T1 compared to T0 (both p's < .001), while the composition of participants regarding gender remained marginally stable (p = .051).
Participant flow and allocation to behavioral measures in the T0 and T1 questionnaires.
Associations between exposure frequency, intention to comply, and behavioral determinants
MANOVA was conducted to test hypothesis 1. Exposure frequency (IV) had a significant multivariate main effect on the combined outcome measures, F(24, 3150) = 2.01, p = .002; Wilks' Λ = 0.957. Univariate effects showed significant effects of exposure frequency on social norm (F(3, 1093) = 2.77, p = .041, = .008) and perceived risk of COVID-19 (F(3, 1093) = 5.04, p = .002, = .014) and the flu (F(3, 1093) = 3.97, p = .008, = .011), but not on intention to comply with the behavioral measures (F(3, 1093) = 1.98, p = .116, = .005) (Table 2). Hypothesis 1, that participants who are more frequently exposed to persuasive messages would have a relatively higher intention to comply, is thus not supported by the findings.
Behavioral measure type was included in the analysis as a potential effect modifier. The analysis revealed a significant multivariate main effect of behavioral measure type on the combined outcome variables: scores for coughing/sneezing into the elbow were consistently higher than for staying home when ill, F(8, 1083) = 111.61, p < .001; Wilks' Λ = 0.548. Univariate analyzes showed significant effects of behavioral measure type on all individual outcomes (all *p'*s < .05), except perceived risk of COVID-19 (p = .196) (Table 3). No significant interaction between exposure frequency and behavioral measure type on the combined outcome variables was identified, F(24, 3141) = 1.31, p = .142; Wilks' Λ = 0.972. However, as also shown in Table 3, exposure frequency only significantly impacted individual outcomes within the behavioral measure staying home when ill, and not within coughing/sneezing into the elbow.
Furthermore, regarding univariate effects on individual outcomes (also shown in Table 3), it should be noted that although both the main effects of behavioral measure type and some of the interaction effects with exposure frequency on individual outcomes are statistically significant, their strengths differ. The large effect size for behavioral measure type (e.g. = .227 for intention) suggests a substantial effect, whereas the small effect size for the interaction between exposure frequency and behavioral measure type (e.g. = .008 for intention) suggests a weak effect.
Main and interaction effects of potential effect modifiers
To explore research question 1, MANOVAs were performed with exposure frequency and each respective potential effect modifier as IVs in the analyzes, including behavioral measure type as a covariate. All potential effect modifiers showed multivariate main effects on the combined outcomes (all p's < .05) (Table 4). Moreover, univariate analyzes of each potential effect modifier on the individual outcomes (Table 5) showed a significant effect of gender, i.e. women had higher scores than men on almost all behavioral determinants: intention (F(1, 1062) = 11.21, p < .001, = .010), attitude (F(1, 1062) = 7.41, p = .007, = .007), moral norm (F(1, 1062) = 5.77, p = .016, = .005), perceived risk of COVID-19 (F(1, 1062) = 24.88, p < .001, = .023), and perceived risk of the flu (F(1, 1062) = 30.79, p < .001, = .028). Furthermore, ethnic background significantly impacted social and moral norm, as participants with a Dutch background had lower social norm (F(2, 1081) = 6.20, p = .002, = .011) and moral norm scores (F(2, 1081) = 10.57, p < .001, = .019) than participants with migration backgrounds. Moreover, participants with a non-western migration background perceived a higher risk of COVID-19 (F(2, 1081) = 21.30, p < .001, = .038) and the flu (F(2, 1081) = 25.22, p < .001, = .045) than people of other backgrounds.
No multivariate interaction effects were identified between exposure frequency and any of the potential effect modifiers on the combined outcomes (all p's > .05). Univariate analyzes showed limited interaction effects between exposure frequency and potential effect modifiers on individual outcomes (Table 5). Intention to comply was significantly higher among women who were exposed five or more times than for women who were not exposed. For men, intention to comply was higher when exposed one or two times, compared to less or more times (F(3, 1062) = 4.34, p = .005, = .012). Among participants with Dutch and non-western migration backgrounds, perceived risk of COVID-19 and the flu was higher when exposed more frequently, compared to less or no exposure (COVID-19 F(6, 1081) = 3.10, p = .005, = .017, flu F(6, 1081) = 2.42, p = .025, = .013), although for participants with a Dutch background there was no significant difference between those who were exposed five times or more versus those who were not exposed.
Behavioral compliance as a function of exposure frequency and behavioral measure type
To test hypothesis 2, logistic regression analysis was conducted with exposure frequency as independent variable, compliance with either of the behavioral measures as outcome, and behavioral measure type as covariate. The analysis showed no significant association between compliance with behavioral measures and exposure frequency (all p's > .05) (Table 6). Hypothesis 2, that participants who are more frequently exposed to persuasive messages comply with behavioral measures more often than participants who are less frequent or not exposed, is not supported by the findings. However, the analysis showed a significant association between compliance and behavioral measure type. Participants were more likely to comply with coughing/sneezing into the elbow than with staying home when ill, OR = 0.165, 95% CI [0.117, 0.233]. Thus, the odds of compliance with staying home when ill were 83.5% lower compared to coughing and sneezing into the elbow.
Changes over time in intention to comply and behavioral determinants
Repeated measures MANOVA was conducted with data from participants who completed the questionnaire at both T0 and T1, to explore research question 2. With exposure frequency as between-subjects factor, time (T0 or T1) as within-subjects factor, and behavioral measure type as covariate, the analysis showed a significant multivariate main effect of time on the combined outcomes, indicating changes in the outcomes from pre- to post-exposure (F(8, 185) = 3.15, p = .002; Wilks' Λ = 0.880). There was no significant interaction effect between time and exposure frequency on the combined outcomes, F(24, 537.158) = 1.17, p = .266; Wilks' Λ = 0.863. Univariate analyzes showed a significant main effect of time on intention to comply (decreasing from T0 to T1, F(1, 192) = 5.877, p = .016) and social norm (decreasing from T0 to T1, F(1, 192) = 17.332, p < .001). Thus, intention to comply and social norm were lower post-exposure than pre-exposure, regardless of exposure frequency. For attitude, a significant interaction effect between time and exposure frequency was found, F(3, 192) = 5.037, p = .002. Attitudes improved from T0 to T1 among unexposed participants, remained stable for those exposed 1–2 or 3–4 times, but declined for participants with five or more exposures. No pre-post changes were found for moral norm, self-efficacy, response efficacy, perceived risk of COVID-19, and perceived risk of the flu.
Intention to comply in a hypothetical high-risk pandemic situation
Intention to comply in a hypothetical high-risk pandemic situation was compared to the present low-risk situation (both measured at T1) using repeated measures ANOVA, addressing research question 3. The analysis showed a main effect of pandemic situation (current low-risk or hypothetical high-risk) on intention to comply. Intention to comply was significantly higher in a hypothetical high-risk pandemic situation (M = 4.01, SD = 0.94) than in the current low-risk situation (M = 3.61, SD = 1.24, F(1, 1096) = 8.08, p = .005). Additionally, a significant interaction effect was found between pandemic situation and behavioral measure type (F(1, 1096) = 112.99, p < .001, = .093) (Table 7). Intention to comply was higher in the hypothetical high-risk than in the current low-risk situation for both behavioral measure types. However, the mean difference was substantially larger for staying home when ill (MD = 0.73, p < .001) than for coughing and sneezing into the elbow (MD = 0.11, p = .005). This reflects that intention to comply with coughing and sneezing into the elbow is already high in the current low-risk situation, and the potential for increase is smaller than for staying home when ill.
Discussion
This field study tests the effects of persuasive messages on (behavioral determinants of) compliance with two behavioral measures to prevent the spread of viruses that cause respiratory infections such as COVID-19 and the flu, notably: coughing and sneezing into the elbow, and staying home when ill with respiratory infection symptoms. Exposure frequency has a significant effect on social norm regarding the behavioral measures and perceived risk of COVID-19 and the flu, but not on compliance or intention to comply. Hypothesis 1 and 2, i.e. that participants who are more frequently exposed to persuasive messages have a higher intention to comply and comply more often with behavioral measures than participants who are less frequent or not exposed, are thus not supported by the findings. As participants were exposed to messages conveying risks of non-compliance, positive social outcomes of compliance, and promoting empathy for others, it is to be expected that significant effects were found on related determinants.
Effect modifiers of the association between exposure frequency and behavioral determinants
Insights are also gained regarding the three exploratory research questions. Regarding research question 1, exposure frequency significantly impacts individual outcomes within the behavioral measure staying home when ill, but not within coughing/sneezing into the elbow. Moreover, compliance with and behavioral determinants of staying home when ill are significantly lower than compliance with and determinants of coughing/sneezing into the elbow, regardless of exposure frequency. This suggests that the effectiveness of repeated exposure seems to depend on the type of behavioral measure targeted in the messages. More specifically, it suggests that people are more willing to comply with behavioral measures that incur less personal and social cost. Coughing and sneezing into the elbow hardly disrupts everyday life, whereas staying home when ill with respiratory infection symptoms may severely impede daily activities and may arouse resistance, especially when one is experiencing only mild symptoms. This interpretation is consistent with research reporting that behavioral measures with moderate personal or social cost (e.g. the number of visitors allowed in home settings during the COVID-19 pandemic is slightly restricted) were more effective in reducing the number of infections than behavioral measures with high personal or social cost (e.g. the number of allowed visitors is severely restricted), due to more non-compliance with high-cost measures (Wallinga et al., 2024).
Changes over time (pre- to post-exposure) in intention to comply and behavioral determinants as a function of exposure frequency
Regarding research question 2, the findings can be cautiously interpreted by drawing on theory regarding the possible effects of repeated exposure to persuasive messages. This theorizing underscores that while exposure is necessary for persuasive messages to induce changes in behavior and determinants (Hornik, 2002), too much exposure can lead to undesired effects, such as message fatigue and reactance, counteracting changes in behavioral determinants and behavior (Cho & Salmon, 2007; Okuhara et al., 2023; Shen et al., 2022; Skurka & Keating, 2024; So et al., 2016; Zhao et al., 2023). The identified difference in intention scores between men and women depending on exposure frequency may be explained by higher reactance tendencies for men, who display the highest scores when exposed once or twice, but not more often. On the other hand, women show higher scores following more exposure. Whether reactance is a relevant factor for men, and whether even more exposure produces more positive effects for women needs to be examined in further studies. A similar pattern is found for perceived risk of COVID-19 and the flu, where participants with a non-Western migration background display the highest perceived risk with five or more exposures, whereas for Dutch participants the highest perceived risk score is obtained with one to four rather than more exposures. More research is needed to find factors that might explain this difference. No other interaction effects between exposure frequency and demographic characteristics, trust in government, prosocial orientation, perceived health, educational institution, student/employee, and participation in pre-exposure questionnaire are identified.
Intention to comply in a hypothetical high-risk pandemic situation versus the current low-risk situation
Finally, regarding research question 3, it is observed that for both behavioral measures, intention to comply following exposure to persuasive messages is higher in a hypothetical high-risk pandemic situation than in the current low-risk situation. In both situations intention to comply with coughing/sneezing into the elbow is higher than intention of staying home when ill; however, the increase in intention to comply between the low- and high-risk situation is much larger for staying home when ill than for coughing/sneezing into the elbow. This reflects that intention to comply with coughing/sneezing into the elbow is already high in the low-risk situation, and thus the potential for increase is smaller than for staying home when ill. In addition, the felt need to act, including willingness to comply with a measure that entails more personal or social cost, likely increases when the risk of infection and experiencing severe symptoms is higher (cf. e.g. Kafadar et al., 2022; Limbu & Gautam, 2023).
Strengths and limitations
The study has several strengths, yet is also prone to some limitations that warrant cautious interpretation and generalization of the findings. A strength of the field study design is the high external validity, as evidence is provided on the effects of persuasive messages on (determinants of) behavioral compliance in real-life practice. A related limitation is that field studies are susceptible to external influences beyond the researchers' control, e.g. seasonal illness trends or simultaneous public health campaigns, which may have resulted in confounding. Another study strength is the inclusion of a broad range of participants, representing all common post-secondary school educational levels in the Netherlands.
Recruitment and study conduct at the intermediate vocational education institution posed more challenges. Participants at the intermediate vocational education institution only received questions about coughing and sneezing into the elbow, as they were also only exposed to messages about this measure, per request of the educational institution. Thus, it remains opaque to what extent findings regarding staying home when ill are also applicable in these participants.
Moreover, the number of participants from this institution is relatively low. Consequently, the number of participants is not equally divided over all participating educational institutions, which poses another limitation: unequal participant numbers in groups potentially influence identification of statistically significant effects. Participant numbers were also unequal for message exposure frequency, with lower numbers of participants reporting higher exposure frequency, and for behavioral type, with lower numbers of participants in the group that answered questions about staying home when ill. We note that this may have affected statistical power and robustness of results.
Moreover, differences in the demographic composition of participants in T1 compared to T0 need to be taken into account when interpreting the results. Furthermore, self-report questionnaires entail a risk of socially desirable responding, and a risk of recall bias. Notably, the variable exposure frequency reflects participants' reported estimates of how frequently they were exposed to the persuasive messages, but they might not have been able to recall this correctly. There might be underreporting because they do not recall exposure and recall is more likely when the messages are mentally processed.
A final study strength as well as potential limitation comprises the message phrasing and poster design. Message phrasing and poster design were co-created with policy and communication experts of the Netherlands Ministry of Public Health, Welfare and Sports, as well as with students. This was done to ensure messages resembled communication of the Netherlands government during the COVID-19 pandemic, and to maximize potential practical usability in the future. However, tailoring the materials to the context of the Netherlands may also limit generalizability.
Recommendations
Lack of effects on intention and behavior might be due to the low-risk pandemic situation during the present field study, in which risk awareness is low, and thus is the felt need to act. As it is also observed that in a hypothetical high-risk pandemic situation the intention to comply increases, it might be expected that exposure to persuasive messages a high-risk situation is potentially more effective in enhancing intention and behavior. In addition, it is recommended to tailor persuasive messages to the needs of specific subgroups (e.g. by gender or cultural background, as relevant differences were found in this study) and to combine effective communication strategies such as persuasive messages with structural or policy measures, to optimize potential effects on compliance. Finally, based on the finding that people are more willing to comply with measures that are relatively easy to perform and require less personal sacrifice, explanations of specific measures' relevance and effectiveness (rather than a one-size-fits-all-measures approach) and practical support for people to comply with more difficult to perform behaviors might further stimulate compliance. Future research could investigate this, as well as the effectiveness of persuasive messages when exposure periods are longer, messages are ubiquitously present (rather than only in one specific setting), and when there is a real high-risk pandemic situation. Moreover, future research could benefit from methodological refinement such as using behavioral outcomes and objective measures of exposure rather than self-report measures.
Conclusion
In conclusion, exposure to persuasive messages impacts those behavioral determinants at which these messages are directed, that is, social norms and perceived risk of COVID-19 and the flu. However, this did not lead to changes in compliance nor intention to comply with behavioral measures. This indicates that exposing people to concise persuasive messages in their digital and physical environment, similar to communication deployed by, e.g. the Dutch government during the COVID-19 pandemic, initiates the process for enhancing compliance but as such is not yet sufficient. The findings imply practical implications and provide leads for future research.
Supplementary Material
Supplementary_file 1_Persuasive_messages.pdfSupplementary_file 1_Persuasive_messages.pdf
Supplementary_file_3_MANOVAs_descriptives_test_statistics.pdfSupplementary_file_3_MANOVAs_descriptives_test_statistics.pdf
Supplementary_file_2_Overview_measures.pdfSupplementary_file_2_Overview_measures.pdf
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1CBS. (2022). Nieuwe indeling bevolking naar herkomst. Retrieved 26 April 2023, from https://www.cbs.nl/nl-nl/longread/statistische-trends/2022/nieuwe-indeling-bevolking-naar- herkomst/4-de-nieuwe-indeling-naar-geboren-in-nederland-en-herkomstland
- 2Cho, H., & Salmon, C. T. (2007). Unintended effects of health communication campaigns. Journal of Communication, 57(2), 293–317. 10.1111/j.1460-2466.2007.00344.x · doi ↗
- 3COVID-19 Mental Disorders Collaborators. (2021). Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. The Lancet, 398(10312), 1700–1712. 10.1016/S 0140-6736(21)02143-7PMC 850069734634250 · doi ↗ · pubmed ↗
- 4De Ridder, D., Aarts, H., Benjamins, J., Glebbeek, M.-L., Leplaa, H., Leseman, P., Potgieter, R., Tummers, L., & Zondervan-Zwijnenburg, M. (2021). Keep your distance from me”: A field experiment on empathy prompts to promote distancing during the COVID-19 pandemic. Journal of Community and Applied Social Psychology, 32(4), 755–766. 10.1002/casp.259335463459 PMC 9015613 · doi ↗ · pubmed ↗
- 5Faramarzi, A., Norouzi, S., Dehdarirad, H., Aghlmand, S., Yusefzadeh, H., & Javan-Noughabi, J. (2024). The global economic burden of COVID-19 disease: A comprehensive systematic review and meta-analysis. Systematic Reviews, 13(1), 68. 10.1186/s 13643-024-02476-638365735 PMC 10870589 · doi ↗ · pubmed ↗
- 6Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41, 1149–1160. 10.3758/BRM.41.4.114919897823 · doi ↗ · pubmed ↗
- 7Gillman, A. S., Iles, I. A., Klein, W. P. M., & Ferrer, R. A. (2022). Increasing receptivity to COVID 19 public health messages with self-affirmation and self vs. other framing. Health Communication, 38(9), 1942–1953. 10.1080/10410236.2022.204302435264033 · doi ↗ · pubmed ↗
- 8Government of the Netherlands. (n.d.). Preventing respiratory infections. https://www.government.nl/topics/c/coronavirus-COVID-19/tackling-new-coronavirus-in-the-netherlands/preventing-respiratory-infections.