Effectiveness of direct oral anticoagulants for all‐cause mortality and cardiovascular events in overweight and obese patients with atrial fibrillation: Insight from the nationwide START registry
Danilo Menichelli, Gianluca Gazzaniga, Emilia Antonucci, Gualtiero Palareti, Daniela Poli, Pasquale Pignatelli, Daniele Pastori, Benilde Cosmi, Benilde Cosmi, Daniela Poli, Elena Lotti, Martina Berteotti, Walter Ageno, Giovanna Colombo, Salvatore Bradamante, Eugenio Bucherini

TL;DR
DOACs may be better than VKAs for reducing mortality and cardiovascular events in overweight and obese atrial fibrillation patients.
Contribution
This study provides real-world evidence on DOACs' effectiveness in overweight and obese AF patients using a nationwide registry.
Findings
DOACs were linked to lower all-cause mortality and cardiovascular events compared to VKAs.
Mortality benefits of DOACs were consistent in both overweight and obese patients.
Cardiovascular event reduction was significant only in overweight patients.
Abstract
Overweight and obesity are highly prevalent in atrial fibrillation (AF) patients, yet the best anticoagulant strategy for this group is still unclear. We evaluated the risk of all‐cause mortality and cardiovascular events (CVEs) in overweight and obese AF patients treated with direct oral anticoagulants (DOACs) or vitamin K antagonists (VKAs). We analysed 10,259 AF patients on anticoagulants from the prospective nationwide START registry. Overweight was defined as BMI 25–29.9 kg/m2 and obesity as BMI ≥30 kg/m2. Mortality risk was assessed with Cox proportional hazards models, and CVEs with Fine–Grey models accounting for competing risks. Additional modelling strategies, subgroup analyses, and propensity score matching were performed to explore data and ensure robustness. Overall, 6534 (63.7%) patients had BMI >25 kg/m2 (65.7% overweight, 34.3% obese). Over a median follow‐up of 17.4…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
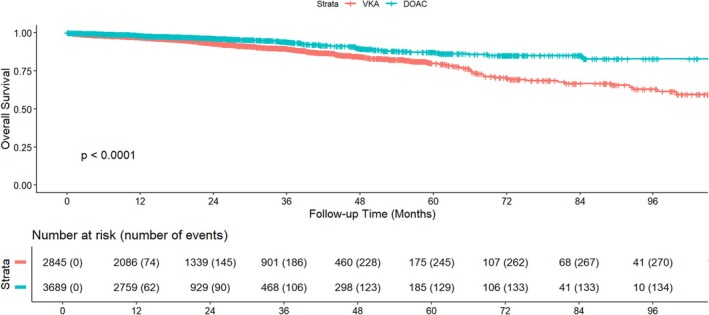 FIGURE 1
FIGURE 1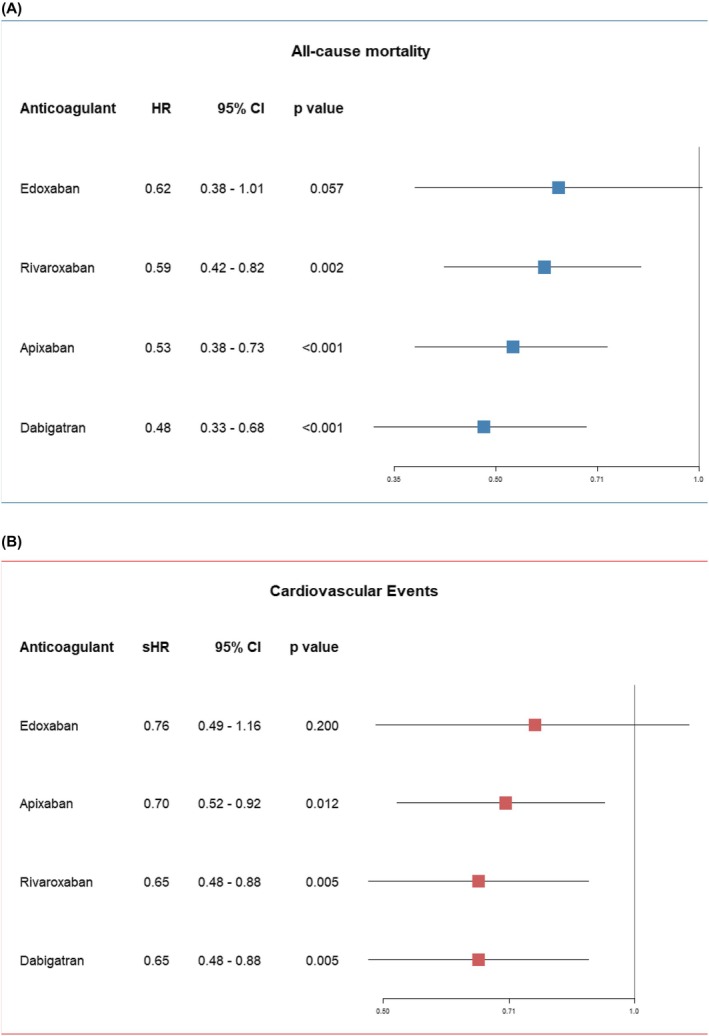 FIGURE 2
FIGURE 2|
| Overall, | Overweight |
| Obesity |
|
|
| |||
|---|---|---|---|---|---|---|---|---|---|---|
| VKA ( | DOAC ( | VKA ( | DOAC ( | |||||||
| Age (years) | 6258 | 76.0 (70.0, 82.0) | 76.0 (70.0, 81.0) | 78.0 (72.0, 83.0) | <0.001 | 73.0 (66.0, 79.0) | 76.0 (69.0, 81.0) | <0.001 | <0.001 | <0.001 |
| Age ≥ 75 years | 6258 | 3780 (57.9%) | 1069 (57.3) | 1617 (66.7) | <0.001 | 414 (42.3) | 680 (54.0) | <0.001 | <0.001 | <0.001 |
| Women | 2726 (41.7%) | 717 (38.4) | 977 (40.3) | 0.218 | 444 (45.4) | 588 (46.6) | 0.574 | <0.001 | <0.001 | |
| BMI | 6534 | 28.4 (26.6, 31.2) | 27.1 (26.0, 28.4) | 27.1 (26.0, 28.4) | 0.575 | 32.7 (31.1, 35.2) | 32.8 (31.2, 35.2) | 0.567 | <0.001 | <0.001 |
| Obesity degree | 6534 | ‐ | 0.042 | <0.001 | <0.001 | |||||
| Obesity I | 1651 (25.3%) | 0.0 | 0.0 | 723 (73.9) | 928 (73.5) | |||||
| Obesity II | 413 (6.3%) | 0.0 | 0.0 | 165 (16.9) | 248 (19.7) | |||||
| Obesity III | 176 (2.7%) | 0.0 | 0.0 | 90 (9.2) | 86 (6.8) | |||||
| Hypertension | 6534 | 5478 (83.8%) | 1477 (79.1%) | 2038 (84.0) | <0.001 | 832 (85.1) | 1131 (89.6) | 0.001 | <0.001 | <0.001 |
| Diabetes | 6534 | 1610 (24.6%) | 383 (20.5) | 492 (20.3) | 0.845 | 328 (33.5) | 407 (32.3) | 0.520 | <0.001 | <0.001 |
| CAD | 6534 | 1140 (17.5%) | 409 (21.9) | 365 (15.0) | <0.001 | 185 (18.9) | 181 (14.3) | 0.004 | 0.572 | 0.062 |
| Anaemia | 6534 | 1608 (24.6%) | 486 (26.0) | 604 (24.9) | 0.393 | 226 (23.1) | 292 (23.1) | 0.987 | 0.240 | 0.087 |
| eGFR | 6521 | 68.0 (52.0, 89.0) | 64.0 (48.0, 81.0) | 64.0 (50.0. 80.0) | 0.062 | 82.0 (58.5. 105.0) | 79.0 (60.0, 101.0) | 0.925 | <0.001 | <0.001 |
| eGFR <30 ml/min | 6521 | 192 (2.9%) | 114 (6.1) | 30 (1.2) | <0.001 | 42 (4.3) | 6 (0.5) | <0.001 | 0.026 | 0.043 |
| Heart failure | 6534 | 1487 (22.8%) | 441 (23.6) | 485 (20.0) | 0.004 | 251 (25.7) | 310 (24.6) | 0.551 | 0.001 | 0.227 |
| Smoking | 6534 | 297 (4.5%) | 95 (5.1) | 92 (3.8) | 0.039 | 50 (5.1) | 60 (4.8) | 0.697 | 0.162 | 0.978 |
| Previous stroke/TIA | 6534 | 964 (15%) | 263 (14.1) | 406 (16.7) | 0.018 | 116 (11.9) | 179 (14.2) | 0.107 | 0.045 | 0.097 |
| PAD | 6534 | 393 (6.0%) | 133 (7.1) | 140 (5.8) | 0.071 | 61 (6.2) | 59 (4.7) | 0.103 | 0.163 | 0.373 |
| COPD/OSAS | 6534 | 817 (12.5%) | 207 (11.1) | 251 (10.3) | 0.433 | 150 (15.3) | 209 (16.6) | 0.434 | <0.001 | 0.001 |
| CHA2DS2‐VASc | 6528 | 4.0 (3.0, 5.0) | 4.0 (2.0, 5.0) | 4.0 (3.0, 5.0) | 0.002 | 4.0 (2.0, 4.0) | 4.0 (3.0, 5.0) | <0.001 | 0.119 | 0.675 |
| HAS‐BLED | 6528 | 2.0 (2.0, 2.0) | 2.0 (2.0, 3.0) | 2.0 (2.0, 2.0) | 0.092 | 2.0 (1.0, 2.0) | 2.0 (2.0, 2.0) | <0.001 | 0.507 | 0.005 |
|
| ||||||||||
| Anticoagulant type | 6534 | <0.001 | <0.001 | <0.001 | ‐ | |||||
| VKA | 2845 (43.7%) | 100.0 | 0.0 | 100.0 | 0.0 | |||||
| Apixaban | 1142 (17.5%) | 0.0 | 717 (29.5) | 0.0 | 425 (33.7) | |||||
| Rivaroxaban | 1016 (15.6%) | 0.0 | 696 (28.7) | 0.0 | 320 (25.4) | |||||
| Edoxaban | 621 (9.5%) | 0.0 | 448 (18.5) | 0.0 | 173 (13.7) | |||||
| Dabigatran | 910 (13.9%) | 0.0 | 566 (23.3) | 0.0 | 344 (27.3) | |||||
| TTR | 1867 | 67.0 (56.0, 76.0) | 68.0 (57.0, 77.0) | ‐ | ‐ | 65.0 (53.0, 75.0) | ‐ | ‐ | ‐ | 0.001 |
| TTR in range (≥60%) | 1867 | 1271 (68%) | 879 (71%) | ‐ | ‐ | 392 (62%) | ‐ | ‐ | ‐ | <0.001 |
| DOAC Reduced Dose | 3689 | 1298 (35%) | ‐ | 938 (39%) | ‐ | ‐ | 360 (29%) | ‐ | <0.001 | ‐ |
| Antiplatelet | 6534 | 786 (12.0%) | 286 (15.3) | 243 (10.0) | <0.001 | 128 (13.1) | 129 (10.2) | 0.035 | 0.841 | 0.109 |
| Class 1c AAD | 6534 | 530 (8.1%) | 118 (6.4) | 249 (10.3) | <0.001 | 61 (6.3) | 102 (8.1) | 0.101 | 0.032 | 0.913 |
| Amiodarone | 6534 | 840 (12.9%) | 273 (14.6) | 282 (11.6) | 0.004 | 138 (14.1) | 147 (11.6) | 0.083 | 0.979 | 0.712 |
| Lipid lowering therapy | 6534 | 2456 (37.6%) | 690 (37.0) | 885 (36.5) | 0.740 | 366 (37.4) | 515 (40.8) | 0.104 | 0.010 | 0.807 |
| RAASi | 6534 | 3920 (60.0%) | 1084 (58.1) | 1432 (59.0) | 0.535 | 613 (62.7) | 791 (62.7) | 1.000 | 0.030 | 0.017 |
| Beta blockers | 6534 | 3095 (47.4%) | 1004 (53.8) | 1008 (41.5) | <0.001 | 562 (57.5) | 521 (41.3) | <0.001 | 0.884 | 0.060 |
| Calcium channel blockers | 6534 | 1558 (23.8%) | 479 (25.7) | 509 (21.0) | <0.001 | 271 (27.7) | 299 (23.7) | 0.030 | 0.058 | 0.238 |
| Diuretics | 6534 | 2662 (40.7%) | 687 (36.8) | 926 (38.2) | 0.363 | 458 (46.8) | 591 (46.8) | 1.000 | <0.001 | <0.001 |
| Digoxin | 6534 | 516 (7.9%) | 162 (8.7) | 169 (7.0) | 0.037 | 92 (9.4) | 93 (7.4) | 0.082 | 0.649 | 0.517 |
| PPI | 6534 | 2329 (35.6%) | 704 (37.7) | 815 (33.6) | 0.005 | 362 (37.0) | 448 (35.5) | 0.459 | 0.244 | 0.717 |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI |
| HR | 95% CI |
| |
| DOAC (vs VKA) | 0.54 | 0.44, 0.67 | <0.001 | 0.57 | 0.46, 0.70 | <0.001 |
| Obesity (vs | 1.00 | 0.81, 1.22 | 0.962 | |||
| Age ≥75 years | 3.09 | 2.42, 3.94 | <0.001 | 1.91 | 1.45, 2.50 | <0.001 |
| Women | 1.11 | 0.91, 1.34 | 0.311 | |||
| Hypertension | 1.11 | 0.83, 1.47 | 0.482 | |||
| Diabetes | 1.16 | 0.93, 1.44 | 0.189 | |||
| CAD | 1.60 | 1.28, 2.01 | <0.001 | 1.39 | 1.08, 1.78 | 0.011 |
| Anaemia | 2.18 | 1.78, 2.66 | <0.001 | 1.41 | 1.14, 1.75 | 0.002 |
| eGFR | 0.97 | 0.97, 0.98 | <0.001 | 0.99 | 0.98, 0.99 | <0.001 |
| Heart failure | 1.91 | 1.56, 2.35 | <0.001 | 1.32 | 1.05, 1.65 | 0.017 |
| Smoking | 0.77 | 0.44, 1.33 | 0.347 | |||
| Previous stroke/TIA | 1.18 | 0.92, 1.52 | 0.191 | |||
| PAD | 2.16 | 1.59, 2.95 | <0.001 | 1.77 | 1.29, 2.43 | <0.001 |
| COPD/OSAS | 2.05 | 1.61, 2.59 | <0.001 | 1.58 | 1.23, 2.03 | <0.001 |
| Antiplatelet | 1.24 | 0.93, 1.64 | 0.137 | |||
| Class 1c AAD | 0.35 | 0.20, 0.62 | <0.001 | 0.52 | 0.29, 0.92 | 0.026 |
| Amiodarone | 0.95 | 0.71, 1.27 | 0.726 | |||
| Lipid lowering therapy | 0.75 | 0.61, 0.92 | 0.006 | 0.67 | 0.54, 0.85 | <0.001 |
| RAASi | 0.66 | 0.55, 0.81 | <0.001 | 0.67 | 0.55, 0.81 | <0.001 |
| Beta blockers | 0.96 | 0.79, 1.17 | 0.683 | |||
| Calcium channel blockers | 1.09 | 0.87, 1.35 | 0.456 | |||
| Diuretics | 1.64 | 1.35, 1.99 | <0.001 | 1.07 | 0.86, 1.33 | 0.532 |
| Digoxin | 1.07 | 0.77, 1.49 | 0.690 | |||
| PPI | 1.12 | 0.91, 1.36 | 0.280 | |||
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| sHR | 95% CI |
| sHR | 95% CI |
| |
| DOAC (vs VKA) | 0.68 | 0.56, 0.81 | <0.001 | 0.71 | 0.59, 0.86 | <0.001 |
| Obesity (vs | 0.99 | 0.82, 1.20 | 0.952 | |||
| Age ≥75 years | 2.63 | 2.12, 3.27 | <0.001 | 1.66 | 1.30, 2.11 | <0.001 |
| Women | 1.05 | 0.88, 1.26 | 0.569 | |||
| Hypertension | 1.11 | 0.85, 1.44 | 0.450 | |||
| Diabetes | 1.22 | 1.00, 1.49 | 0.054 | |||
| CAD | 1.65 | 1.34, 2.02 | <0.001 | 1.44 | 1.14, 1.83 | 0.003 |
| Anaemia | 1.96 | 1.62, 2.36 | <0.001 | 1.34 | 1.10, 1.63 | 0.004 |
| eGFR | 0.98 | 0.97, 0.98 | <0.001 | 0.99 | 0.98, 0.99 | <0.001 |
| Heart failure | 1.80 | 1.49, 2.18 | <0.001 | 1.29 | 1.05, 1.60 | 0.017 |
| Smoking | 0.97 | 0.61, 1.53 | 0.880 | |||
| Previous stroke/TIA | 1.21 | 0.96, 1.52 | 0.106 | |||
| PAD | 2.17 | 1.63, 2.89 | <0.001 | 1.79 | 1.33, 2.40 | <0.001 |
| COPD/OSAS | 1.91 | 1.53, 2.39 | <0.001 | 1.52 | 1.20, 1.92 | <0.001 |
| Antiplatelet | 1.43 | 1.12, 1.83 | 0.004 | 1.04 | 0.80, 1.36 | 0.761 |
| Class 1c AAD | 0.42 | 0.26, 0.67 | <0.001 | 0.58 | 0.35, 0.94 | 0.028 |
| Amiodarone | 0.91 | 0.69, 1.20 | 0.507 | |||
| Lipid lowering therapy | 0.82 | 0.68, 0.99 | 0.036 | 0.72 | 0.58, 0.88 | 0.002 |
| RAASi | 0.76 | 0.64, 0.91 | 0.003 | 0.76 | 0.63, 0.91 | 0.003 |
| Beta blockers | 0.87 | 0.73, 1.05 | 0.141 | |||
| Calcium channel blockers | 1.05 | 0.86, 1.29 | 0.623 | |||
| Diuretics | 1.48 | 1.24, 1.77 | <0.001 | 0.99 | 0.81, 1.21 | 0.896 |
| Digoxin | 0.99 | 0.72, 1.35 | 0.943 | |||
| PPI | 1.01 | 0.84, 1.22 | 0.906 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Venous Thromboembolism Diagnosis and Management · Cardiovascular Disease and Adiposity
INTRODUCTION
1
Obesity affected around 890 million adults worldwide in 2022, corresponding to 16.0% of adults ≥18 years worldwide.1 The prevalence of obesity has been increasing worldwide in the last decades and, according to the Global Burden of Disease, it is estimated to affect 2.1 billion adults in 2013.2 In particular, the prevalence of obesity raised up to 50% of the adult population in some countries from Oceania, North Africa, and the Middle East,3 while it was about 41.8% in North America1 and 20% in Western Europe.3 In particular, a low prevalence (<20%) of obesity was observed in countries from the Mediterranean area that had an obesity prevalence between 20.0% and 24.9%,4 while Northern (i.e. United Kingdom and Ireland), and Eastern (i.e. Bulgaria, Hungary and Lithuania) Europe had a higher prevalence of obesity (25.0%–29.9%).4 In the past decades, the prevalence of obesity in Italy was 8%, due to a healthy diet and lifestyle; however, in the last years, the prevalence has increased abruptly by 27.5% due to lifestyle changes such as the consumption of high‐caloric foods and sedentary behaviors5 reaching 19.9% in 2019.4
It was estimated that the rising of the overweight and obese population provoked 3.4 million deaths and 3.9% of years of life lost worldwide.2 In addition, obesity has been associated with several cardiovascular (CV) risk factors such as arterial hypertension, diabetes mellitus and dyslipidemia3 and CV disease.3 Among CV diseases, atrial fibrillation (AF) is strongly associated with obesity6: indeed, epidemiologic studies showed that the two major predictors of new‐onset AF are arterial hypertension and obesity.6, 7 In particular, data from the Framingham Heart Study, seem to suggest that obesity could increase the risk of AF by 50%.8 Several mechanisms such as epicardial adiposity, inflammation, oxidative stress, fibrosis, ion channel alterations, and autonomic dysfunction seem to be involved in the left atrium enlargement and AF pathogenesis in obese patients.6
Although obesity is a risk factor for new‐onset AF, its role in the prognosis of AF patients is still contradictory. Indeed, results from a post‐hoc analysis of The Effective Anticoagulation With Factor Xa Next Generation in Atrial Fibrillation–Thrombolysis in Myocardial Infarction 48 (ENGAGE AF‐TIMI 48) trial revealed that overweight and obese patients with AF had a lower risk of stroke/systemic embolism and mortality.9 These results were coherent with a post‐hoc analysis of the Atrial Fibrillation Follow‐up Investigation of Rhythm Management (AFFIRM) trial, in which obese and overweight patients had a lower all‐cause mortality risk compared to normal weight.10 Conversely, data from the prospective Danish Diet, Cancer and Health study, in which 3135 AF patients were enrolled and followed up to 4.9 years found a direct association between overweight/obesity and ischemic stroke, thromboembolism or death.11 Also, a large meta‐analysis including 49,364 AF patients found no difference in all‐cause and CV death risk between obese and normal weight AF patients.12
While long‐term anticoagulation treatment with vitamin K antagonists (VKAs) or direct oral anticoagulants (DOACs) is effective in the majority of AF patients to reduce thromboembolism,13 less evidence is available in patients with obesity. In previous studies14, 15, 16, 17, 18 the effectiveness and safety of DOAC in obese patients with AF appear controversial.
In addition, few prospective studies based on real‐world data from observational studies are available. For this reason, the aim of our study was to investigate the effectiveness of DOACs compared to VKAs in a real‐world cohort of overweight and obese patients with AF.
METHODS
2
START Registry
2.1
The START registry is a prospective, observational, multicenter cohort study conducted in Italy, enrolling patients aged 18 years or older who initiate anticoagulation therapy for AF. Comprehensive details about the registry have been previously published.19 Briefly, inclusion criteria comprised adult patients with AF requiring oral anticoagulation; patients receiving low‐molecular‐weight heparin were excluded. Individuals with a life expectancy of less than 6 months, those not residing in the participating region, or planning to relocate within the next 6 months were not eligible for inclusion in the registry. Patients already participating in phase 2 or 3 clinical trials were also excluded, whereas those enrolled in other observational or phase 4 studies were eligible.
The study is registered at ClinicalTrials.gov (NCT02219984) and received approval from the Institutional Review Boards of all participating institutions. Informed consent was obtained from each participant prior to inclusion, and the study protocol complies with the ethical standards set forth in the 1975 Declaration of Helsinki.
This post‐hoc analysis was restricted to only patients with AF and overweight or obesity.
Baseline features
2.2
Baseline variables comprised demographic information and clinical data, encompassing cardiovascular risk factors, routinary laboratory parameters, relevant comorbidities, left ventricular ejection fraction, smoking status, indication for anticoagulation therapy, the specific class of oral anticoagulant administered, and concurrent pharmacological treatments. A history of cardiovascular disease was defined as documented coronary artery disease (CAD), including prior myocardial infarction or coronary revascularization (via percutaneous coronary intervention or coronary artery bypass grafting). Cerebrovascular disease was defined by a prior ischemic stroke or transient ischemic attack (TIA).
Overweight and obesity definitions
2.3
Obesity and overweight were defined and classified according to The World Health Organization (WHO).4, 20, 21 The WHO,21 classifies adult obesity using the body mass index (BMI), which is measured by calculating [(weight in kg)/(height in m)^2^]. Overweight was defined by BMI between 25.0 and 29.9 kg/m^2^ and obesity by a BMI ≥30.0 kg/m^2^. Obese patients were stratified into class I (BMI: 30.0–34.9 kg/m^2^); class II (BMI: 35.0–39.9 kg/m^2^) and class III (BMI ≥40.0 kg/m^2^).
Study Endpoints
2.4
The aim of this study was to investigate the association between oral anticoagulant type (DOACs vs. VKAs) and clinical outcomes in patients with a BMI >25 kg/m^2^, with particular attention to differences between overweight and obese subgroups. Specifically, all‐cause mortality and the occurrence of cardiovascular events (CVEs) were evaluated according to anticoagulant type, both in the overall population, and according to overweight and obesity. CVEs were defined as fatal or non‐fatal myocardial infarction, coronary revascularization, fatal or non‐fatal ischemic stroke, and transient ischemic attack. All events were prospectively documented during follow‐up visits and recorded by registry investigators in the electronic case report form.
Statistical analysis
2.5
Descriptive statistics were employed to characterize the study population. The distribution of continuous variables was evaluated using the Kolmogorov–Smirnov test. Variables with normal distribution were summarized using means and standard deviations, whereas non‐normally distributed variables were expressed as medians with interquartile ranges (IQR). Categorical variables were reported as absolute frequencies and percentages. Group comparisons for continuous variables were performed using the independent samples t‐test or the Wilcoxon rank‐sum test, depending on the distribution. Categorical variables were compared using the chi‐square test or Fisher's exact test, as appropriate. For comparisons involving more than two groups, one‐way analysis of variance (ANOVA) or the non‐parametric Kruskal–Wallis test was applied.
To explore the geographical distribution of patients with BMI >25 kg/m^2^, the population was stratified by Italian region, and a choropleth map was produced to visualize regional differences.
To evaluate differences in all‐cause mortality based on anticoagulant type, we conducted Kaplan–Meier survival analyses in the overall study population. Survival curves were generated using the Kaplan–Meier method and compared using the log‐rank test. Univariable and multivariable Cox proportional hazards regression models were subsequently used to estimate hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) for all‐cause mortality associated with the use of DOACs vs. VKAs and individual clinical variables.
The Fine–Grey subdistribution hazard model was employed to estimate the cumulative incidence of CVEs, accounting for the competing risk of all‐cause mortality. Cumulative Incidence Functions (CIF) were plotted to visualize cumulative incidence.
The following clinical and pharmacological variables were evaluated as candidate predictors in both Cox proportional hazards and Fine–Grey competing risks regression models: use of DOAC, BMI category, age ≥75 years, female sex, history of hypertension, diabetes mellitus, CAD, anaemia, impaired renal function (expressed as estimated glomerular filtration rate – eGFR), heart failure (HF), active smoking, previous stroke or TIA, peripheral artery disease (PAD), chronic obstructive pulmonary disease or obstructive sleep apnoea syndrome (COPD/OSAS), antiplatelet therapy, use of class 1c antiarrhythmic drugs, amiodarone, lipid‐lowering therapy, renin–angiotensin–aldosterone system inhibitors (RAASi), beta blockers, calcium channel blockers, diuretics, digoxin, and proton pump inhibitors (PPI). Variables demonstrating statistical significance in univariable analyses (p < 0.05) were subsequently included in the multivariable models.
These analyses were initially conducted in the overall population of patients with a BMI greater than 25 kg/m^2^ and subsequently repeated after stratifying the cohort by overweight and obese categories.
To avoid potential bias from variable selection based only on univariate p‐values filtering, we constructed a second multivariable Cox model and Fine–Grey model including a set of prespecified clinically relevant covariates (i.e. anticoagulant type, BMI class, age, sex, hypertension, diabetes, CAD, anaemia, renal function [eGFR], HF, Paroxysmal Atrial Fibrillation, PAD, and COPD/OSAS). To formally test for effect modification by BMI, the models also included an interaction term between anticoagulant type and BMI class.
The proportional hazards assumption was assessed using Schoenfeld residuals (data shown in Table S1).
To address potential confounding between patients treated with DOACs and those receiving VKAs, we used propensity score matching (PSM) to evaluate the consistency of results across modelling approaches. Propensity scores were estimated via logistic regression, including the following predefined covariates: sex, age, HF, BMI, hypertension, diabetes, CAD, anaemia, eGFR, previous stroke/TIA, COPD/OSAS, smoking, antiplatelet, Class 1c AAD, amiodarone, and beta‐blockers' use. These variables were selected as they represent the most frequent comorbidities and treatments in patients with AF. DOAC users were matched 1:1 to VKA users using nearest‐neighbour matching with a calliper width of 0.1, without replacement. Covariate balance after matching was assessed with standardized mean differences (SMDs), with values <0.1 indicating adequate balance. Patient characteristics before and after matching are summarized in Table S2, and additional PSM balance diagnostics are reported in Table S3. The matched cohorts were subsequently analysed. HR for all‐cause mortality was derived from a univariate Cox proportional hazards model, while the risk of CVEs was evaluated using a univariate Fine–Grey model, accounting for all‐cause death as a competing risk.
Lastly, we performed some exploratory analyses. (1) Restricted Cubic Splines (RCS) with 4 default knots were used to assess potential non‐linear associations between BMI, treated as a continuous variable, and all‐cause mortality in a univariable model. (2) Patients were stratified according to time in therapeutic range (TTR), calculated using the Rosendaal method,22 with 60% as the threshold; patients with missing TTR values were excluded from this analysis. (3) An analysis to compare the use of DOAC vs. VKA in each subgroup of patients according to obesity severity (I‐III) with overweight as a reference. (4) A subgroup analysis for all‐cause mortality and CVE risk was conducted in patients weighing ≥100 kg. (5) Univariable Cox and Fine‐Grey models were used to examine the association of each DOAC agent versus VKA with all‐cause mortality and CVEs, respectively.
Statistical analyses were conducted using R (version 4.2.3) and IBM SPSS Statistics (version 25.0), with a two‐sided significance threshold set at α = 0.05.
RESULTS
3
Geographic distribution
3.1
Overall, 10,259 patients were enrolled in the START registry. Of these, 6534 patients (63.7%) had a BMI >25 kg/m^2^. The geographic distribution of patients with BMI >25 kg/m^2^ across Italian regions is shown in Figure S1. The highest prevalence of BMI >25 kg/m^2^ relative to total patients was observed in Puglia (655 patients, 81.1%), followed by Calabria (75%) regions.
Descriptive analysis
3.2
Table 1 summarizes the baseline characteristics of the 6534 patients with BMI >25 kg/m^2^ enrolled in the START registry, stratified by overweight (BMI 25–29.9 kg/m^2^) and obese (BMI ≥30 kg/m^2^) status. The median age was 76.0 years (IQR 70.0–82.0), and 41.7% of patients were women. In the overweight group (n = 4294 AF patients), patients on DOACs (n = 2427) were older, more frequently women and affected by arterial hypertension, and had a history of previous stroke or TIA compared to VKA. Conversely, patients on VKA (n = 1867) were more frequently affected by CAD, severe chronic kidney disease with eGFR <30 mL/min/1.73 m^2^ and HF. A significant difference in the management of rhythm and rate control strategies and antiplatelet use was found between the two groups.
On the other hand, in the obesity groups (n = 2240 AF patients), patients on DOACs (n = 1262) were older, more frequently women and affected by arterial hypertension compared to VKA. AF patients on VKA (n = 978) were more frequently affected by CAD, severe chronic kidney disease with eGFR <30 mL/min/1.73 m^2^, and had a higher proportion of patients with a severe degree of obesity.
Significant differences in the management of rate control (i.e. calcium channel blockers and beta blockers) strategy and antiplatelet were found between two groups (Table 1).
Baseline characteristics of the 2240 obese patients, stratified by obesity class Obesity I (BMI 30.0–34.9 kg/m^2^, n = 1651), Obesity II (BMI 35.0–39.9 kg/m^2^, n = 413), and Obesity III (BMI ≥40.0 kg/m^2^, n = 176) and explorative comparisons are presented in Table S4.
Survival analysis
3.3
During follow‐up, 408 all‐cause deaths, and 481 CVEs occurred. The Kaplan–Meier curve in Figure 1 illustrates overall survival in patients with BMI >25 kg/m^2^, stratified by type of oral anticoagulant (DOAC vs. VKA). Over a median follow‐up of 17.4 [IQR 12.0–30.6] months, patients treated with DOACs demonstrated significantly better survival compared to those on VKAs (log‐rank p < 0.0001).
Kaplan–Meier survival curves by anticoagulant type.
The results of the univariable and multivariable Cox proportional hazards models for all‐cause mortality are summarized in Table 2. In the multivariable model, treatment with DOACs was independently associated with a significantly lower risk of all‐cause mortality compared to VKAs (HR 0.57, 95% CI 0.46–0.70, p < 0.001). This result was then confirmed by performing univariable Cox regression analysis on the PSM cohort (HR 0.49, 95% CI 0.38–0.62, p < 0.001).
Obesity status (vs overweight) was not associated with mortality (HR 1.00, 95% CI 0.81–1.22, p = 0.962). In contrast, age ≥75 years, CAD, anaemia, HF, PAD, COPD/OSAS and reduced eGFR were associated with mortality (Table 2). Among pharmacological treatments, the use of lipid‐lowering therapy, RAAS inhibitors, and Class 1c antiarrhythmics was associated with a lower risk of death (Table 2).
Similar results were observed in the multivariable model including clinically relevant covariates and an interaction term for anticoagulant type and BMI Class (Table S5), DOAC use was associated with a significantly lower risk of all‐cause mortality (HR 0.41, 95% CI 0.31–0.54, p < 0.001) compared with VKAs. Obesity, relative to overweight, was not independently associated with either outcome, and the interaction term did not reach statistical significance.
Table S6 reports the results of separate Cox regression analyses in overweight (Panel A) and obese (Panel B) patients. In both groups, DOAC therapy remained associated with a lower risk of all‐cause mortality (Overweight: HR 0.52, 95% CI 0.39–0.68; Obese: HR 0.69, 95% CI 0.48–0.98) after adjustment.
Predictors of CVEs
3.4
The overall incidence rate of CVEs was 3.69 per 100 person‐years (95% CI: 3.37–4.04). CIF curves are shown in Figure S2. Results of Fine‐Grey competing risk regression identifying predictors of CVEs are shown in Table 3. In the overall population, DOAC use was associated with a lower subdistribution hazard for CVEs compared to VKA, both in univariable (sHR 0.68, 95% CI 0.56–0.81, p < 0.001) and multivariable models (sHR 0.71, 95% CI 0.59–0.86, p < 0.001). This result was then confirmed by performing univariable Fine‐Grey analysis on the PSM cohort (sHR 0.63, 95% CI 0.51–0.78, p < 0.001).
Obesity was not associated with a difference in CVE risk compared to overweight (sHR 0.99, 95% CI 0.82–1.20, p = 0.952). Advanced age (≥75 years), CAD, anaemia, HF, PAD, and COPD/OSAS emerged as independent predictors of increased CVE risk. Conversely, lipid‐lowering therapy (sHR 0.72, 95% CI 0.58–0.88, p = 0.002), RAAS inhibitors (sHR 0.76, 95% CI 0.63–0.91, p = 0.003), and class 1c antiarrhythmics (sHR 0.58, 95% CI 0.35–0.94, p = 0.028) were associated with reduced risk.
Similar results were also observed in the second model, including only clinically relevant covariates and the interaction term between anticoagulant type and BMI Class (Table S5), DOAC use was associated with significantly lower risk of CVEs (sHR 0.55, 95% CI 0.43–0.71, p < 0.001) compared with VKAs, with no statistical significance of the interaction term.
In stratified Fine–Grey analyses (Table S7), DOAC use remained significantly associated with reduced risk of CVEs among overweight patients (sHR 0.67, 95% CI 0.53–0.86, p = 0.002), but this association did not reach statistical significance in the obese subgroup (sHR 0.80, 95% CI 0.58–1.09, p = 0.153). Among overweight patients, several clinical factors—including age ≥75 years, CAD, PAD, and COPD/OSAS, and reduced eGFR—were robust predictors of increased CVE risk. Similar risk factors were identified in the obese group, with significant contributions from HF, anaemia, PAD, and prior stroke/TIA. Notably, lipid‐lowering therapy and RAAS inhibitors were protective in overweight individuals, but not in those with obesity (Table S7).
Exploratory analyses
3.5
In the univariable Cox model with RCS, BMI as a continuous variable was not significantly associated with all‐cause mortality (overall effect p = 0.76; test for nonlinearity p = 0.70, Figure S3). The spline curve showed a relatively flat relationship between BMI and mortality, indicating no clear evidence of increased or reduced risk across the BMI spectrum, which is consistent with the findings of the other Cox models. Then, we performed an analysis stratifying patients according to TTR class (threshold 60%). TTR data were available for 1867 patients (65.6% of the cohort), of whom 1271 (68%) had TTR ≥60%. Table S8 reports the results of multivariable Cox regression for all‐cause mortality and Fine–Grey models for CVEs, stratified by TTR. In patients with TTR ≥60% (Panel A), DOAC use was associated with a lower risk of all‐cause mortality (HR 0.47, 95% CI 0.35–0.63, p < 0.001) and CVEs (sHR 0.64, 95% CI 0.49–0.83, p < 0.001) compared to VKA. Obesity was not significantly associated with outcomes, and the interaction term between DOAC and obesity was not statistically significant. Among patients with TTR <60% (Panel B), DOAC use remained strongly protective for all‐cause mortality (HR 0.32, 95% CI 0.23–0.44, p < 0.001) and CVEs (sHR 0.43, 95% CI 0.33–0.58, p < 0.001). The interaction between DOAC and obesity was statistically significant for all‐cause mortality, suggesting that in patients with suboptimal TTR, the mortality benefit of DOAC may be attenuated in obese patients. No significant interaction was observed for CVEs.
Third, although the low number of patients with severe obesity, we performed an exploratory analysis, to evaluate the use of DOAC, compared to warfarin use, in each subgroup of patients according to obesity severity. At univariable Cox analysis (Table S9), we observed a reduction in the all‐cause of death risk in overweight and obesity 1st degree severity patients treated with DOAC, without difference between DOAC and VKA use in patients with 2nd and 3rd degree of obesity (Table S9A). For CVEs, a univariable Fine‐Grey competing risk analysis showed a lower incidence of CVEs in overweight patients treated with DOAC, while no differences were detected across the higher obesity categories (Table S9B).
Fourth, we performed a subgroup analysis restricted to patients with body weight ≥100 kg. Overall, 708 patients (10.8% of the cohort) were in this group, accounting for 41 deaths and 51 CVEs. In univariable models, DOAC use was not significantly associated with all‐cause mortality (HR 0.88, 95% CI 0.47–1.65, p = 0.691) or with CVEs (sHR 0.95, 95% CI 0.54–1.67, p = 0.850).
Lastly, we examined the association of individual DOAC agents with outcomes, using VKA as the reference (Figure 2). For both all‐cause mortality (Panel A) and CVEs (Panel B), Apixaban, Rivaroxaban, and Dabigatran were associated with lower risk, whereas Edoxaban did not reach statistical significance.
Forest plot showing the association of individual DOAC agents versus VKA with all‐cause mortality (A) and cardiovascular events (B).
DISCUSSION
4
In this large, real‐world cohort of AF patients enrolled in the START registry, we found a high prevalence of overweight obesity accounting for nearly two‐thirds of the total population, with diverse distribution across Italian regions. The distribution in our cohort reflects the Italian general population with a higher prevalence of overweight and obesity in southern countries of Italy23 and older adults.23 However, although we found a similar prevalence of overweight in AF patients (40.8%) compared to the general population with age ≥75 years (41.3%),23 we found a higher prevalence of obesity in our cohort (23.1%) compared to the overall population (13.4%) with a similar age observed in the literature.23 This finding confirms that patients with AF are affected by multiple cardio‐metabolic risk factors.
Despite this high prevalence and although obese patients exhibited a higher burden of cardiometabolic comorbidities, including hypertension, diabetes, and COPD/OSAS, compared to overweight patients, obesity was not associated with an increased risk of all‐cause mortality or CVEs.
In exploratory analyses, RCS modelling showed a relatively flat relationship between BMI and mortality, indicating no clear evidence of either increased or reduced risk across the BMI spectrum. At very high body weight, DOAC use was not associated with either outcome, although this may reflect limited statistical power due to the small number of events.
In contrast, we observed a significant effect of eGFR on both all‐cause mortality and CVE risk across different modelling strategies. This aspect has been explored in detail in a previous publication.24
Importantly, treatment with DOACs was associated with a lower risk of both all‐cause mortality and CVEs, with consistent effects observed in overweight patients. However, in the obese subgroup, the inverse association of DOACs with CVEs did not reach statistical significance, suggesting potential effect modification by body size or residual confounding.
A retrospective study from the ARISTOPHANES cohort14 performed on 88,461 AF patients with obesity (BMI ≥30 kg/m^2^) found a lower risk of ischemic stroke and systemic embolism in patients treated with apixaban and rivaroxaban compared to VKA. However, patients were followed for a short period (6.9 months) and no data were available on other clinical outcomes such as all‐cause mortality and CVEs and about concomitant comorbidities and therapies.14
A post‐hoc analysis of the ENSURE‐AF15 trial, which included 2199 AF patients undergoing cardioversion showed no significant differences between warfarin and DOAC in reducing a composite endpoint of stroke, systemic embolic event, myocardial infarction, cardiovascular death, and regarding safety, (composite of major and clinically relevant non‐major bleeding). However, the short follow‐up (2 months), the younger age (mean age 63 years) and the peculiar clinical setting as patients undergoing cardioversion for AF may explain the differences in the results.
A further study performed on 28,011 veterans with AF from the retrospective registry Veterans Health Administration Corporate Data Warehouse17 showed no difference in the effectiveness of DOAC and VKA, although DOACs were associated with a lower risk of bleeding compared to VKA. However, the cohort enrolled only patients with severe obesity (weight ≥120 kg or BMI >40 kg/m^2^) and the population was younger (about 63 years) compared to our AF cohort and it is made up almost exclusively of male veterans, underlining a potential selection bias.
Another retrospective analysis from 2 healthcare claims databases16 enrolling 3563 matched pairs of morbidly obese AF, defined according to International Classification of Diseases‐9 (ICD‐9), showed similar effectiveness of ischemic stroke and systemic embolism between rivaroxaban and warfarin with a lower risk of bleeding in the rivaroxaban group. Patients enrolled were younger than our cohort (mean age 63 years), were treated only with rivaroxaban instead of all DOACs and were followed only for a mean of 10.3 months. Furthermore, no data about all‐cause mortality and CVEs were available.
Additionally, a retrospective study performed18 on 29,135 AF patients followed for a mean of 44.4 months showed no difference in bleeding and ischemic stroke between oral anticoagulants but a higher mortality rate in patients underweight and with obesity degree I treated with DOACs. The cohort was similar to our population with a mean age of 76 years and a high thromboembolic risk (mean CHA_2_DS_2_‐VASc of 3.5). The higher mortality risk may be explained because of concomitant diseases: indeed, patients on DOACs, compared to VKA, had a greater proportion of the elderly and comorbidities, as also explained by Nakao et al.18
Finally, a recent metanalysis,25 including 434,320 obese patients with either AF or venous thromboembolism, found similar results to our study: indeed, they observed a reduction in the composite outcome (all‐cause mortality, stroke, systemic embolism, and myocardial infarction). However, the heterogeneity of the studies included and population characteristics, the inclusion of both patients with AF and venous thromboembolism, the different doses of anticoagulation by clinical indication and the inclusion of several retrospective studies represented limitations and potential sources of bias in the analysis.
In synthesis, controversial results of previous studies performed in AF patients with obesity may be caused by different inclusion criteria (i.e. different obesity degrees included), different clinical outcomes, length of follow‐up, heterogeneity of comorbidity and age and the design of the studies, often retrospective or post‐hoc analyses of clinical trials with very restricted inclusion criteria.
Strengths
4.1
Our study had several strengths. Firstly, the prospective design could identify obese patients with a specific tool as BMI instead of ICD code. Furthermore, patients were consecutively enrolled and observed during a long follow‐up evaluating CVEs and all‐cause mortality, instead of only ischemic stroke risk. In addition, the START registry was well characterized with several comorbidities' information collected at baseline compared to retrospective studies that often were subjected to limited clinical information and selection bias. Finally, our multicenter cohort reflects real‐world data on patients with AF, an elderly population with multiple comorbidities and high thromboembolic and cardiovascular risk and may be useful to estimate the effect of DOAC in this older and frail population.
Limitations
4.2
However, our study has several limitations. First, this was a multicenter study conducted in Italy and included predominantly Caucasian patients; therefore, these findings may be generalizable to Western countries with a similar prevalence of obesity; however, further studies are needed to assess their applicability to other populations, such as Asian populations, which have different metabolic phenotypes and obesity prevalence. Additionally, patient recruitment was not evenly distributed across Italian regions, which may affect the regional representativeness of the sample. In particular, some regions contributed only a small number of patients, making it difficult to draw reliable conclusions about regional obesity patterns. Moreover, given the registry‐based nature of the study, 60 centers were involved, many of which enrolled only a small number of patients. This prevented us from performing a stratified analysis by center or including the center variable in the PSM, thereby limiting our ability to adjust for inter‐center variability; however, the large number of participating centers may have helped dilute any potential prescription bias, thus enhancing the generalizability of our findings.
Second, BMI has inherent limitations as a measure of adiposity, as it does not differentiate between fat and lean mass or reflect fat distribution, which are more closely linked to CV risk. Nevertheless, BMI was routinary and widely used as a practical surrogate of adiposity in common clinical practice.13, 20, 21
Moreover, our cohort enrolled a low proportion of patients with severe obesity (i.e. second degree or major) so our results in this subgroup of patients were merely exploratory and not conclusive.
Third, we do not have information on the occurrence of each single component of the composite CVE; this limits a detailed analysis of the relevance of each single event type. Similarly, we do not have information on adherence and persistence, which could potentially impact the effectiveness of anticoagulant treatment.
Finally, as common in observational studies, we could not exclude potential unmeasured confounders that may influence the results, although the extensive multivariable adjustment performed in our study took into account several comorbidities and treatments involved in the risk of all‐cause mortality and CVEs.
CONCLUSIONS
5
In conclusion, this real‐world study performed on AF patients showed a high prevalence of overweight and obesity in this population. Furthermore, the treatment with DOACs was independently associated with a lower risk of all‐cause mortality and CVEs compared to VKAs after adjustment for multiple clinical covariates in both overweight and obese patients. These findings seem to support the use of DOACs as an effective and safe therapeutic option across a broad range of elevated BMI categories and highlight the importance of individualized risk assessment beyond BMI alone. However, further studies are needed to confirm our results, especially in patients with extreme BMI and severe obesity degrees.
AUTHOR CONTRIBUTIONS
Danilo Menichelli: conceptualization, formal analysis, writing – original draft. Gianluca Gazzaniga: formal analysis, writing – original draft, visualization. Emilia Antonucci: data curation, methodology, investigation. Gualtiero Palareti: visualization, supervision, writing – review and editing. Daniela Poli: data curation, methodology, investigation. Pasquale Pignatelli: visualization, supervision, writing – review and editing. Daniele Pastori: conceptualization, formal analysis, visualization, supervision, writing – review and editing. All Authors read and approve the last version of the manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare they have no conflict of interest.
Supporting information
Table S1: Schoenfeld Residuals Test for the Proportional Hazards Assumption. (A) Multivariable Cox regression model including predictors significant at univariable analysis. (B) Multivariable Cox regression model including clinically relevant covariates and the interaction between anticoagulant type and BMI class. Table S2: Patients’ characteristics before and after Propensity Score Matching. Table S3: Propensity score matching balance diagnostics. Table S4: Baseline characteristics of obese patients stratified according to obesity class. Table S5: Multivariable Cox Regression for All‐Cause Mortality and Fine‐Grey Model for CVEs, including clinically relevant covariates and an interaction term between Anticoagulant Type and BMI Class. Table S6: Univariable and multivariable cox regression models for predictors of all‐cause mortality in overweight (Panel A) and obese (Panel B) patients. Table S7: Univariable and multivariable fine–grey competing risk models for predictors of cardiovascular events in overweight (Panel A) and obese (Panel B) patients. Table S8: TTR‐stratified analysis of anticoagulant users; multivariable cox regression for all‐cause mortality and fine‐grey model for cardiovascular events (Panel A: TTR ≥60%; Panel B: TTR <60%). Table S9: Univariable cox regression analysis of direct oral anticoagulant use (compared to warfarin) on all‐cause mortality (A) and Fine‐Grey analysis for cardiovascular events (B) according to obesity degree. Figure S1: Geographic distribution of patients of START registry with BMI >25 across Italian regions. Figure S2: Cumulative incidence function of CVE by anticoagulant type. Figure S3: Association of Body Mass Index as a continuous variable with all‐cause mortality as modelled by restricted cubic splines regression analysis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Martin SS , Aday AW , Allen NB , et al. 2025 heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2025;151(8):e 41‐e 660.39866113 10.1161/CIR.0000000000001303 PMC 12256702 · doi ↗ · pubmed ↗
- 2Ng M , Fleming T , Robinson M , et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980‐2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2014;384(9945):766‐781.24880830 10.1016/S 0140-6736(14)60460-8PMC 4624264 · doi ↗ · pubmed ↗
- 3Ortega FB , Lavie CJ , Blair SN . Obesity and cardiovascular disease. Circulation Research. 2016;118(11):1752‐1770.27230640 10.1161/CIRCRESAHA.115.306883 · doi ↗ · pubmed ↗
- 4Koskinas KC , van Craenenbroeck EM , Antoniades C , et al. Obesity and cardiovascular disease: an ESC clinical consensus statement. European Journal of Preventive Cardiology. 2025;32(3):184‐220.39210708 10.1093/eurjpc/zwae 279 · doi ↗ · pubmed ↗
- 5d'Errico M , Pavlova M , Spandonaro F . The economic burden of obesity in Italy: A cost‐of‐illness study. The European Journal of Health Economics. 2022;23(2):177‐192.34347176 10.1007/s 10198-021-01358-1PMC 8882110 · doi ↗ · pubmed ↗
- 6Sha R , Baines O , Hayes A , et al. Impact of obesity on atrial fibrillation pathogenesis and treatment options. Journal of the American Heart Association. 2024;13(1):e 032277.38156451 10.1161/JAHA.123.032277 PMC 10863823 · doi ↗ · pubmed ↗
- 7Huxley RR , Lopez FL , Folsom AR , et al. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: the atherosclerosis risk in communities (ARIC) study. Circulation. 2011;123(14):1501‐1508.21444879 10.1161/CIRCULATIONAHA.110.009035 PMC 3181498 · doi ↗ · pubmed ↗
- 8Wang TJ , Parise H , Levy D , et al. Obesity and the risk of new‐onset atrial fibrillation. JAMA. 2004;292(20):2471‐2477.15562125 10.1001/jama.292.20.2471 · doi ↗ · pubmed ↗