Autoimmune Pulmonary Alveolar Proteinosis Triggered by Salazosulfapyridine in a Patient With Rheumatoid Arthritis: A Case Report
Tomoyuki Ikeuchi, Mitsuhiro Yamamoto, Hirokazu Touge, Naoto Burioka, Akira Yamasaki

TL;DR
An elderly woman with rheumatoid arthritis developed a rare lung condition after taking salazosulfapyridine, likely due to suppressed GM-CSF activity.
Contribution
Identifies a possible mechanism linking SASP treatment, GM-CSF suppression, and autoimmune pulmonary alveolar proteinosis in rheumatoid arthritis.
Findings
The patient showed aPAP features including anti-GM-CSF antibodies and PAS-positive fluid in lung biopsies.
aPAP in RA patients is rare and may result from SASP-induced GM-CSF suppression and antibody production.
This case highlights a paradox in RA pathology involving GM-CSF activity.
Abstract
A 91-year-old woman diagnosed with rheumatoid arthritis (RA) in her 40s achieved disease stabilization after salazosulfapyridine (SASP) treatment. In May 2025, chest computed tomography (CT) revealed bilateral ground-glass opacities with interlobular septal thickening, presenting a crazy-paving pattern. She was diagnosed with autoimmune pulmonary alveolar proteinosis (aPAP) based on positive serum anti-granulocyte-macrophage colony-stimulating factor (GM-CSF) antibodies and periodic acid-Schiff (PAS)-positive fluid accumulation in the alveoli identified on transbronchial lung biopsy (TBLB). The development of aPAP is considered extremely rare in patients with RA, as the disease is typically characterized by elevated GM-CSF activity, creating a pathological paradox. Previous reports have revealed that almost all patients with aPAP and RA receive SASP treatment. We hypothesized that aPAP…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
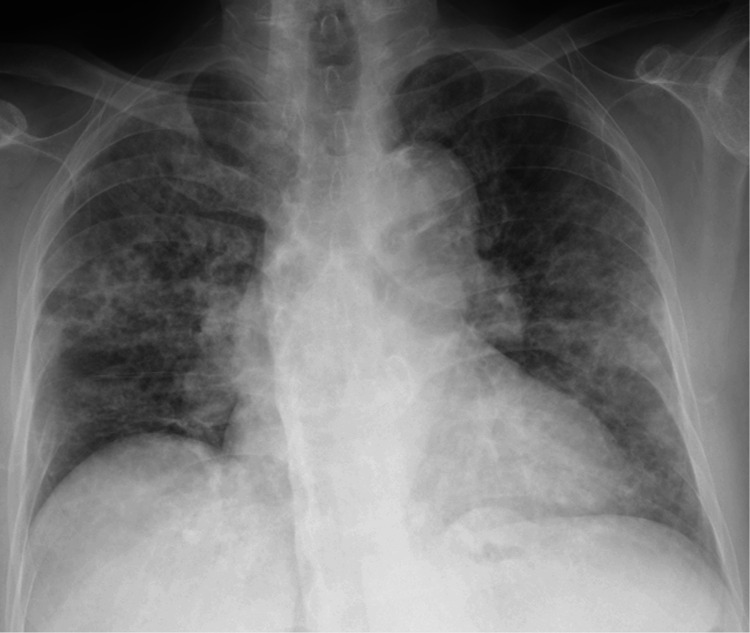 Figure 1
Figure 1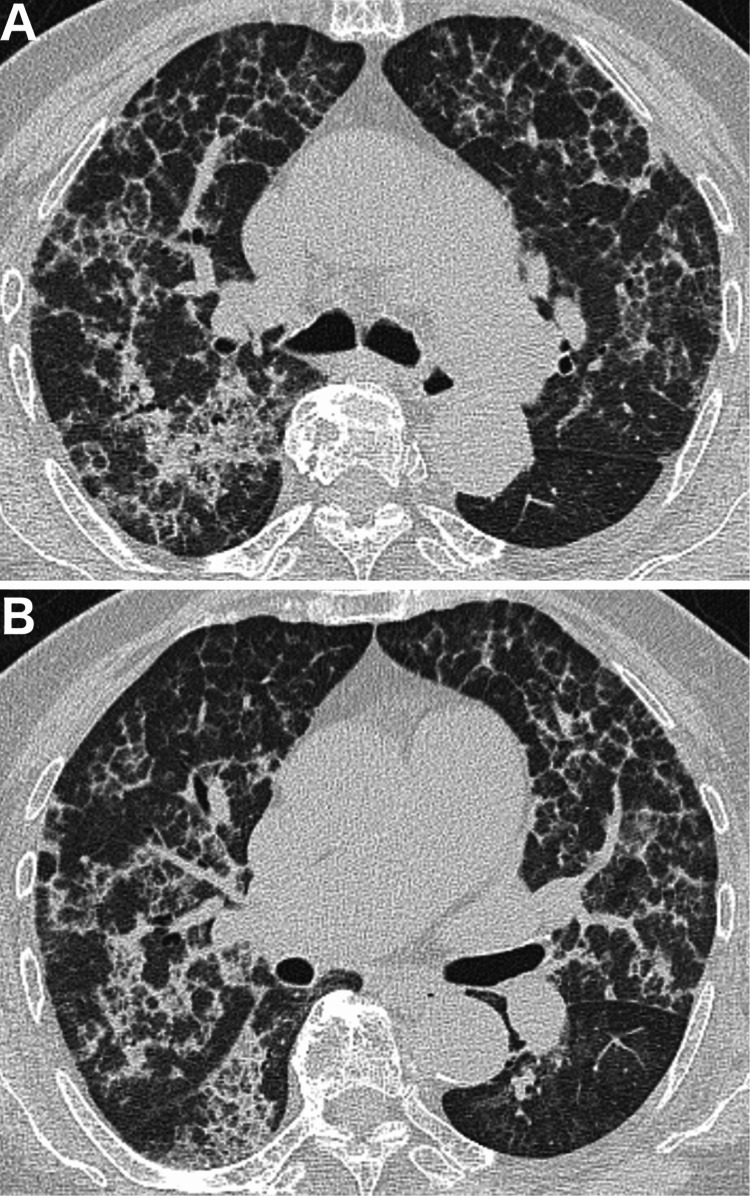 Figure 2
Figure 2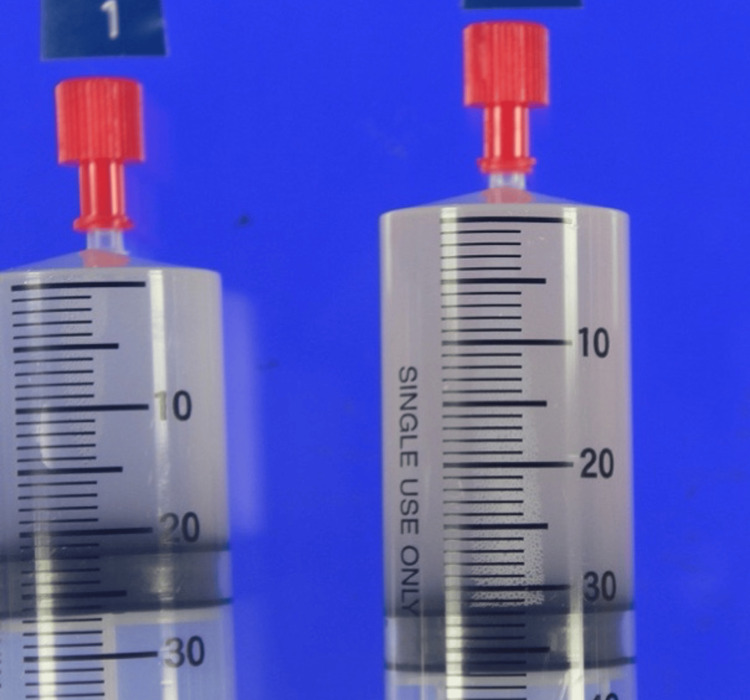 Figure 3
Figure 3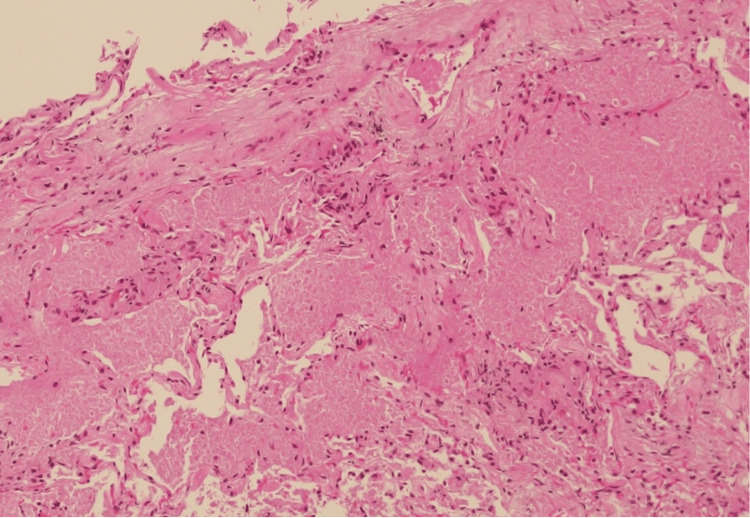 Figure 4
Figure 4| Laboratory test (blood) | Unit | Result | Normal Range |
| Complete blood count | |||
| White blood cells | 1000/μL | 4.6 | 3.3-8.6 |
| Red blood cells | million/μL | 3.58 | 3.86-4.92 |
| Hemoglobin | g/dL | 11.0 | 11.6-14.8 |
| Platelets | '000/μL | 174 | 158-348 |
| Neutrophils | % | 50.0% | 36.0-69.5 |
| Lymphocytes | % | 18.5% | 20.8-52.7 |
| Monocytes | % | 4.2% | 4.5-10.6 |
| Eosinophils | % | 0.3% | 0.5-8.8 |
| Basophils | % | 0.2% | 0.2-1.7 |
| Biochemistry | |||
| Sodium | mmol/L | 144 | 138-145 |
| Potassium | mmol/L | 3.9 | 3.6-4.8 |
| Chloride | mmol/L | 110 | 98-107 |
| Creatinine | mg/dL | 0.6 | 0.46-0.79 |
| Blood urea nitrogen (BUN) | mg/dL | 14 | 8-20 |
| Glucose | mg/dL | 118 | 73-109 |
| Protein, total | g/dL | 7.7 | 6.6-8.1 |
| Albumin | g/dL | 3.8 | 4.1-5.1 |
| Globulin | g/dL | 3.4 | 2.2-3.4 |
| Albumin/globulin Ratio | 1.1 | 1.32-2.23 | |
| Bilirubin, total | mg/dL | 0.5 | 0.4-1.5 |
| Alanine transaminase | U/L | 13 | 7-23 |
| Aspartate aminotransferase | U/L | 23 | 13-30 |
| Alkaline phosphatase | U/L | 107 | 38-113 |
| Serum | |||
| CRP | mg/dL | 0.02 | 0-0.14 |
| Sialylated carbohydrate antigen KL-6 | U/mL | 1200 | 0-500 |
| Pulmonary surfactant protein D (SP-D) | ng/mL | 276 | <110 |
| Pulmonary surfactant protein A (SP-A) | ng/mL | 64.7 | 0-43.8 |
| Anti-granulocyte-macrophage colony-stimulating factor (GM-CSF) antibody | positive | negative(<3.5U/mL) | |
| β-D-glucan | pg/mL | 25.6 | 0-20 |
| IgG | mg/dL | 1349 | 861-1747 |
| Rheumatoid factor (RF) | IU/mL | 222 | 0-15 |
| Matrix metalloproteinase-3 (MMP-3) | mg/mL | 55.0 | 17.3-59.7 |
| Arterial blood gas analysis (room air) | |||
| pH | 7.41 | 7.35-7.45 | |
| PaCO2 (partial pressure of carbon dioxide) | Torr | 37.4 | 35-45 |
| PaO2 (partial pressure of oxygen) | Torr | 61.9 | 75-100 |
| HCO3- | mmol/L | 23.1 | 22-26 |
| A-aDO2 | Torr | 41.1 | ≤10 |
| Pulmonary function test | |||
| FVC (Forced vital capacity) | L | 1.45(85.9%) | 1.48(reference value) |
| FEV1 (Forced expiratory volume in one second) | L | 1.09(103.8%) | 1.05(reference value) |
| FEV1% (FEV1/FVC) | % | 75.2 | ≥70 |
| %DLCO (carbon monoxide diffusing capacity) | % | 77.4 | 80-120 |
| Reporting year | Reference No. | Sex | Age | RF (IU/mL) | Duration of RA treatment | DMARDs | Symptoms | anti-GM-CSF antibody (U/mL) | Treatments |
| 2006 | Wardwell et al., 2006 [ | Male | 42 | Not listed | One month | LEF+PSL | SOB | Negative | WLL, withdrawal of LEF |
| 2017 | Ito et al., 2017 [ | Female | 65 | 29.3 | Five years | SASP+MTX | DOE, DC | 26.1 | WLL, GI, CS |
| 2017 | Ito et al., 2017 [ | Female | 68 | 238.3 | 26 years | SASP | DOE | 42.3 | WLL, GI |
| 2020 | Hashimoto et al., 2020 [ | Male | 70 | 110.5 | Five years | SASP | DC | 40.5 | Expectorant |
| - | Present case | Female | 91 | 222.0 | 45 years | SASP | DOE | Positive (>3.5) | GI |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Neonatal Respiratory Health Research · Proteoglycans and glycosaminoglycans research
Introduction
Pulmonary alveolar proteinosis (PAP) is a disorder in which pulmonary surfactant abnormally accumulates in the alveolar spaces due to disruption in surfactant production or clearance processes, resulting in respiratory failure. Based on etiology, PAP is categorized as autoimmune, secondary, congenital, or unclassified. Autoimmune pulmonary alveolar proteinosis (aPAP) represents approximately 90% of all PAP cases [1]. In patients with aPAP, granulocyte-macrophage colony-stimulating factor (GM-CSF) in the lungs is neutralized by autoantibodies, resulting in impaired maturation of alveolar macrophages and subsequent accumulation of pulmonary surfactant. In contrast, in patients with rheumatoid arthritis (RA), GM-CSF is overexpressed as an inflammatory cytokine, and a monoclonal antibody against GM-CSF receptor is being investigated as novel therapeutic agents [2]. Thus, aPAP and RA represent contradictory pathological conditions: aPAP is characterized by insufficient GM-CSF activity, whereas RA is characterized by excessive GM-CSF. Therefore, the coexistence of both diseases is extremely rare [3]. This patient had comorbid RA and underwent salazosulfapyridine (SASP) treatment. Herein, we present a case of aPAP diagnosed in a patient with RA, discussing the diagnostic approach and exploring a potential link to SASP therapy. We reviewed previously reported cases of aPAP associated with RA and discussed the presumed pathogenic mechanisms.
Case presentation
A 91-year-old woman presented with dyspnea upon exertion, with ground-glass opacities in both lung fields. She had been diagnosed with RA in her 40s. The patient’s condition stabilized with SASP treatment, and she was being managed at a local clinic. During a routine visit in May 2025, chest radiography and computed tomography (CT) revealed ground-glass opacities in both lung fields. A follow-up chest CT performed three weeks later showed enlargement of the opacities. Dyspnea on exertion persisted; however, the patient had no other accompanying symptoms, including cough, sputum production, or fever. the patient was referred to our department for further investigation. She had no history of smoking or exposure to dust.
On physical examination, the patient had a blood pressure of 120/71 mmHg, a heart rate of 73 bpm, a respiratory rate of 20/min, an oxygen saturation of 93% on room air, and a temperature of 36.8°C. Her breath sounds were clear, and her fingers and limb joints showed no tenderness or deformities.
Chest radiography revealed diffuse reticular ground-glass opacities in both lungs (Figure 1). Chest CT revealed bilateral ground-glass opacities with interlobular septal thickening, presenting a crazy-paving pattern (Figure 2). The laboratory test results are presented in Table 1. Complete blood count, serum biochemistry, and C-reactive protein (CRP) levels were within normal limits. Sialylated carbohydrate antigen KL-6, pulmonary surfactant protein D (SP-D), and pulmonary surfactant protein A (SP-A) levels were elevated. Rheumatoid factor (RF) levels were elevated, whereas matrix metalloproteinase-3 (MMP-3) levels were within the normal range. RA disease activity was well controlled, with a DAS28-CRP level of 1.2. Anti-GM-CSF antibodies were detected using a simple serum diagnostic kit. Arterial blood gas analysis revealed mild respiratory failure and elevated A-aDO₂ levels. Pulmonary function testing revealed a decrease in %DLCO (diffusing capacity of the lungs for carbon monoxide).
Chest X-ray at the initial visitChest X-ray showed bilateral ground-glass opacities.
Chest CT scan at the time of diagnosisChest computed tomography (CT) revealed interlobular septal thickening against a background of ground-glass opacities, presenting a crazy-paving pattern. A. CT slice at the carinal level. B. CT slice at the middle lobe and lingular level.
Bronchoalveolar lavage (BAL) was performed in the left B^4b^ and transbronchial lung biopsy (TBLB) was obtained from the left B^3^. The BAL fluid appeared turbid and milky white (Figure 3). The recovery rate was 98/150 mL (65%). Total cell count was 277 cells/μL; a cell differential could not be performed due to significant cell disruption, a finding often associated with PAP due to fragile, lipid-laden macrophages. The mean CD4/CD8 ratio was 0.69. Cultures for common bacteria and acid-fast bacilli were negative. TBLB (Figure 4) showed preserved alveolar architecture, with pale eosinophilic material positive for periodic acid-Schiff (PAS) staining within the alveolar spaces.
Appearance of the BAL fluidThe bronchoalveolar lavage fluid (BALF) was milky white. Cytological examination revealed benign findings, with scattered ciliated columnar epithelial cells and alveolar macrophages against a background of periodic acid-Schiff (PAS)-positive material.
Histopathology of the lung (lt. B3, hematoxylin and eosin (H&E) stain)The alveolar structure remains intact. Pale eosinophilic periodic acid-Schiff (PAS)-positive material was observed in the alveolar spaces.
The patient was diagnosed with aPAP based on the presence of anti-GM-CSF antibodies. Inhalation therapy with sargramostim, a GM-CSF agent, was initiated in July 2025. Since RA was well controlled with SASP treatment, SASP therapy was continued. Chest CT scan was performed approximately one month later, in August, showed improvement in ground-glass opacities in the right lower lobe. Arterial blood gas analysis on September revealed PaO₂ of 64.2 Torr and A-aDO₂, of 38.8 Torr, indicating slight improvement. The planned treatment regimen, one week of inhalation therapy followed by one week off, will be repeated for up to 12 cycles [4].
Discussion
aPAP and RA represent contradictory pathological conditions, and their coexistence is extremely rare. A PubMed search for cases of concurrent aPAP and RA identified only four previously reported cases (Table 2) [3,5,6]. Including the present case, we were able to identify five cases. Of these five cases, four patients received SASP for RA treatment. In one case treated with leflunomide and prednisone [5], the anti-GM-CSF antibody test was negative, and drug-induced PAP was suspected.
Orally administered SASP is metabolized by intestinal bacteria into sulfapyridine (SP) and 5-aminosalicylic acid. The therapeutic effect in RA is primarily attributed to SP, which is readily absorbed, and previous clinical trials [7] have demonstrated that SP alone achieves efficacy comparable to that of SASP. SASP has multiple effects on the immune system, which are thought to include the suppression of antibody production through B-cell inhibition, suppression of inflammatory cytokines, and modulation of signal transduction pathways, including inhibition of nuclear transcription factors such as NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) [8-10]. We hypothesize that SASP, through its known inhibition of NF-κB and other immunomodulatory pathways, may indirectly suppress GM-CSF signaling or production within the alveolar microenvironment. Clinical data observations indirectly supporting this association include several reported cases of SASP-induced agranulocytosis that recovered rapidly with GM-CSF administration [11].
Previous studies have measured SP and SASP in the synovial fluid of patients with RA treated with SASP [12,13]. SP and SASP are systemically well absorbed from the colon and are presumed to have a high tissue distribution. The immunomodulatory effects of SP and SASP on the lungs may suppress GM-CSF activity within the alveoli. We propose a 'dual-hit' pathogenesis: first, SASP may partially suppress local GM-CSF activity, creating a permissive environment; second, the acquired production of anti-GM-CSF antibodies provides the final, critical hit that neutralizes GM-CSF sufficiently to cause impaired surfactant clearance and clinical aPAP. We speculate that under these circumstances, anti-GM-CSF antibodies were acquired, leading to dual suppression of GM-CSF, and a subsequent decline in its concentrations to a level that promoted pulmonary surfactant accumulation. Similar to other rare and fatal treatment-induced complications in chronic systemic disease, our case of SASP-triggered aPAP underscores that even standard, long-used therapies can uncommonly precipitate life-threatening conditions [14]. This reality demands heightened clinical vigilance to ensure timely diagnosis and intervention.
Conclusions
As GM-CSF levels are elevated in patients with RA, the development of aPAP is rare. We reviewed previous reports, including the present case, on the development of aPAP in a patient with RA. Notably, four out of the five reported cases, including ours, were associated with SASP treatment, suggesting a potential drug-specific trigger rather than a mere association with RA itself. Because SASP exhibits GM-CSF-suppressive effects and high tissue distribution in the lungs, its administration suppresses GM-CSF activity within the alveoli. In addition, acquired anti-GM-CSF antibodies result in the dual suppression of GM-CSF, leading to the development of aPAP. When respiratory symptoms or pulmonary abnormalities develop in patients with RA receiving SASP, pulmonary alveolar proteinosis should be considered in the differential diagnosis. The present case was managed with inhaled sargramostim (GM-CSF agent) therapy. Further investigation is required to determine the most appropriate treatment for these pathological conditions, including SASP withdrawal.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Assessment and management of pulmonary alveolar proteinosis in a reference center Orphanet J Rare Dis Campo I Mariani F Rodi G 40820132349754610.1186/1750-1172-8-40PMC 3605309 · doi ↗ · pubmed ↗
- 2Targeting GM-CSF in rheumatoid arthritis Clin Exp Rheumatol Avci AB Feist E Burmester GR 044342016 https://www.clinexprheumatol.org/abstract.asp?a=1086227586802 · pubmed ↗
- 3A case of autoimmune pulmonary alveolar proteinosis complicated by rheumatoid arthritis Annals of the Japanese Respiratory Society Hashimoto M Suga K Hatakeyama T Horibe R Nishiyama K 47748192020 http://journal.jrs.or.jp/detail_e.php?-DB=jrs&-recid=17882&-action=browse
- 4Inhaled GM-CSF for pulmonary alveolar proteinosis N Engl J Med Tazawa R Ueda T Abe M 92393238120193148396310.1056/NEJ Moa 1816216 · doi ↗ · pubmed ↗
- 5Pulmonary alveolar proteinosis associated with a disease-modifying antirheumatoid arthritis drug Respirology Wardwell NR Jr Miller R Ware LB 6636651120061691634510.1111/j.1440-1843.2006.00905.x · doi ↗ · pubmed ↗
- 6Two cases of autoimmune pulmonary alveolar proteinosis with rheumatoid arthritis Allergol Int Ito S Wakahara K Kojima T Takahashi N Nishiwaki K Yamaguchi E Hasegawa Y 5075096620172824219910.1016/j.alit.2017.02.002 · doi ↗ · pubmed ↗
- 7Which component of sulphasalazine is active in rheumatoid arthritis?Br Med J (Clin Res Ed) Pullar T Hunter JA Capell HA 15351538290198510.1136/bmj.290.6481.1535 PMC 14157522860942 · doi ↗ · pubmed ↗
- 8Regulation of human B cell function by sulfasalazine and its metabolites Int Immunopharmacol Hirohata S Ohshima N Yanagida T Aramaki K 631640220021201350310.1016/s 1567-5769(01)00186-2 · doi ↗ · pubmed ↗