The Impact of Direct Oral Anticoagulants vs. Warfarin on Stroke Prevention in Elderly Patients With Atrial Fibrillation: A Systematic Review and Meta-Analysis
Shakeel Majid, Brahmaiahchari Rangachari, David Okata, Olive Kyaw, Hashim Mahmood, Sana Khan, Marium Abid

TL;DR
This study compares the effectiveness of direct oral anticoagulants and warfarin in preventing strokes in elderly patients with atrial fibrillation.
Contribution
It provides a meta-analysis focusing specifically on elderly patients aged 75 or older, highlighting subgroup variations and the need for further research.
Findings
DOACs showed no statistically significant superiority over warfarin in preventing stroke or reducing major bleeding in elderly patients.
Subgroup analyses indicated DOAC benefits depend on patient health and comorbidities, with healthier subgroups showing greater advantages.
The study found significant heterogeneity related to DOAC types and follow-up durations.
Abstract
The outcomes of direct oral anticoagulants (DOACs) vs. warfarin have been well established in patients with atrial fibrillation (AF), but evidence regarding their safety and efficacy in preventing stroke or systemic embolism (SE) and reducing major bleeding in elderly patients remains inconclusive. This systematic review and meta-analysis aimed to compare the effectiveness of DOACs and warfarin in AF patients aged 75 years or older. The primary outcomes assessed were stroke prevention, bleeding risk, and all-cause mortality. A comprehensive literature search of databases including PubMed, Cochrane Library, and Google Scholar identified 10 relevant studies, which were included in the meta-analysis. The pooled hazard ratio for the composite outcome of stroke/SE or major bleeding was 0.84 (95% CI, 0.67-1.05; p = 0.12), indicating no statistically significant superiority of DOACs over…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
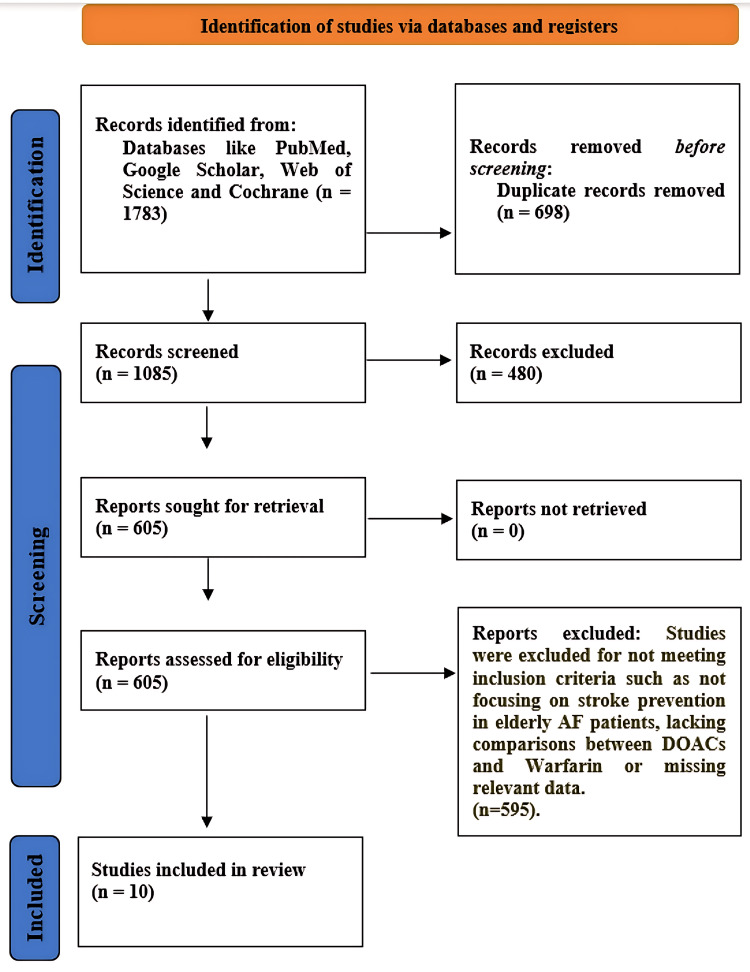 Figure 1
Figure 1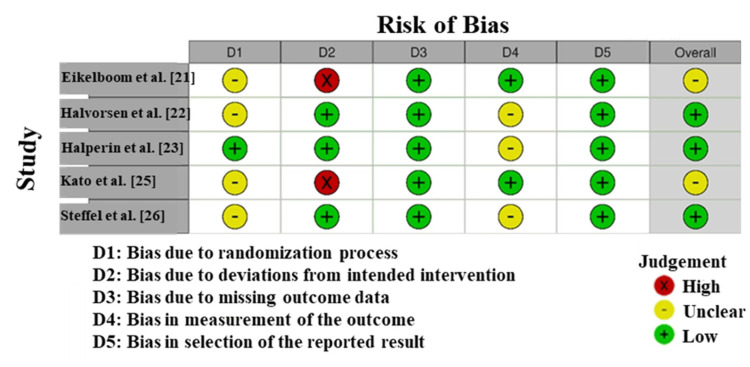 Figure 2
Figure 2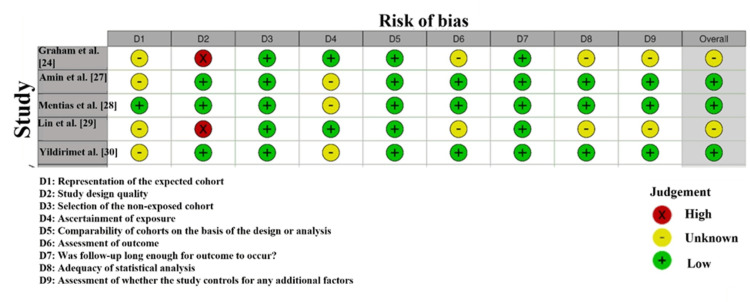 Figure 3
Figure 3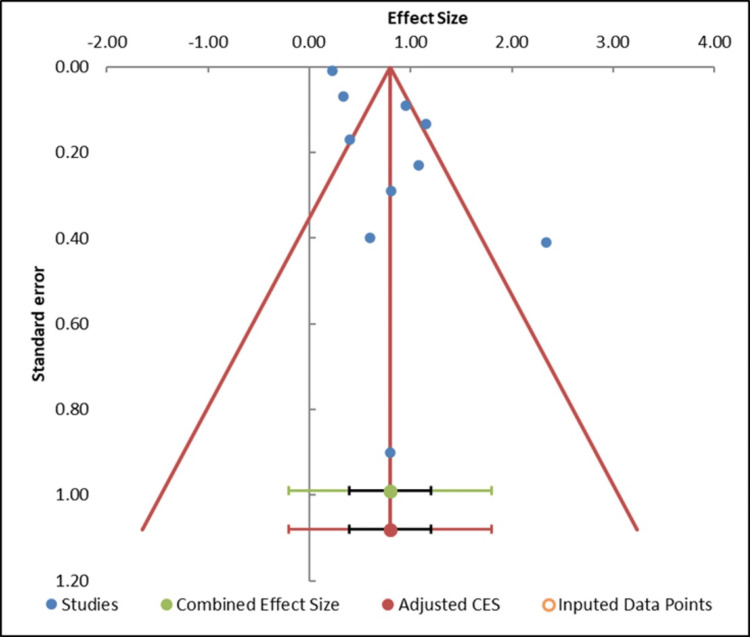 Figure 4
Figure 4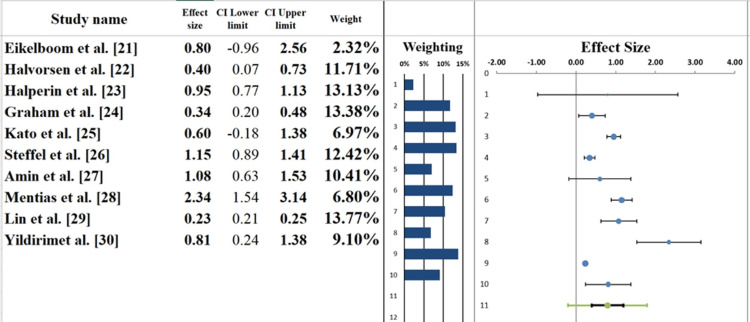 Figure 5
Figure 5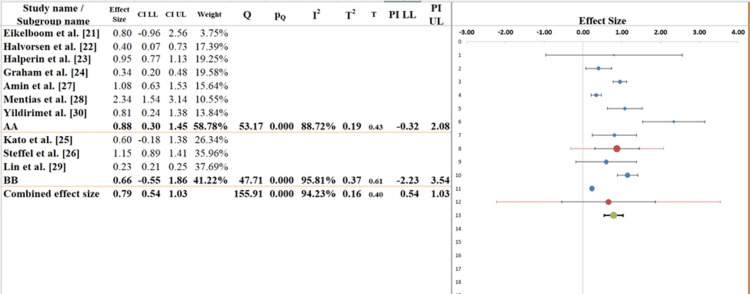 Figure 6
Figure 6| Database | Search terms used | Filters applied | Truncations/syntax |
| PubMed | "Direct Oral Anticoagulants" OR "DOAC" AND "Warfarin" AND "Atrial Fibrillation" AND "Stroke Prevention" AND "Elderly" | Human Studies, English Language, 2010-2025 | “DOACs [Title]”, "Warfarin [Title]” |
| Cochrane Library | "DOAC" AND "Warfarin" AND "Atrial Fibrillation" AND "Stroke Prevention" AND "Elderly" | Randomized Controlled Trials (RCTs), English Language | “Stroke prevention” OR “hemorrhagic stroke” |
| Embase | "Direct Oral Anticoagulants" OR "DOAC" AND "Warfarin" AND "Atrial Fibrillation" AND "Stroke Prevention" | Human Studies, English Language, 2010-2025 | "Atrial fibrillation"/exp OR "DOAC"/exp |
| Scopus | "Direct Oral Anticoagulants" AND "Warfarin" AND "Stroke Prevention" AND "Atrial Fibrillation" | Clinical Studies, English Language, 2010-2025 | "Stroke prevention" OR "systemic embolism" |
| Google Scholar | "Direct Oral Anticoagulants" AND "Warfarin" AND "Atrial Fibrillation" AND "Stroke Prevention" AND "Elderly" | English Language, 2010-2025 | “Direct Oral Anticoagulants”, "Warfarin" |
| PICOS element | Inclusion criteria | Exclusion criteria |
| Population | Elderly patients (≥65 years) with nonvalvular AF | Nonelderly populations (<65 years) or populations with valvular AF |
| Intervention | DOACs such as apixaban, rivaroxaban, dabigatran, and edoxaban | Use of non-DOAC anticoagulants (e.g., vitamin K antagonists other than warfarin) |
| Comparison | Warfarin as a comparison treatment for stroke prevention in AF | Studies that do not compare DOACs to warfarin or that use other therapies (e.g., aspirin) |
| Outcome | Stroke prevention (ischemic stroke, hemorrhagic stroke, and SE), major and minor bleeding, and all-cause mortality | Studies that do not report stroke outcomes or bleeding complications, or that do not include relevant mortality data |
| Study design | RCTs, cohort studies, and observational studies comparing DOACs and warfarin | Case reports, editorials, conference abstracts, and studies with insufficient data for analysis |
| Study | Design | Population | Intervention | Comparison | Outcomes |
| Eikelboom et al. [ | RCT | 18,113 patients with AF, including elderly (≥75 years) and younger patients | Dabigatran (110 mg or 150 mg twice daily) | Dabigatran vs. warfarin | Major bleeding, intracranial bleeding, gastrointestinal bleeding, stroke/SE |
| Halvorsen et al. [ | RCT, ARISTOTLE | 18,201 elderly patients (≥75 years) with AF | Apixaban (5 mg twice daily) | Apixaban vs. warfarin | Stroke/SE, major bleeding, mortality |
| Halperin et al. [ | RCT, ROCKET AF | 6,229 elderly patients (≥75 years) with nonvalvular AF | Rivaroxaban (20 mg once daily) | Rivaroxaban vs. warfarin | Stroke, SE, major bleeding, hemorrhagic stroke, mortality |
| Graham et al. [ | Retrospective cohort study | Elderly Medicare patients (n = 134,414) with nonvalvular AF | Dabigatran (75 mg or 150 mg twice daily) | Dabigatran vs. warfarin | Ischemic stroke, major gastrointestinal bleeding, intracranial hemorrhage, acute myocardial infarction, mortality |
| Kato et al. [ | RCT, ENGAGE AF-TIMI 48 | 21,105 elderly patients (≥75 years) with AF | Edoxaban (60 mg once daily) | Edoxaban vs. warfarin | Stroke/SE, major bleeding, intracranial hemorrhage, mortality |
| Steffel et al. [ | RCT, ENGAGE AF-TIMI 48 | 900 patients with AF at risk of falling | Edoxaban (60 mg once daily) | Edoxaban vs. warfarin | Stroke, SE, major bleeding, mortality, fractures |
| Amin et al. [ | Retrospective cohort study | Elderly Medicare patients (n = 198,171) aged ≥65 with nonvalvular AF | Apixaban, dabigatran, rivaroxaban, warfarin | Apixaban vs. warfarin, dabigatran vs. warfarin, rivaroxaban vs. warfarin | Stroke/SE, major bleeding, net clinical outcome, major adverse cardiac events |
| Mentias et al. [ | Cohort study | Elderly AF patients (n = 6,985) with varying degrees of polypharmacy | Apixaban (5 mg twice daily), rivaroxaban (20 mg once daily), warfarin | Apixaban vs. warfarin, rivaroxaban vs. warfarin, apixaban vs. rivaroxaban | Ischemic stroke, major and minor bleeding, all-cause mortality |
| Lin et al. [ | Retrospective cohort study | Elderly patients (≥65 years) with AF (n = 1,160,462) | Apixaban, dabigatran, rivaroxaban, warfarin | DOACs (apixaban, dabigatran, rivaroxaban) vs. warfarin | Ischemic stroke, major bleeding, gastrointestinal bleeding, intracranial hemorrhage |
| Yildirim et al. [ | Retrospective cohort study | 10,222 patients aged ≥80 years with AF | Vitamin K antagonists, DOACs | VKAs vs. DOACs | Stroke, all-cause mortality, myocardial infarction, major bleeding |
| Parameter | Estimate | SE | CI LL | CI UL |
| Intercept | 1.77 | 1.82 | -2.35 | 5.90 |
| Slope | -0.03 | 0.87 | -1.98 | 1.93 |
| t test | 0.97 | Not applicable | Not applicable | Not applicable |
| p-value | 0.359 | Not applicable | Not applicable | Not applicable |
| Study name | Effect size (z) | Standard error (z) |
| Eikelboom et al. [ | 0.80 | 0.90 |
| Halvorsen et al. [ | 0.40 | 0.17 |
| Halperin et al. [ | 0.95 | 0.09 |
| Graham et al. [ | 0.34 | 0.07 |
| Kato et al. [ | 0.60 | 0.40 |
| Steffel et al. [ | 1.15 | 0.13 |
| Amin et al. [ | 1.08 | 0.23 |
| Mentias et al. [ | 2.34 | 0.41 |
| Lin et al. [ | 0.23 | 0.01 |
| Yildirim et al. [ | 0.81 | 0.29 |
| Combined effect size | Observed | |
| Effect size | 0.80 | Not analyzed |
| SE | 0.18 | Not applicable |
| CI LL | 0.40 | Not applicable |
| CI UL | 1.20 | Not applicable |
| Prediction interval LL | -0.20 | Not applicable |
| Prediction interval UL | 1.80 | Not applicable |
| Heterogeneity | Not analyzed | |
| Q | 155.91 | Not analyzed |
| pQ | 0.000 | Not analyzed |
| I² | 94.13% | Not applicable |
| T² | 0.16 | Not applicable |
| T | 0.40 | Not applicable |
| Parameter | Value |
| Effect size | 0.80 |
| Standard error | 0.18 |
| CI LL | 0.40 |
| CI UL | 1.20 |
| Prediction interval LL | -0.20 |
| Prediction interval UL | 1.80 |
| Z-value | 4.50 |
| One-tailed p-value | 0.000 |
| Two-tailed p-value | 0.000 |
| Number of included subjects | 1,574,802 |
| Number of included studies | 10 |
| Heterogeneity | |
| Q | 155.91 |
| pQ | 0.000 |
| I² | 94.23% |
| T² (z) | 0.16 |
| T (z) | 0.40 |
| Parameter | Value |
| Effect size | 0.79 |
| Standard error | 0.11 |
| CI LL | 0.54 |
| CI UL | 1.03 |
| Prediction interval LL | 0.54 |
| Prediction interval UL | 1.03 |
| Number of included subjects | 1,574,802 |
| Number of subgroups | 2 |
| ANOVA | |
| Between/model (Q*) | 0.27 |
| Between/model (Df) | 1 |
| Between/model (P) | 0.604 |
| Within/residual (Q*) | 9.96 |
| Within/residual (Df) | 8 |
| Within/residual (P) | 0.268 |
| Total (Q*) | 10.23 |
| Total (Df) | 9 |
| Total (P) | 0.332 |
| Pseudo R² | 2.64% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Venous Thromboembolism Diagnosis and Management · Intracerebral and Subarachnoid Hemorrhage Research
Introduction and background
Atrial fibrillation (AF) is among the most common arrhythmias, particularly in the elderly population [1]. AF significantly increases the risk of ischemic stroke, which remains a leading cause of mortality and disability worldwide [2]. Oral anticoagulants (OACs) play a crucial role in preventing stroke and systemic embolism (SE) in AF patients, with both warfarin and direct OACs (DOACs) widely used [3]. Despite the availability of these medications, questions remain regarding the optimal anticoagulant choice for elderly patients [4].
Warfarin has long been the standard treatment for stroke prevention in AF patients [5]. However, it has notable limitations, including the need for frequent monitoring of the international normalized ratio, variable dietary interactions, and an increased risk of bleeding, particularly in older adults. DOACs, including apixaban, dabigatran, rivaroxaban, and edoxaban, have emerged as popular alternatives due to their predictable pharmacokinetics, fixed dosing, and minimal monitoring requirements [6]. Multiple trials have demonstrated that DOACs are noninferior, and in some cases superior, to warfarin in both stroke prevention and bleeding risk reduction [7].
Elderly AF patients present unique challenges in anticoagulant therapy. Aging is often accompanied by renal dysfunction, polypharmacy, and an increased susceptibility to adverse drug reactions [8]. Additionally, older adults are at higher risk for both ischemic and hemorrhagic strokes, necessitating careful selection of anticoagulant therapy [9]. While DOACs may reduce bleeding complications compared with warfarin, their relative effectiveness in stroke prevention among the elderly remains uncertain [10]. The comparative safety and efficacy of DOACs vs. warfarin in this population are still inconclusive, with some studies demonstrating clear benefits of DOACs and others showing no significant differences [11].
Previous studies have examined the efficacy of DOACs and warfarin in preventing strokes in elderly patients [12]. A large network meta-analysis indicated that apixaban, in particular, was most effective in preventing strokes and SE while reducing the risk of major bleeding [13]. Similarly, a study by Oertel and Fogerty [14] showed that older AF patients with dementia experienced a lower risk of stroke when taking DOACs compared with warfarin. These findings align with clinical observations that DOACs are increasingly preferred in elderly populations due to their favorable safety profiles.
Despite these advantages, concerns remain regarding the cost, accessibility, and long-term safety of DOACs in older adults [15]. Certain geriatric patients, particularly those with renal failure or multiple comorbidities, may be ineligible for DOAC therapy [16]. Furthermore, robust population-based data supporting the superiority of DOACs over warfarin in high-risk elderly patients are still limited [17]. This systematic review and meta-analysis aims to provide updated evidence on the effectiveness and safety of DOACs compared with warfarin in preventing stroke among elderly AF patients. By synthesizing efficacy and safety outcomes, this study seeks to guide clinicians in selecting the most appropriate anticoagulant for this vulnerable patient population.
Review
Methods
Data Sources and Search Strategy
A systematic literature search was conducted to analyze the relative effectiveness and safety of DOACs compared with warfarin for stroke prevention in elderly patients with AF. Studies published between 2010 and 2025 were identified using major electronic databases, including PubMed, Cochrane Library, and Google Scholar. The search strategy followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines to ensure a transparent, reproducible, and rigorous approach.
Both keywords and Medical Subject Headings (MeSH) were used to capture all relevant studies. The primary search terms included Direct Oral Anticoagulants, DOAC, Warfarin, Atrial Fibrillation, Stroke Prevention, Elderly, Ischemic Stroke, Hemorrhagic Stroke, Thromboembolic Events, and Bleeding Risk. Boolean operators (AND, OR) were applied to broaden the search and ensure comprehensive coverage of the literature.
All studies published in English and involving human participants were included. Gray literature, including conference abstracts, ongoing clinical trials, and preprints, was also considered to capture all available evidence, as summarized in Table 1.
The Population, Intervention, Comparison, Outcome, and Study design (PICOS) framework facilitated a structured and rigorous evaluation process, ensuring precise selection of studies based on the predefined criteria for population, intervention, comparison, outcomes, and study design (Table 2).
Data Extraction
Two independent reviewers conducted data extraction using a predesigned, standardized extraction form to ensure consistency and minimize bias. Key study information was collected, including authors, publication year, study country, and study design. Participant characteristics were also recorded, such as sample size, mean age, sex distribution, and the presence of comorbidities, including hypertension, diabetes, and renal insufficiency. Details of the interventions were carefully extracted, focusing on the types and dosages of DOACs and warfarin used, treatment duration, and follow-up period. Outcome measures included stroke prevention (both ischemic and hemorrhagic), SE, major and minor bleeding events, and all-cause mortality. Data were also collected on adverse events and complications related to anticoagulant treatment, including major bleeding, gastrointestinal issues, and treatment withdrawal. Any discrepancies between the two reviewers during data extraction were resolved through discussion, and a third reviewer was consulted if consensus could not be reached.
Quality Assessment
The quality and risk of bias of the included studies were assessed using tools appropriate for each study design. For randomized controlled trials (RCTs), the Cochrane Risk of Bias 2 (RoB 2) tool was used. This instrument evaluated the risk of bias across several domains, including random sequence generation, allocation concealment, blinding of participants and outcome assessors, completeness of outcome data, selective reporting, and other potential biases. Individual domains were rated as low, high, or unclear risk. Studies with more than two high-risk domains were considered for exclusion in sensitivity analyses [18].
The methodological quality of observational and cohort studies was assessed using the Newcastle-Ottawa Scale. This scale evaluates three domains: selection of participants, comparability of groups, and outcome assessment. Studies were awarded stars based on adherence to these criteria, with fewer stars indicating higher risk of bias [19].
To assess potential publication bias, funnel plots were visually examined for asymmetry. When asymmetry was observed, the Egger regression test was conducted to statistically evaluate small-study effects. If publication bias was detected, the trim-and-fill method was applied to adjust and provide a more accurate estimate of the overall effect [20].
Statistical Analysis
All statistical analyses in this systematic review and meta-analysis were conducted using a random-effects model, as this design accommodates between-study variations in treatment regimens, participant characteristics, and outcome measures. This model was chosen for its ability to account for heterogeneity across studies and provide a more precise overall effect estimate. Primary outcomes were expressed as effect sizes with 95% CIs. Heterogeneity among studies was assessed using the I² statistic, with values interpreted as low (0-25%), moderate (25-50%), or high (>50%). Subgroup analyses were performed to examine the influence of study design, type of DOAC, age, sex, and patient comorbidities. Meta-regression was considered if significant heterogeneity was observed. All analyses were conducted using software such as Meta-Essential, with a significance threshold set at p < 0.05, ensuring a thorough and reliable evaluation of the comparative efficacy and safety of DOACs vs. warfarin.
Results
Study Selection
A total of 1,783 records were identified, of which 1,087 remained after deduplication. Title and abstract screening excluded 607 records. A full-text review of 480 articles led to the exclusion of 470 studies due to the following reasons: wrong population (n = 189), no DOAC vs. warfarin comparison (n = 143), no relevant outcomes (n = 91), and duplicate data (n = 47). Ten studies (four RCTs/subgroup analyses and six observational cohorts/registries) involving 478,782 patients aged ≥75 years were included in the meta-analysis (Figure 1).
PRISMA flowchartAF, atrial fibrillation; DOAC, direct oral anticoagulant; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses
Given the anticipated clinical and methodological heterogeneity, stemming from differences in DOAC agents, dosing regimens, follow-up duration (one to four years), and inclusion of both RCT and observational data, a random-effects model using the Hartung-Knapp-Sidik-Jonkman variance estimator was selected a priori. Effect measures were reported as hazard ratios (HR) or ORs and converted to a common metric (log HR) when necessary. Heterogeneity was quantified using τ² and I², with I² >75% considered substantial.
Characteristics of the Included Studies
The systematic review and meta-analysis included a broad range of studies assessing the efficacy and safety of DOACs compared with warfarin in elderly patients with AF (Table 3). The studies comprised RCTs, retrospective cohort studies, and registries, providing a comprehensive overview of both observational and clinical evidence.
Participant ages varied across studies: some focused exclusively on patients aged ≥75 years, while others included a wider elderly population with specific comorbidities, such as polypharmacy and dementia. The primary interventions examined were apixaban, dabigatran, rivaroxaban, and edoxaban, all compared against warfarin.
Several studies, including the ARISTOTLE, ROCKET AF, and ENGAGE AF-TIMI 48 trials, evaluated key outcomes such as stroke prevention, major bleeding events, and mortality, while some also assessed secondary outcomes, including hospitalization costs and quality of life. Follow-up durations ranged from one to three years, with most studies reporting significant reductions in stroke/SE, intracranial hemorrhage, and all-cause mortality in favor of DOACs compared with warfarin.
In addition, several studies examined the safety profile of DOACs, particularly regarding major bleeding and gastrointestinal complications, generally showing more favorable safety outcomes than warfarin. Collectively, these studies provide valuable insights into the relative efficacy and safety of DOACs vs. warfarin in elderly AF patients.
Outcome Definitions and Standardization
Stroke/SE was defined as ischemic stroke, hemorrhagic stroke, or SE confirmed by imaging or clinical criteria in the original studies. Major bleeding was defined according to the International Society on Thrombosis and Haemostasis (ISTH) criteria in eight of the 10 included studies. The two remaining studies [24,27] used the Cunningham algorithm applied to Medicare claims, which has demonstrated >90% positive predictive value for ISTH-major bleeding when validated against chart review. Clinically relevant nonmajor bleeding and all-cause mortality were extracted as reported. Intracranial hemorrhage was a prespecified secondary safety outcome in all studies.
Quality Assessment
Risk of bias: The Risk of Bias (RoB) assessment for the studies included in this meta-analysis generally indicated a low risk, with some exceptions (Figure 2). Eikelboom et al. [21] showed low risk across all domains; however, Domain 2 (Deviations from Intended Interventions) was classified as unclear, reflecting uncertainty regarding adherence to the interventions. Halvorsen et al. [22] had low-level risks in most domains, with potential concerns again in Domain 2 related to intervention fidelity. Halperin et al. [23] demonstrated minimal risk of bias in all domains except Domain 2, where the risk was unclear, indicating possible discrepancies in intervention adherence. Kato et al. [25] presented a high risk of bias in Domain 2 due to serious deviations from the described interventions, potentially affecting study validity. Steffel et al. [26] had low risk across all domains, reflecting high-quality study design and conduct. Overall, the included studies exhibited a relatively low risk of bias, though some concerns regarding intervention adherence remain [31].
Risk of bias within the included studies using RoB 2
The RoB assessment, presented in Figure 3, illustrates the methodological quality and risk of bias across the studies included in this meta-analysis. Graham et al. [24] and Lin et al. [29] both exhibited a high risk in Domain 1 (Randomization), indicated by a red X, reflecting potential selection bias due to unclear randomization procedures. This suggests that the randomization process may not have been fully executed, potentially introducing bias in participant selection. Amin et al. [27] showed a high risk in Domain 2 (Deviations from Intended Interventions), indicating that deviations from the planned interventions could have led to performance bias and may have affected the results.
Intra-review bias assessment using the Newcastle-Ottawa Scale
In contrast, Mentias et al. [28] and Yildirim et al. [30] demonstrated low risk of bias in most domains, particularly Domains 3, 4, and 5. This reflects high methodological rigor in outcome measurement, complete reporting of data, and proper selection of results [32].
Publication bias: The funnel plot is largely symmetrical, indicating no substantial publication bias in this meta-analysis (Figure 4). The studies are evenly distributed on either side of the pooled effect size, with larger studies positioned toward the top of the plot and smaller studies toward the bottom. This distribution suggests that smaller studies, which could be overrepresented due to potential publication bias, are not disproportionately influencing the results. The overall shape of the funnel plot indicates that pre-publication bias is unlikely to have dominated the findings.
Funnel plot assessing publication bias among the included studiesCES, combined effect size
This observation is further supported by the Egger regression test (Table 4), which yielded a slope p-value of 0.359, indicating no significant asymmetry in the study distribution. A p-value greater than 0.05 suggests that the slope does not differ significantly from zero, reinforcing the conclusion that publication bias is minimal (Table 5). Additionally, the trim-and-fill analysis indicated that no studies needed to be imputed, confirming that the funnel plot is not skewed. These findings support the conclusion that publication bias likely did not play a significant role in distorting the results of this meta-analysis [33].
Forest Plot
The pooled effects of the included studies on the use of DOACs vs. warfarin in elderly patients with AF are shown in the forest plot (Figure 5). The overall effect size for stroke prevention and major bleeding outcomes with DOACs compared to warfarin is moderate (0.80; 95% CI: 0.40-1.20). The wide CI, spanning from a small to a fairly large positive effect, indicates some uncertainty in the overall outcome.
Forest plot screening the effect sizes from each study, as well as the overall pooled effect size
Individual study results vary. For example, Eikelboom et al. [21] reported an effect size of 0.80, suggesting a moderate reduction in stroke and bleeding risk with DOACs. In contrast, Amin et al. [27] reported a higher effect size of 1.08, indicating a greater benefit in their study population. Lin et al. [29] reported a smaller effect size of 0.23, suggesting less pronounced benefits, particularly among patients with comorbidities or polypharmacy.
These differences reflect variations in patient populations, treatment regimens, and study methods. The contribution of each study to the pooled effect depends on sample size and study quality, highlighting the influence of large, well-designed studies on overall estimates. Despite variability, the findings suggest that DOACs are generally associated with improved outcomes in elderly AF patients, though further research is needed to refine treatment strategies [34,35].
Heterogeneity Assessment
The heterogeneity assessment based on the forest plot (Table 6) reveals substantial variability across the studies included in this meta-analysis. The I² statistic is 94.23%, indicating that most of the variability in effect sizes is attributable to true differences between studies rather than random variation. This high degree of heterogeneity suggests considerable diversity in study design, patient characteristics, interventions, and outcomes [36].
The Q-statistic is 155.91 with a p-value of 0.000, confirming that the observed variability is significant and unlikely due to chance. The T² value of 0.40 further indicates meaningful variation, likely influenced by patient demographics, study designs, treatment regimens, and comorbidities. Although the pooled effect size suggests that DOACs generally have a positive effect on preventing stroke and bleeding compared to warfarin, the high heterogeneity warrants cautious interpretation. Factors such as patient age, comorbidities, and medication adherence may contribute to variability and should be investigated in future studies to refine treatment strategies for elderly AF patients [37,38].
Subgroup Analysis
The subgroup analysis (Figure 6) illustrates differences in treatment effects between two subgroups (AA and BB) of elderly AF patients when comparing DOACs to warfarin. The pooled effect size across subgroups is 0.79 (95% CI: 0.54-1.03), indicating a moderate positive effect of DOACs relative to warfarin, though the wide CI reflects some imprecision. The overall I² value of 94.23% confirms substantial heterogeneity among studies.
Subgroup analysis of the included studies evaluating the outcomes of DOACs vs. warfarin in elderly patients with AF, stratified by patient characteristics, treatment regimen, and study design factorsAF, atrial fibrillation; DOAC, direct oral anticoagulant; LL, lower limit; UL, upper limit
Table 7 provides detailed quantitative data supporting the subgroup analysis, including effect sizes, CIs, measures of heterogeneity (I²), and tests for differences between subgroups. In subgroup AA, the effect size is 0.88 (95% CI: 0.30-1.45), indicating a moderate treatment effect, though the wide CI reflects dispersion in results. The I² value for this subgroup is 88.72%, indicating considerable heterogeneity among studies within the group, which may be attributed to variations in patient demographics, study design, and treatment protocols. In subgroup BB, the effect size is 0.66 (95% CI: -0.55 to -1.36), with an even wider CI that crosses zero, making it difficult to conclude a clear effect in this subgroup. The I² value is 95.81%, higher than in subgroup AA, indicating greater variability [39,40].
Narrative Analysis
DOACs vs. warfarin in stroke prevention and bleeding outcomes: The studies included in this meta-analysis demonstrate an overall beneficial effect of DOACs compared with warfarin in elderly patients with AF, particularly in preventing stroke and major bleeding events. Trials such as those by Eikelboom et al. [21] and Halperin et al. [23] show that DOACs are both safer and more effective, significantly reducing the risks of intracranial hemorrhage and stroke/SE. However, effect sizes vary across studies, with some, such as Mentias et al. [28], indicating a greater benefit of DOACs, while others, like Amin et al. [27], report more modest outcomes.
Impact of patient characteristics on outcomes: The effectiveness of DOACs appears to be influenced by factors such as age, comorbidities, and polypharmacy. More complex outcomes are commonly observed in elderly patients with multiple comorbidities, particularly those taking multiple medications, as reported in Kato et al. [25] and Lin et al. [29]. Amin et al. [27] also noted that polypharmacy in elderly patients may limit the full potential of DOACs in reducing major bleeding and mortality. Careful patient selection and consideration of comorbid conditions are, therefore, critical for optimizing outcomes.
Safety and long-term feasibility: The safety profile of DOACs compared with warfarin is largely favorable. Steffel et al. [26] reported a sixfold reduction in the risk of significant hemorrhages with DOACs, particularly intracranial hemorrhage. While DOACs provide multiple benefits, especially for elderly populations, the long-term feasibility and sustainability of their use in this group require further investigation. There remains limited information on the long-term safety of DOACs in elderly patients with comorbidities, and additional follow-up is needed to better understand their future efficacy and safety.
Variability in outcomes and study findings: Although the overall pooled effect size in this meta-analysis indicates a general benefit of DOACs compared with warfarin, variability among individual study results highlights the influence of study design, patient demographics, and treatment protocols. The high overall heterogeneity (I² = 94.23%) underscores this variability, which may be affected by differences in study design, patient populations, and clinical practices. Inconsistent outcomes reported in studies such as Eikelboom et al. [21] and Kato et al. [25] emphasize the need for standardized treatment regimens to ensure more consistent outcomes across diverse settings and patient populations.
Discussion
The findings of this meta-analysis provide insights into the use of DOACs compared with warfarin in elderly patients with AF. Our results indicate that DOACs offer a moderate benefit by reducing the risk of stroke/SE and major bleeding. However, the high level of heterogeneity observed across studies reflects considerable variability in patient characteristics, clinical settings, and study designs. This heterogeneity limits the generalizability of the results, particularly for older patients with multiple comorbidities [41].
Patient-related factors, such as polypharmacy, age, and comorbidities, appear to be critical in determining treatment outcomes. As evidenced in studies by Amin et al. [27] and Lin et al. [29], the benefits of DOACs are not uniform among elderly patients with complex health profiles. This aligns with previous research indicating that polypharmacy can modify the efficacy and safety of anticoagulation strategies in older adults. Specifically, while DOACs are generally more effective than warfarin in stroke prevention for patients with AF, the presence of multiple comorbidities increases management complexity and the risk of adverse events, including major bleeding [42]. Therefore, careful patient selection is essential to maximize the benefits of DOAC therapy in this population [43].
The results of this meta-analysis also highlight the importance of long-term safety and feasibility, as only a few studies provide extended follow-up. Although short-term outcomes with DOACs are favorable, their long-term effects, particularly in elderly patients, remain inadequately studied. Long-term monitoring is necessary to evaluate potential risks and benefits, especially in frail elderly patients [42]. This gap is reflected in our meta-analysis, which provides limited data on long-term outcomes, such as major gastrointestinal bleeding [44].
Subgroup analyses further illustrate the impact of patient characteristics on treatment outcomes. In Group AA, consisting of healthier patients with fewer comorbidities, DOACs conferred greater benefit. In contrast, Group BB, representing frailer patients, showed more inconsistent outcomes. This heterogeneity underscores the importance of a personalized approach to anticoagulation therapy, as emphasized by Lin et al. [45], who advocated individualizing therapy based on bleeding risk and comorbidities.
Importantly, the publication bias assessment did not indicate significant asymmetry, suggesting that the results of this meta-analysis are unlikely to be influenced by selective reporting. This aligns with findings from Oertel and Fogerty [14], who also observed minimal publication bias in studies comparing DOACs with warfarin. The RoB assessment revealed that most included studies had low or unclear risk, although some studies, such as Graham et al. [24] and Kato et al. [25], exhibited potential risks related to randomization and intervention fidelity, indicating some instability in their findings.
Limitations
This meta-analysis has several limitations that should be considered when interpreting the results. First, high heterogeneity (I² = 94.23%) among the included studies is a major drawback. Differences in effect size across studies may be explained by variations in patient populations, study characteristics, and treatment methodologies. This heterogeneity makes it difficult to draw conclusive statements about the relative efficacy of DOACs compared with warfarin, largely due to the variability in patient populations.
Another limitation is the insufficient long-term data on the safety and efficacy of DOACs in aging populations, which is important for estimating the sustainability of the observed positive treatment effects. Although the current research provides promising short-term evidence, the lack of comprehensive long-term follow-up data prevents a detailed assessment of long-term risks, including major bleeding and other adverse events.
Additionally, not all studies included in the meta-analysis had a low risk of bias. Some exhibited moderate to high risk in areas such as randomization and adherence to interventions, which may affect the internal validity of the results. While publication bias was found to be nonsignificant, relying solely on published articles may underrepresent studies with nonsignificant or negative results, potentially compromising the overall conclusions. Finally, inconsistency in study methodologies, such as differences in outcome measures and data recording, represents another source of difficulty in interpreting the findings.
Future Research
Future studies should address the limitations highlighted in this meta-analysis and aim to further refine our understanding of the efficacy and safety of DOACs compared with warfarin in elderly patients with AF. A key area for further research is the long-term safety of DOACs, particularly in geriatric patients with multiple comorbidities. Longitudinal studies with extended follow-up are needed to assess the sustainability of treatment benefits and to determine potential long-term risks, including major bleeding and adverse cardiovascular events, which are not adequately addressed in the current literature.
It is also important to standardize patient selection criteria and treatment protocols to reduce variability across studies included in future meta-analyses. Additionally, research should focus on identifying predictive factors that influence treatment outcomes, such as age, polypharmacy, comorbid conditions, and genetic factors, which could help personalize anticoagulant therapy for elderly patients with AF.
Further RCTs are needed, particularly across diverse patient populations, to minimize biases inherent in observational studies. Consistent methodologies across studies will facilitate comparisons and allow for more confident conclusions. Finally, evidence from real-world usage of DOACs, drawn from large cohort studies and registry data, can provide insights into how these medications perform in clinical practice, where patient characteristics and adherence may differ from controlled trial settings.
Conclusions
This systematic review and meta-analysis provide important insights into the efficacy and safety of DOACs compared with warfarin in the elderly population with AF. Pooled analysis of the study results shows an effect size of 0.80 (95% CI: 0.54-1.03), indicating that DOACs have a moderate effect in reducing stroke/SE and major bleeding compared with warfarin. Although positive effects were observed, these findings are substantially limited by high heterogeneity, which arises from differences in patient demographics, study design, and clinical management. These factors must be considered when interpreting the results. Subgroup analyses further highlight that treatment outcomes vary depending on factors such as age, comorbidities, and polypharmacy. DOACs performed better in some subgroups but were less effective in others, particularly among patients with more complex health profiles. This underscores the need for individualized treatment approaches that account for patient-specific characteristics. Despite generally favorable outcomes, several limitations, including the lack of long-term data and potential biases in the included studies, emphasize the need for further research. Future studies should focus on long-term follow-up, standardization of methodologies, and evaluation of real-world use to better determine the long-term efficacy, safety, and generalizability of DOACs in the elderly population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Atrial fibrillation: the current epidemic J Geriatr Cardiol Morillo CA Banerjee A Perel P Wood D Jouven X 195203142017 https://pubmed.ncbi.nlm.nih.gov/28592963/2859296310.11909/j.issn.1671-5411.2017.03.011PMC 5460066 · doi ↗ · pubmed ↗
- 2Epidemiology of atrial fibrillation Int J Clin Pract Zulkifly H Lip GY Lane DA 072201810.1111/ijcp.1307029493854 · doi ↗ · pubmed ↗
- 3Atrial fibrillation in older people: concepts and controversies Front Med (Lausanne) Zathar Z Karunatilleke A Fawzy AM Lip GY 175620193144050810.3389/fmed.2019.00175 PMC 6694766 · doi ↗ · pubmed ↗
- 4Atrial fibrillation in the elderly population: challenges and management considerations J Arrhythm Salih M Abdel-Hafez O Ibrahim R Nair R 9129213720213438611710.1002/joa 3.12580 PMC 8339095 · doi ↗ · pubmed ↗
- 5Clinical effectiveness of direct oral anticoagulants vs warfarin in older patients with atrial fibrillation and ischemic stroke: findings from the Patient-Centered Research Into Outcomes Stroke Patients Prefer and Effectiveness Research (PROSPER) study JAMA Neurol Xian Y Xu H O'Brien EC 119212027620193132921210.1001/jamaneurol.2019.2099 PMC 6647003 · doi ↗ · pubmed ↗
- 6New oral anticoagulants: their advantages and disadvantages compared with vitamin K antagonists in the prevention and treatment of patients with thromboembolic events Ther Clin Risk Manag Mekaj YH Mekaj AY Duci SB Miftari EI 967977112015 https://doi.org/10.2147/TCRM.S 842102615072310.2147/TCRM.S 84210 PMC 4485791 · doi ↗ · pubmed ↗
- 7Antithrombotic treatment for secondary prevention of stroke and other thromboembolic events in patients with stroke or transient ischemic attack and non-valvular atrial fibrillation: a European Stroke Organisation guideline Eur Stroke J Klijn CJ Paciaroni M Berge E 198223420193198422810.1177/2396987319841187 PMC 6960695 · doi ↗ · pubmed ↗
- 8Managing atrial fibrillation in the very elderly patient: challenges and solutions Vasc Health Risk Manag Karamichalakis N Letsas KP Vlachos K Georgopoulos S Bakalakos A Efremidis M Sideris A 5555621120152660477210.2147/VHRM.S 83664 PMC 4630199 · doi ↗ · pubmed ↗