Two Years, Many Clues: Diagnostic Journey and Treatment of Chronic Neurobrucellosis in an Elderly Woman
Pedro Vasques, Daniel Araújo, Andreia Paulos, Maria Lima, Ana Catarina Gonçalves, Evelise Ramos, João Pedro Caria, Andre Militão, Maria Isabel Casella

TL;DR
A 61-year-old woman with chronic neurological symptoms was eventually diagnosed with neurobrucellosis after a two-year journey, highlighting the disease's diagnostic challenges.
Contribution
The paper presents a rare case of chronic neurobrucellosis diagnosed after prolonged misdiagnosis and emphasizes the importance of considering this condition in unexplained neurological cases.
Findings
Chronic neurobrucellosis was confirmed after isolating Brucella melitensis from cerebrospinal fluid.
Neurological symptoms persisted for two years with initial misdiagnosis as CNS vasculitis.
Targeted antibiotic treatment led to significant clinical improvement in the patient.
Abstract
Neurobrucellosis is a rare complication of brucellosis, a zoonotic infection caused by Brucella spp. Its varied neurological manifestations make diagnosis difficult, often resulting in delays and increased morbidity. We present the case of a 61-year-old woman with recurrent neurological symptoms over two years, including confusion, gait imbalance, and cognitive decline. Despite extensive investigations showing ischemic changes on brain imaging, intrathecal IgG synthesis, and persistent cerebrospinal fluid (CSF) lymphocytic pleocytosis with initially sterile cultures, a presumptive diagnosis of primary central nervous system (CNS) vasculitis was made. After several hospital admissions and empirical treatments, Brucella melitensis was eventually isolated from the CSF, confirming chronic neurobrucellosis. Targeted antibiotic therapy led to significant clinical improvement. This case…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
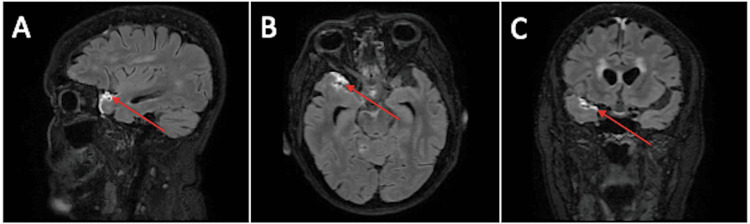 Figure 1
Figure 1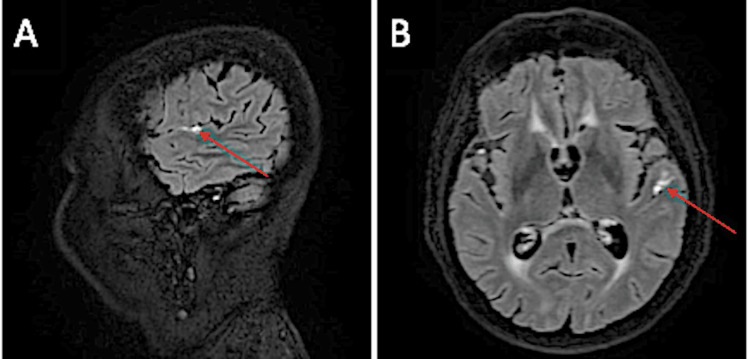 Figure 2
Figure 2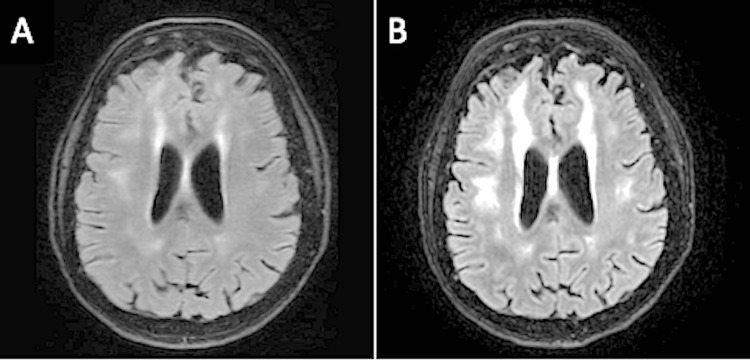 Figure 3
Figure 3| Laboratory finding | Value | Reference range |
| Hemoglobin | 11 g/dL | 11.5-15 g/dL |
| Leukocyte count | 13.400/μL | 4.500-11.400/μL |
| C-Reactive protein | 23.8 mg/dL | <0.5 mg/dL |
| Erythrocyte sedimentation rate | 72 mm/h | 1-20 mm/h |
| Urinalysis | 250 leukocytes/HPF | <25 /HPF |
| Parameter | Value | Reference range |
| Hemoglobin | 11 g/dL | 11.5-15 g/dL |
| Erythrocyte sedimentation rate | 47 mm/h | 1-20 mm/h |
| Ferritin | 846 ng/mL | 30-200 ng/mL |
| Anti-ds-DNA | <0.5 UI/mL | <10 UI/mL |
| ENA antibodies | Negative | - |
| Anti-HIV-1/2 antibodies + Ag p24 | Negative | - |
| Ag HBs | Negative | - |
| Anti-HCV antibodies | Negative | - |
| Total antibodies (IgM + IgG) for syphilis | Negative | - |
| Parameter | Value | Reference range |
| CSF cell count | 55 leukocytes/μL (80% lymphocytes) | <5 leukocytes/μL |
| Proteinorrhachia | 206 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 56 mg/dL | 40-70 mg/dL |
| Glycemia | 111 mg/dL | 80-115 mg/dL |
| CSF multiplex PCR | Negative | - |
| Parameter | Value | Reference range |
| CSF cell count | 70 leukocytes/μL (65% lymphocytes) | <5 leukocytes/μL |
| Proteinorrhachia | 157 mg/dL | 15-40 mg/dL |
| ADA | 13 U/L | <9 U/L |
| Glycorrhachia | 49 mg/dL | 40-70 mg/dL |
| Glycemia | 120 mg/dL | 80-115 mg/dL |
| CSF multiplex PCR | Negative | - |
|
| Negative | - |
|
| Negative | - |
| Bacterial culture | Sterile | - |
| Mycobacterial culture | Sterile | - |
| Anatomopathological exam | Unspecific lymphoplasmacytic infiltrate | - |
| Parameter | Value | Reference range |
| Immunoglobulin G | 1140 mg/dL | 700-1600 mg/dL |
| Immunoglobulin A | 353 mg/dL | 70-400 mg/dL |
| Immunoglobulin M | 59.7 mg/dL | 40-230 mg/dL |
| Kappa light chains | 294 mg/dL | 170-370 mg/dL |
| Lambda light chains | 177 mg/dL | 90-210 mg/dL |
| Peripheral blood immunophenotyping | Unremarkable | - |
|
| Negative | - |
|
| Negative | - |
| Parameter | Value | Reference range |
| CSF cell count | 60 leukocytes/μL (75% lymphocytes) | <5 leukocytes/μL |
| Proteinorrhachia | 183 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 45 mg/dL | 40-70 mg/dL |
| Glycemia | 132 mg/dL | 80-115 mg/dL |
| CSF multiplex PCR | Negative | - |
|
| Negative | - |
| Bacterial culture | Sterile | - |
| Parameter | Value | Reference range |
| CSF cell count | 50 leukocytes/μL (75% lymphocytes) | <5 leukocytes/μL |
| Proteinorrhachia | 209 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 45 mg/dL | 40-70 mg/dL |
| Glycemia | 132 mg/dL | 80-115 mg/dL |
| Bacterial culture | Sterile | - |
| Mycobacterial culture | Sterile | - |
| Anatomopathologic exam | No signs of malignancy | - |
| Flow cytometry | CD4 predominance, no monoclonality | - |
| Oligoclonal bands | Intrathecal IgG synthesis | - |
| Antineuronal antibody panel | Negative | - |
| Parameter | Value | Reference range |
| CSF cell count | <5 leukocytes/μL (100% lymphocytes) | <5 leukocytes/μL |
| Proteinorrhachia | 162 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 62 mg/dL | 40-70 mg/dL |
| Glycemia | 147 mg/dL | 80-115 mg/dL |
| Bacterial culture | Sterile | - |
| Mycobacterial culture | Sterile | - |
| Mycological culture | Sterile | - |
| Parameter | Value | Reference range |
| Huddleson reaction | Negative | - |
| CMV - IgM | Negative | <0.7 UI/mL (negative); >0.9 UI/mL (positive) |
| CMV - IgG | 82 UI/mL | <4 UI/mL (negative); >6 UI/mL (positive) |
| EBV - CA IgM | <10 UI/mL | <20 UI/mL (negative); >40 UI/mL (positive) |
| EBV - CA IgG | 302 UI/mL | <20 UI/mL (negative); >20 UI/mL (positive) |
| EBNA - IgG | 57 UI/mL | <5 UI/mL (negative); >20 UI/mL (positive) |
|
| <0.1 Ua/mL | <10 Ua/mL (negative); >10 Ua/mL (positive) |
|
| <0.1 Ua/mL | <10 Ua/mL (negative); >10 Ua/mL (positive) |
|
| Negative | <0.55 UI/mL (negative); >0.65 UI/mL (positive) |
|
| Negative | <4 UI/mL (negative); >8 UI/mL (positive) |
| CSF - arboviruses IgM | Negative | - |
| CSF - arboviruses IgG | Negative | - |
| ANA | Negative | - |
| ENA | Negative | - |
| Anti-ds-DNA | <0.5 UI/mL | <10 UI/mL (negative); >15 UI/mL (positive) |
| Anti-cardiolipin - IgM | 3.4 UI/mL | <10 UI/mL (negative); >40 UI/mL (positive) |
| Anti-cardiolipin - IgG | <0.5 UI/mL | <10 UI/mL (negative); >40 UI/mL (positive) |
| Lupus anticoagulant | Not observed | - |
| Anti-glycoprotein I antibodies - IgM | <2.9 UI/mL | <7 UI/mL (negative); >10 UI/mL (positive) |
| Anti-glycoprotein I antibodies - IgG | <0.6 UI/mL | <7 UI/mL (negative); >10 UI/mL (positive) |
| Anti-PR3 | <0.2 UI/mL | <2 UI/mL (negative); >3 UI/mL (positive) |
| Anti-MPO | <0.2 UI/mL | <2 UI/mL (negative); >5 UI/mL (positive) |
| Parameter | Value | Reference range |
| CSF cell count | 115 leukocytes/μL (70% lymphocytes) | <5 leukocytes/μL |
| Proteinorrhachia | 313 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 64 mg/dL | 40-70 mg/dL |
| Glycemia | 100 mg/dL | 80-115 mg/dL |
| Bacterial culture | Sterile | - |
| Flow cytometry | CD4 lymphocyte predominance, no monoclonality | - |
| Parameter | Value | Reference range |
| CSF cell count | 85 leukocytes/μL (70% lymphocytes) | <5 leukocytes/μL |
| Proteinorrhachia | 217 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 57 mg/dL | 40-70 mg/dL |
| Glycemia | 81 mg/dL | 80-115 mg/dL |
| Bacterial culture | Sterile | - |
| Parameter | Value | Reference range |
| CSF cell count | 28 leukocytes/μL (100% lymphocytes) | <5 leukocytes/μL |
| Proteinorrhachia | 80 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 65 mg/dL | 40-70 mg/dL |
| Glycemia | 87 mg/dL | 80-115 mg/dL |
| Bacterial culture | Brucella melitensis | - |
| Parameter | Value | Reference range |
| Rose Bengal test | Positive | - |
| Brucella - IgA (blood) | Positive | - |
| Brucella - IgG (blood) | Positive | |
| Brucella - IgA (CSF) | Positive | - |
| Brucella - IgG (CSF) | Positive | - |
| Immunocapture test | 1:2560 | - |
| Parameter | Value | Reference range |
| Huddleson reaction | Positive | - |
| Immunocapture test | 1:5120 | - |
| Erythrocyte sedimentation rate | 20 mm/h | 1-20 mm/h |
| Parameter | Value | Reference range |
| CSF cell count | 20 leukocytes/μL (no cell predominance) | <5 leukocytes/μL |
| Proteinorrhachia | 67 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 51 mg/dL | 40-70 mg/dL |
| Glycemia | 147 mg/dL | 80-115 mg/dL |
| Bacterial culture | Sterile | - |
| Brucella IgM | Negative | - |
| Brucella IgA | Positive | |
| Brucella IgG | Positive | |
| Brucella DNA PCR | Positive | - |
| Parameter | Value | Reference range |
| CSF cell count | 8 leukocytes/μL (no cell predominance) | <5 leukocytes/μL |
| Proteinorrhachia | 77 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 41 mg/dL | 40-70 mg/dL |
| Glycemia | 115 mg/dL | 80-115 mg/dL |
| Bacterial culture | Sterile | - |
| Brucella DNA PCR (CSF) | Positive | - |
| Huddleson reaction | Positive | - |
| Immunocapture test | 1:5120 | - |
| Parameter | Value | Reference range |
| CSF cell count | <5 leukocytes/μL | <5 leukocytes/μL |
| Proteinorrhachia | 59 mg/dL | 15-40 mg/dL |
| Glycorrhachia | 51 mg/dL | 40-70 mg/dL |
| Glycemia | Unknown | 80-115 mg/dL |
| Bacterial culture | Sterile | - |
| Brucella DNA PCR (CSF) | Negative | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrucella: diagnosis, epidemiology, treatment · Burkholderia infections and melioidosis · Bartonella species infections research
Introduction
Brucellosis has a worldwide distribution, with up to 500,000 cases diagnosed annually [1,2], and is endemic in the Mediterranean Basin, the Middle East, Central and South America, parts of sub-Saharan Africa, and South and Central Asia [3]. The bacteria primarily infect livestock and wildlife, while humans are incidental hosts who typically acquire the infection through contact with animal tissues or secretions, consumption of unpasteurized animal products, or inhalation of aerosols [3]. Of the dozen known Brucella species, four account for most human infections [3]: Brucella melitensis (from sheep/goats and the most virulent in humans), Brucella abortus (cattle), Brucella suis (swine), and Brucella canis (dogs). After entering the host, these organisms predominantly affect the reticuloendothelial system and use multiple mechanisms to evade immune detection.
Neurobrucellosis, estimated to occur in 4%-5% of brucellosis cases [1,2], is usually acquired through hematogenous spread [4]. Its underlying immunopathology involves meningeal granulomatosis and vasculitis, giving rise to a broad range of possible clinical presentations, including meningoencephalitis, transverse myelitis, peripheral neuropathy, and space-occupying lesion syndromes [2], often with a protracted course. Laboratory diagnosis relies on prolonged culture of this fastidious organism in blood, CSF, or tissue biopsy samples, along with serological evidence of infection [4,5].
There is no consensus on the optimal treatment for neurobrucellosis, but successful regimens typically involve prolonged combination antibiotic therapy with agents that have good central nervous system (CNS) penetration, such as ceftriaxone, rifampicin, cotrimoxazole, and doxycycline [6,7]. Sequelae are common due to delays in diagnosis and treatment. These vary depending on the clinical presentation and the CNS structures involved, but most often include motor deficits and sensorineural hearing or visual impairment [4,8].
Case presentation
We present the case of a 61-year-old woman with a medical history of breast cancer treated with surgery, chemotherapy, and radiotherapy in 2006, with discharge from oncology follow-up in 2014; poorly controlled hypertension; chronic primary headaches for several decades treated with triptans and NSAIDs; and anxiety managed with benzodiazepines.
To better understand the case, a chronological summary of the most relevant emergency room (ER) visits and hospital admissions is presented below.
2021-2022
The patient, who was fully autonomous and living alone in Setúbal, had no known history of contact with livestock or consumption of unpasteurized dairy products. She first presented to the ER in June 2021 with a two-month history of headache, tinnitus, and malaise, along with episodes of fainting, gait imbalance, periods of confusion and incoherent speech, and, according to relatives, an unintentional 9 kg weight loss (approximately 10% of her body weight). Physical examination on admission was largely unremarkable except for mild confusion. There were no focal neurological deficits, including no changes in speech, coordination, or gait. Vital signs were mostly normal, except for mild tachycardia (105 bpm); the patient was normotensive, afebrile, and had a peripheral oxygen saturation of 98% on room air. Laboratory findings are summarized in Table 1.
Besides the laboratory results, a brain computed tomography (CT) scan showed a previous left cerebellar infarction, with no acute findings. She was admitted to the Infectious Diseases (ID) Department, where empirical ceftriaxone was started for a presumed urinary tract infection (UTI). This led to improvement in her neurocognitive symptoms and normalization of inflammatory markers after completing treatment. A whole-body CT scan excluded malignancy but revealed multiple enlarged right cervical lymph nodes considered pathologic based on number, size, and enhancement. Neurology recommended an electroencephalogram (EEG) and brain magnetic resonance imaging (MRI). The EEG showed no abnormalities, and the MRI, which was performed after hospital discharge, demonstrated ischemic changes in both cerebellar hemispheres (previously seen only on the left in the CT scan) and in the periventricular white matter.
Over the following two months, laboratory investigations showed persistent anemia (Hb 11 g/dL) and slightly elevated erythrocyte sedimentation rate (ESR; 47 mm/h) and ferritin (846 ng/mL), with negative infectious serologies (human immunodeficiency virus (HIV), hepatitis C virus (HCV), hepatitis B virus (HBV), Venereal Disease Research Laboratory (VDRL)) and negative autoimmunity markers (anti-dsDNA and ENA antibodies) (Table 2).
A cervical CT scan was performed to further assess the noted lymphadenopathy and revealed Waldeyer’s ring hypertrophy. Biopsy of this area ruled out malignancy. Given her weight loss and persistent anemia, the patient underwent upper endoscopy, which showed mild gastritis with Helicobacter pylori infection, and a total colonoscopy, which was unremarkable. As part of the stroke workup, transthoracic echocardiography (TTE) and Holter monitoring were also conducted, with no significant abnormalities detected.
The patient was referred for Neurology outpatient follow-up and, over the next several months, underwent additional diagnostic testing. Transcranial Doppler and neck vessel ultrasound scans were unremarkable. A transesophageal echocardiogram (TEE) revealed a patent foramen ovale (PFO) with bidirectional shunting. A positron emission tomography (PET) scan showed increased metabolic activity in the nasopharynx, although malignancy had already been excluded on biopsy. A repeat brain and spinal cord MRI, performed eight months after the initial study, showed no new abnormalities. She was then referred for PFO closure, pending exclusion of chronic pulmonary embolism (PE) through a thoracic angio-CT scan.
During this period, the patient continued to experience headaches, dizziness, and gait imbalance, leading to four additional ER visits. In her final visit, in October 2022, she was found at home lying on the floor, with incoherent speech and urinary incontinence. On arrival to the ER, she had a temperature of 38 °C and reported memory difficulties and bilateral hand paraesthesias. A lumbar puncture (LP) was performed, and the cerebrospinal fluid (CSF) findings are shown in Table 3.
During her stay in the ER, suprapubic tenderness was noted on physical examination, and her urine appeared cloudy. This prompted initiation of empirical ceftriaxone for a presumed UTI, along with concurrent aseptic meningitis.
She was admitted to the ID Department for continued evaluation. Urine culture later grew Enterococcus faecium, and antimicrobial therapy was adjusted to a seven-day course of linezolid after she developed an erythematous infusion reaction compatible with Red Man Syndrome during vancomycin administration. During this admission, and to further broaden the diagnostic workup, a repeat lumbar puncture was performed (Table 4), along with additional blood tests, including Borrelia spp. serology and peripheral blood immunoglobulin levels with immunophenotyping (Table 5).
Repeat EEG remained normal. Angio-CT of the thorax was performed and could not definitively rule out PE, which was subsequently achieved by ventilation-perfusion scintigraphy.
2023
In January 2023, she continued to exhibit mild cognitive impairment, mainly characterized by executive dysfunction. An EEG performed in the outpatient setting revealed mild epileptiform activity for the first time, and the patient was started on levetiracetam.
In April, she returned to the ER with fever, headache, confusion, nausea, and vomiting; hence, another LP was performed (Table 6).
She was readmitted for further evaluation, again with a working diagnosis of aseptic meningitis. During this stay, she continued to exhibit mild confusion and intermittent, self-limited fever without an identifiable infectious source. Blood and urine cultures remained negative. Following the Neurology consultation, additional investigations were performed, including another EEG, repeat brain MRI, and a new LP with expanded testing as recommended (Table 7). These studies showed findings similar to previous evaluations, notably persistent lymphocytic pleocytosis and, importantly, evidence of intrathecal IgG synthesis on oligoclonal band testing. This latter result represented a key milestone in the diagnostic process.
She was discharged after showing clinical improvement but was readmitted to the ID Department shortly thereafter with fever, vomiting, confusion, dysarthria, and quadriparesis (MRC 3/5-4/5). The LP findings during this admission showed slight differences compared to prior evaluations (Table 8), and an extensive panel of additional tests was performed to further broaden the diagnostic workup (Table 9).
Later in her stay, Escherichia* coli* was isolated from a urine culture obtained during a recurrence of fever, and she completed a one-week course of cefuroxime based on susceptibility testing. Although the fever resolved, her fluctuating neurological deficits persisted. Given the previously documented intrathecal IgG synthesis, the case was again discussed with Neurology. At this stage, primary CNS vasculitis became the leading diagnostic hypothesis, and the patient was transferred to the Neurology ward in June.
Brain angio-MRI demonstrated leptomeningitis and mural enhancement involving the inferior division of the right middle cerebral artery (MCA) (Figure 1) and the superior temporal branch of the inferior division of the left MCA (Figure 2). Digital subtraction angiography, performed at another hospital, showed a “string-of-beads” appearance in the M3 segment of the right MCA, findings supportive of vasculitis. A repeat LP revealed persistent hyperproteinorrachia and lymphocytic pleocytosis, and CSF flow cytometry remained unremarkable (Table 10).
(A) Sagittal, (B) axial, and (C) coronal gadolinium-enhanced FLAIR images (June 2023)Enhancement of the anterior aspect of the right Sylvian fissure is visible (red arrows), supplied by the homolateral MCA inferior division.FLAIR: fluid-attenuated inversion recovery, MCA: middle cerebral artery.
(A) Sagittal and (B) axial gadolinium-enhanced FLAIR images (June 2023) Enhancement of the posterior aspect of the left Sylvian fissure (red arrows), supplied by the superior temporal division of the left MCA inferior branch.FLAIR: fluid-attenuated inversion recovery, MCA: middle cerebral artery.
It is also worth noting that she developed an episode of acute urinary retention in the context of yet another E. coli UTI, accompanied by mild bilateral hydronephrosis on ultrasound. Directed cotrimoxazole therapy and urinary catheterization, with successful removal after five days, promptly resolved this complication.
Suspected primary CNS vasculitis prompted high-dose corticosteroid therapy (methylprednisolone pulses followed by an oral prednisolone taper). However, her condition deteriorated, with worsening confusion and psychomotor slowing. During this period, EEG documented a non-convulsive status epilepticus, which resolved after lacosamide was added to her ongoing levetiracetam regimen. Cyclophosphamide was then initiated, and she completed three monthly cycles between August and October.
Neurological deficits persisted during this time, including fluctuating quadriparesis, gait ataxia, and intermittent episodes of encephalopathy. MRI performed at the end of the first cyclophosphamide cycle (August) showed worsening T2 hyperintensities and juxtacortical frontoparietal white-matter lesions, consistent with microvascular ischemic changes. She also received a second methylprednisolone pulse during the second cyclophosphamide cycle in September. A repeat MRI following this second cycle demonstrated findings similar to the previous study (Figure 3). Two additional LPs, performed at the end of the second and third cycles, respectively, continued to show persistent lymphocytic pleocytosis and elevated CSF protein levels (Tables 11, 12).
Axial FLAIR images from (A) June 2023 and (B) September 2023Poorly defined areas of subcortical and periventricular hyperintensities mainly located in the frontoparietal white matter are visible, with significant worsening between the two exams.FLAIR: fluid-attenuated inversion recovery.
In the final lumbar puncture, B. melitensis was isolated from the CSF culture and subsequently confirmed by serology (Table 13).
The diagnosis of chronic neurobrucellosis was established, and targeted antibiotic therapy was initiated, consisting of intravenous (IV) ceftriaxone 2 g every 12 hours for six weeks, oral rifampicin 600 mg daily, and oral doxycycline 100 mg twice daily for at least 12 weeks.
In November, the patient developed right leg swelling and pain, and deep venous thrombosis (DVT) of the right lower limb was confirmed by angio-CT scan. Anticoagulation with enoxaparin was started, resulting in significant clinical improvement.
After six weeks of IV antibiotics, she showed marked improvement, regaining full orientation, sustained attention, and fluent, coherent speech. Postural control and motor coordination also improved, allowing her to stand without assistance, though only for brief periods. She was discharged to a convalescent care unit for motor rehabilitation to regain functional autonomy. Follow-up appointments were scheduled with both Neurology and ID, although the latter was subsequently missed. Outpatient medications included rifampicin 600 mg daily and doxycycline 100 mg twice daily for neurobrucellosis; prednisolone 2.5 mg daily and cotrimoxazole 800/160 mg three times per week for corticosteroid taper and chemoprophylaxis; rivaroxaban 20 mg daily for right lower limb DVT; amitriptyline 10 mg for chronic headache; levetiracetam 1500 mg twice daily; and risperidone 1 mg plus trazodone 150 mg at night to manage agitation, particularly in the context of corticosteroid therapy. She was also advised to monitor for dysuria, suprapubic pain, or decreased urine flow, given her history of recurrent UTIs and a prior episode of urinary retention.
2024
Upon reassessment in a Neurology appointment in February, the patient had no deficits apart from a grade 4/5 proximal paresis with flexion of the right thigh, mild right-predominant dysmetria on finger-to-nose test (sequelae of previous cerebellar strokes), and a slight gait imbalance, with ambulation only possible with unilateral support from a caregiver. By this time, the patient was on her 16th week of treatment with rifampicin and doxycycline, and repeat serologic tests and LP were planned to monitor treatment response.
Accordingly, blood tests were repeated in April (Table 14), followed by another LP in May (Table 15).
Due to persistent pleocytosis despite clinical improvement, presumed therapeutic failure was considered, and the patient was readmitted to the Neurology Department in August for a second six-week course of ceftriaxone. The case was reviewed again with ID, who recommended continuing rifampicin and doxycycline without a defined treatment duration. A LP performed during this admission showed significant improvement, as did the repeat serologic tests (Table 16).
Table 16: Repeat LP and blood serologic tests after new course of IV ceftriaxone (August 2024; 42 weeks of treatment): significant improvement as seen by reduction in cell countCSF: cerebrospinal fluid, LP: lumbar puncture. Note: CSF Brucella DNA PCR and immunocapture test were performed outside the hospital.
2025
Clinically, the patient remained stationary, with some gait imbalance still requiring support. New LP in January finally showed no pleocytosis, although still with mildly elevated protein levels (Table 17).
Table 17: Repeat LP (January 2025; 64 weeks of treatment): no pleocytosis observed after prolonged therapyCSF: cerebrospinal fluid, PCR: polymerase chain reaction, LP: lumbar puncture. Note: CSF Brucella DNA PCR was performed outside the hospital.
She is scheduled for clinical evaluations every three months, with a repeat lumbar puncture planned in one year if she remains clinically stable. Having been considered cured, rifampicin and doxycycline were discontinued in May 2025, after 80 weeks of treatment. No treatment-related side effects were reported by the patient during this period.
Discussion
The patient’s long-standing, nonspecific neurological symptoms, sequelae of prior infarctions on CT and MRI, and history of weight loss prompted an extensive investigation. Unremarkable stroke workup, exclusion of cancer relapse, lymphoproliferative disorders, autoimmune disease, and multiple infectious etiologies initially left a diagnostic dead end, with repeated UTI diagnoses and later episodes of concurrent aseptic meningitis. In hindsight, the multiple courses of ceftriaxone for presumed UTI likely contributed to intermittent symptom improvement and relapse, resulting in numerous ER visits and hospital admissions and further delaying the diagnosis of neurobrucellosis. It is also likely that the Huddleson reaction performed a few months before Brucella isolation was a false negative, either due to a prozone effect or because the test detects only agglutinating antibodies. In chronic, long-standing forms of the disease, non-agglutinating antibodies tend to predominate [9-11]. Persistent lymphocytic pleocytosis across multiple LPs was the key finding that eventually guided the diagnosis, after repeated microbiological, anatomopathologic, serological, and molecular CSF exams showed nothing except intrathecal IgG synthesis. This finding initially suggested primary CNS vasculitis, a hypothesis further supported by DSA findings. After clinical and radiological worsening under immunosuppressive therapy, initially appearing paradoxical, B. melitensis was unexpectedly isolated from a CSF culture (after multiple prior LPs). Serological studies subsequently corroborated this result, which, despite initial skepticism, is definitive: CSF culture is a gold standard for neurobrucellosis diagnosis, albeit with a sensitivity of only 35%-45% and high variability across studies [8,12]. Positive Rose Bengal testing, along with immunocapture and ELISA for IgG and IgA in both blood and CSF, provided strong support for the diagnosis, which is essentially one of exclusion. CSF serology is highly specific for neurobrucellosis, and both ELISA and immunocapture assays are less prone to prozone effects, allowing detection of non-agglutinating antibodies [13-15].
Recommended treatment involves a prolonged combination of antibiotics, typically four to six weeks of IV ceftriaxone followed by doxycycline plus rifampicin for at least 12 weeks, sometimes extending to 24 weeks. Prolonged combination therapy is essential to prevent relapse, although supporting evidence remains limited [6,16].
Monitoring response to therapy generally involves repeated clinical assessment, serology, and CSF evaluation, with expected resolution of neurological symptoms and CSF lymphocytic pleocytosis [7,17]. Interestingly, a subsequent positive Huddleson reaction supported the hypothesis of a prior false-negative result due to a prozone effect, even though the test has no role in monitoring treatment response. No standardized serological criteria exist for defining eradication, treatment failure, relapse, or evolution to focal disease, as antibody levels vary widely across patients [18]. A twofold rise in immunocapture antibody titers is inconclusive, and the lack of standardization in many assays, including in-house tests, further complicates interpretation. In endemic areas or among patients with occupational exposure, higher antibody levels are expected in contacts, past infections, and treated individuals compared with patients from non-endemic areas or without occupational risk [19,20], underscoring the central role of clinical assessment and CSF analysis in monitoring treatment response.
Conclusions
This case highlights the importance of considering neurobrucellosis in the differential diagnosis of unexplained neurological syndromes, even when it remains a diagnosis of exclusion. Early recognition and targeted therapy are essential to reduce mortality and prevent irreversible neurological damage. The potential for relapse during follow-up, combined with the typically prolonged and sometimes indefinite treatment duration, also underscores the inherent limitations of case reports involving this disease, as the clinical course may not be fully concluded. Because most of what is known about neurobrucellosis comes from case reports and small retrospective studies, the absence of standardized diagnostic criteria, established treatment regimens, and clear monitoring protocols becomes more understandable, a reflection of the elusive nature of this condition. We hope this case adds a meaningful contribution to the existing literature, given the extensive two-year investigation preceding Brucella isolation in a CSF culture sample, despite an earlier false-negative serology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Uncommon presentation of neurobrucellosis Neurosciences (Riyadh) Ibrahim II Aqeeli MO Aljabri MR Tajuddin AK 2412463020254067007510.17712/nsj.2025.3.20240081 PMC 12279334 · doi ↗ · pubmed ↗
- 2Neurobrucellosis Curr Opin Infect Dis Soares CN da Silva MT Lima MA 1921973620233709304310.1097/QCO.0000000000000920 · doi ↗ · pubmed ↗
- 3Brucellosis in India - a review J Biosci Mantur BG Amarnath SK 5395473320081920897910.1007/s 12038-008-0072-1 · doi ↗ · pubmed ↗
- 4Neurobrucellosis: a retrospective cohort of 106 patients Trop Med Health Arazi F Haddad M Sheybani F Farzadfard MT Rezaeian MK 95320253981537110.1186/s 41182-025-00680-1PMC 11737133 · doi ↗ · pubmed ↗
- 5Brucellosis: epidemiology, pathogenesis, diagnosis and treatment-a comprehensive review Ann Med Qureshi KA Parvez A Fahmy NA 22953985520233816591910.1080/07853890.2023.2295398 PMC 10769134 · doi ↗ · pubmed ↗
- 6Updated therapeutic options for human brucellosis: a systematic review and network meta-analysis of randomized controlled trials P Lo S Negl Trop Dis Huang S Xu J Wang H 018202410.1371/journal.pntd.0012405 PMC 1134089039172763 · doi ↗ · pubmed ↗
- 7Neurobrucellosis: laboratory features, clinical characteristics, antibiotic treatment, and clinical outcomes of 21 patients BMC Infect Dis Zhuang W He T Tuerheng J 4852420243873032710.1186/s 12879-024-09308-x PMC 11088156 · doi ↗ · pubmed ↗
- 8Brucellosis J Neurol Sci Shakir R 11728042020213335819210.1016/j.jns.2020.117280 · doi ↗ · pubmed ↗