Comprehensive characterisation of individuals with fibrotic interstitial lung disease: baseline insights from the INJUSTIS study
Fasihul Khan, Iain Stewart, Lucy Howard, Christopher Michael Barber, Rebecca Borton, Rebecca Braybrooke, Glenn Hearson, Steve Jones, Toby Maher, Laura Matthews, Gauri Saini, Norma Thompson, Andrew M Wilson, Simon R Johnson, Gisli Jenkins

TL;DR
This study characterizes individuals with fibrotic lung diseases, finding similarities in lung function and quality of life despite different causes.
Contribution
The study identifies baseline similarities across fibrotic ILD subtypes, suggesting shared disease mechanisms.
Findings
Participants showed similar lung function and quality of life scores across different fibrotic ILD subtypes.
Anxiety and depression were lower in IPF compared to non-IPF fibrotic ILD.
Asbestos exposure was the most common occupational exposure reported.
Abstract
Interstitial lung disease (ILD) represents a group of complex parenchymal conditions characterised by varying clinical trajectories. The It’s Not JUST Idiopathic Pulmonary Fibrosis Study seeks to identify genetic, proteomic and clinical biomarkers that distinguish rapidly progressive fibrotic phenotypes from stable phenotypes irrespective of aetiology. This manuscript presents baseline insights from the recruited cohort. In this prospective, longitudinal study, participants with fibrotic ILDs, including idiopathic pulmonary fibrosis (IPF), fibrotic hypersensitivity pneumonitis, rheumatoid arthritis-associated ILD, asbestosis and unclassifiable ILD, were enrolled from 24 UK sites. Participants underwent comprehensive baseline evaluation including demographics, exposure history, lung function testing, 6-min walk tests, blood sampling and standardised questionnaires to assess symptoms and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
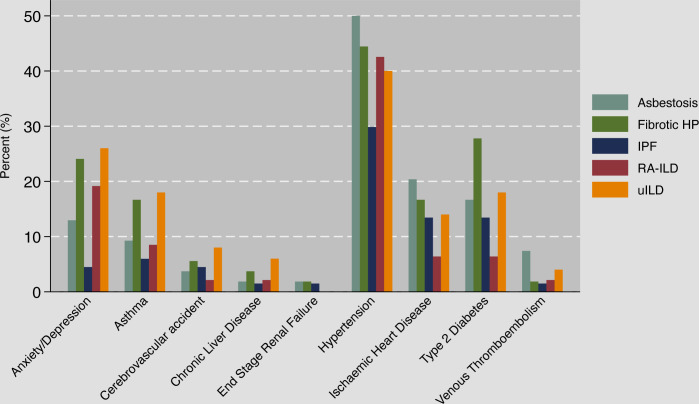 Figure 1
Figure 1| All (n=272) | IPF (n=67) | Non-IPF (n=205) | Asbestosis (n=54) | Fibrotic HP (n=54) | RA-ILD (n=47) | uILD (n=50) | P value | |
|---|---|---|---|---|---|---|---|---|
| Age, years | 71.3 (9.0) | 72.3 (7.8) | 71.0 (9.4) | 75.9 (6.3) | 68.6 (9.2) | 71.0 (8.1) | 68.0 (11.3) | <0.001 |
| Sex | ||||||||
| Male | 188 (69.1%) | 51 (76.1%) | 137 (66.8%) | 53 (98.1%) | 30 (55.6%) | 22 (46.8%) | 32 (64.0%) | <0.001 |
| Female | 84 (30.1%) | 16 (23.9%) | 68 (33.2%) | 1 (1.9%) | 24 (44.4%) | 25 (52.2%) | 18 (36.0%) | |
| Ethnicity | ||||||||
| White | 259 (95.2%) | 67 (100%) | 192 (93.7%) | 54 (100%) | 49 (90.7%) | 43 (91.5%) | 46 (92.0%) | 0.003 |
| Black | 3 (1.1%) | 0 | 3 (1.5%) | 0 | 0 | 1 (2.1%) | 2 (4.0%) | |
| Asian | 6 (2.2%) | 0 | 6 (2.9%) | 0 | 5 (9.3%) | 1 (2.1%) | 0 | |
| Other | 4 (1.5%) | 0 | 4 (2.0%) | 0 | 0 | 2 (4.3%) | 2 (4.0%) | |
| Smoking | ||||||||
| Current/ex | 181 (66.8%) | 41 (62.1%) | 140 (68.3%) | 41 (75.9%) | 31 (57.4%) | 34 (72.3%) | 34 (68.0%) | 0.02 |
| Never | 90 (33.2%) | 25 (37.9%) | 65 (31.7%) | 13 (24.1%) | 23 (42.6%) | 13 (27.7%) | 16 (32.0%) | |
| Pack-years | 19.5 (8-30) | 19 (9–33) | 19.7 (7.8–30) | 18.6 (10-27) | 10.5 (4.8–32) | 20 (8–36) | 20 (5.8–30) | 0.88 |
| BMI (kg/m2) | 29.1 (5.4) | 29.0 (4.9) | 29.2 (5.6) | 28.8 (4.7) | 29.5 (6.7) | 27.8 (3.9) | 30.6 (6.3) | 0.15 |
| Family history of ILD | 31 (11.4%) | 10 (15.2%) | 21 (10.2%) | 4 (7.4%) | 7 (13.0%) | 3 (6.4%) | 7 (14.0%) | 0.49 |
| Lung physiology | ||||||||
| FEV1 (% predicted) | 86.8 (23) | 87.6 (21.6) | 86.6 (23.5) | 87.9 (19.8) | 80.1 (25.5) | 92 (21.6) | 87.3 (25.6) | 0.12 |
| FVC, L | 2.85 (0.86) | 3.00 (0.89) | 2.80 (0.84) | 3.08 (0.71) | 2.55 (0.92) | 2.81 (0.86) | 2.78 (0.80) | 0.01 |
| FVC (% predicted) | 89.0 (21.1) | 90.6 (19.8) | 88.5 (21.5) | 93.7 (19.5) | 80.0 (21.1) | 93.4 (18.5) | 87.3 (24.3) | 0.01 |
| DLCO (% predicted) | 57.9 (17.3) | 58.3 (15.5) | 57.7 (17.9) | 59.4 (18.1) | 53.5 (17.0) | 60.0 (17.9) | 58.2 (18.4) | 0.39 |
| GAP score | 3 (2-4) | 3 (3-4) | 3 (2-4) | 3 (3-4) | 3 (2-4) | 3 (2-4) | 3 (2-4) | 0.02 |
| 6MWD (m) | 302 (120) | 311 (132) | 299 (116) | 276 (114) | 307 (116) | 298 (120) | 315 (114) | 0.49 |
| Time from diagnosis to enrolment (months) | 5.8 (1.9–14) | 8.8 (3.4–16.4) | 5.2 (1.8–13.0) | 4.7 (2.2–10.0) | 7.4 (1.9–18.0) | 7.5 (1.9–14.3) | 4.9 (1.3–9.9) | 0.17 |
| All (n=272) | IPF (n=67) | Non-IPF (n=205) | Asbestosis (n=54) | Fibrotic HP (n=54) | RA-ILD (n=47) | uILD (n=50) | |
|---|---|---|---|---|---|---|---|
| ALT (U/L) | 22.9 (11) | 24.0 (9.9) | 22.6 (11.3) | 20.7 (8.1) | 23.0 (12.1) | 20.7 (10.7) | 25.8 (12.8) |
| Albumin (g/L) | 39.6 (4.5) | 40.2 (3.4) | 39.5 (4.8) | 40.3 (4.4) | 39.7 (3.9) | 37.8 (3.9) | 40.0 (6.3) |
| Calcium (mmol/L) | 2.36 (0.1) | 2.34 (0.08) | 2.36 (0.1) | 2.36 (0.09) | 2.33 (0.1) | 2.35 (0.09) | 2.40 (0.11) |
| Haemoglobin (g/L) | 121.9 (45.3) | 128.3 (43.8) | 120 (45.7) | 117.2 (49.4) | 131.6 (32.4) | 107.9 (49.8) | 121.7 (48.2) |
| White cell count (109 /L) | 8.4 (2.5) | 8.4 (2.2) | 8.4 (2.6) | 7.7 (2.4) | 9.2 (2.7) | 8.8 (2.3) | 8.0 (2.7) |
| Platelets (109 /L) | 254.5 (68.4) | 246.2 (61.8) | 257.1 (70.2) | 240.4 (61.4) | 256.8 (54.3) | 286.2 (91.3) | 247.4 (64.8) |
| Neutrophils (109 /L) | 5.68 (2.43) | 5.42 (2.01) | 5.76 (2.55) | 4.96 (2.1) | 6.44 (2.75) | 6.32 (2.78) | 5.33 (2.24) |
| Eosinophils (109 /L) | 0.27 (0.26) | 0.29 (0.19) | 0.26 (0.27) | 0.31 (0.36) | 0.24 (0.23) | 0.23 (0.26) | 0.25 (0.21) |
| Monocytes (109 /L) | 0.66 (0.27) | 0.69 (0.28) | 0.65 (0.26) | 0.68 (0.27) | 0.66 (024) | 0.66 (0.25) | 0.61 (0.28) |
| Lymphocytes (109 /L) | 1.78 (0.78) | 1.96 (0.83) | 1.73 (0.75) | 1.66 (0.59) | 1.77 (0.81) | 1.71 (0.75) | 1.78 (0.86) |
| RhF | |||||||
| Positive | 42 (15.4%) | 3 (4.5%) | 39 (19%) | 1 (1.9%) | 4 (7.4%) | 29 (61.7%) | 5 (10%) |
| Negative | 79 (29%) | 27 (40.3%) | 52 (25.4%) | 12 (22.2%) | 21 (38.9%) | 3 (6.4%) | 16 (32%) |
| Not checked/unavailable | 151 (55.5%) | 37 (55.2%) | 114 (55.6%) | 41 (75.9%) | 29 (53.7%) | 15 (31.9%) | 29 (58%) |
| Anti-CCP | |||||||
| Positive | 23 (8.5%) | 2 (3%) | 21 (10.2%) | 0 | 2 (3.7%) | 17 (36.2%) | 2 (4%) |
| Equivocal | 4 (1.5%) | 1 (1.5%) | 3 (1.5%) | 0 | 0 | 3 (6.4%) | 0 |
| Negative | 73 (26.8%) | 24 (35.8%) | 49 (23.9%) | 11 (20.4%) | 16 (29.6%) | 6 (12.8%) | 16 (32%) |
| Not checked/unavailable | 172 (63.2%) | 40 (59.7%) | 132 (64.4% | 43 (79.6%) | 36 (66.7%) | 21 (44.7%) | 32 (64%) |
| ANA | |||||||
| Positive | 41 (15.1%) | 9 (13.4%) | 32 (15.6%) | 2 (3.7%) | 9 (16.7%) | 12 (25.5%) | 9 (18%) |
| Negative | 92 (33.8%) | 26 (38.8%) | 66 (32.2%) | 13 (24.1%) | 18 (33.3%) | 13 (27.7%) | 22 (44%) |
| Not checked/unavailable | 139 (51.1%) | 32 (47.8%) | 107 (52.2%) | 39 (72.2%) | 27 (50%) | 22 (46.8%) | 19 (38%) |
| pANCA | |||||||
| Positive | 20 (7.4%) | 3 (4.5%) | 17 (8.3%) | 1 (1.9%) | 7 (13%) | 3 (6.4%) | 6 (12%) |
| Negative | 48 (17.7%) | 11 (16.4%) | 37 (18.1%) | 4 (7.4%) | 15 (27.8%) | 5 (10.6%) | 13 (26%) |
| Not checked/unavailable | 204 (75%) | 53 (79.1%) | 151 (73.7%) | 49 (90.7%) | 32 (59.3%) | 39 (83%) | 31 (62%) |
| cANCA | |||||||
| Positive | 12 (4.4%) | 3 (4.5%) | 9 (4.4%) | 0 | 3 (5.6%) | 2 (4.3%) | 4 (8%) |
| Negative | 74 (27.2%) | 16 (23.9%) | 58 (28.3%) | 8 (14.8%) | 22 (40.7%) | 7 (14.9%) | 21 (42%) |
| Not checked/unavailable | 186 (68.4%) | 48 (71.6%) | 138 (67.3%) | 46 (85.2%) | 29 (53.7%) | 38 (80.9%) | 25 (50%) |
| All (n=272) | IPF (n=67) | Non-IPF (n=205) | Asbestosis (n=54) | Fibrotic HP (n=54) | RA-ILD (n=47) | uILD (n=50) | |
|---|---|---|---|---|---|---|---|
| Acids (industrial) | 30 (11%) | 9 (13.4%) | 21 (10.2%) | 10 (18.5%) | 5 (9.3%) | 3 (6.4%) | 3 (6%) |
| Asbestos | 98 (36%) | 15 (22.4%) | 83 (40.5%) | 54 (100%) | 9 (16.7%) | 10 (21.3%) | 10 (20%) |
| Bird | 110 (40.4%) | 28 (41.8%) | 82 (40%) | 22 (40.7%) | 24 (44.4%) | 22 (46.8%) | 14 (28%) |
| Cutting oils/fluids | 37 (13.6%) | 12 (17.9%) | 25 (12.2%) | 13 (24.1%) | 6 (11.1%) | 3 (6.4%) | 3 (6%) |
| Farm animals | 20 (7.4%) | 1 (1.5%) | 19 (9.3%) | 3 (5.6%) | 9 (16.7%) | 2 (4.3%) | 5 (10%) |
| Grain dust | 23 (8.5%) | 7 (10.5%) | 16 (7.8%) | 8 (14.8%) | 5 (9.3%) | 2 (4.3%) | 1 (2%) |
| Hairdressing products | 6 (2.2%) | 1 (1.5%) | 5 (2.4%) | 0 | 3 (5.6%) | 1 (2.1%) | 1 (2%) |
| Metal dust | 60 (22.1%) | 20 (29.9%) | 40 (19.5%) | 16 (29.6%) | 10 (18.5%) | 7 (14.9%) | 7 (14%) |
| Mineral dust | 69 (25.4%) | 13 (19.4%) | 56 (27.3%) | 29 (53.7%) | 9 (16.7%) | 8 (17%) | 10 (20%) |
| Paint | 46 (16.9%) | 7 (10.5%) | 39 (19%) | 17 (31.5%) | 8 (14.8%) | 4 (8.5%) | 10 (20%) |
| Paper dust | 30 (11%) | 9 (13.4%) | 21 (10.2%) | 7 (13%) | 8 (14.8%) | 3 (6.4%) | 3 (6%) |
| Textile dust | 33 (12.1%) | 8 (11.9%) | 25 (12.2%) | 12 (22.2%) | 6 (11.1%) | 6 (12.8%) | 1 (2%) |
| Welding fumes | 55 (20.2%) | 15 (22.4%) | 40 (19.5%) | 18 (33.3%) | 11 (20.4%) | 6 (12.8%) | 5 (10%) |
| Wood dust | 53 (19.5%) | 5 (7.5%) | 48 (23.4%) | 28 (51.9%) | 7 (13%) | 3 (6.4%) | 10 (20%) |
| All (n=272) | IPF (n=67) | Non-IPF (n=205) | Asbestosis (n=54) | Fibrotic HP (n=54) | RA-ILD (n=47) | uILD (n=50) | |
|---|---|---|---|---|---|---|---|
| IPARC | 9.5 (5-10) | 9 (4-14) | 10 (5–19) | 10 (6–18) | 10 (5–19) | 9 (3-20) | 9.5 (5-20) |
| KBILD | |||||||
| Total | 57.1 (14.6) | 58.2 (10.3) | 56.7 (15.8) | 54.6 (14.6) | 55.6 (12.4) | 60.2 (17.7) | 56.8 (18.0) |
| Breathlessness domain | 65.1 (24.9) | 69.9 (22.5) | 63.5 (25.4) | 58.7 (25.3) | 63.7 (24.5) | 69.9 (26.5) | 62.6 (24.9) |
| Activities domain | 44.7 (21.3) | 47.2 (18.2) | 43.8 (22.2) | 42.9 (19.7) | 41.6 (18.7) | 47.9 (22.9) | 43.4 (27.3) |
| Psychological domain | 58.9 (19.8) | 59.3 (16.7) | 58.8 (20.8) | 56.6 (20.0) | 58.5 (18.8) | 62.9 (22.9) | 57.4 (21.6) |
| EQ-5D-5L | |||||||
| Health score | 70 (50–85) | 75 (60–85) | 70 (50–80) | 70 (50–80) | 70 (50–85) | 71 (50–85) | 65 (50–90) |
| EQ-5D index | 0.80 (0.66–0.92) | 0.83 (0.73–0.94) | 0.79 (0.62–0.90) | 0.79 (0.66–0.88) | 0.81 (0.63–0.94) | 0.75 (0.57–0.89) | 0.75 (0.49–0.94) |
| MRC | |||||||
| Score | 2 (2-3) | 2 (2-3) | 2 (2-3) | 3 (2-3) | 2.5 (2-3) | 2 (2-3) | 2 (2-3) |
| 1 | 35 (13%) | 8 (12.3%) | 27 (13.2%) | 7 (13%) | 4 (7.4%) | 8 (17%) | 8 (16.3%) |
| 2 | 116 (43.1%) | 34 (52.3%) | 82 (40.2%) | 19 (35.2%) | 23 (42.6%) | 22 (46.8%) | 18 (36.7%) |
| 3 | 70 (26%) | 15 (23.1%) | 55 (27%) | 16 (29.6%) | 18 (33.3%) | 8 (17%) | 13 (26.5%) |
| 4 | 38 (14.1%) | 7 (10.8%) | 33 (15.2%) | 11 (20.4%) | 7 (13.0%) | 7 (14.9%) | 6 (12.2%) |
| 5 | 10 (3.7%) | 1 (1.5%) | 9 (4.4%) | 1 (1.9%) | 2 (3.7%) | 2 (4.3%) | 4 (8.2%) |
| LCQ | |||||||
| Total | 17.0 (13.2–19.4) | 17.4 (14.2–19.3) | 16.7 (12.9–19.5) | 15.9 (12.1–18.5) | 16.5 (13.1–18.7) | 18.8 (13.9–20.1) | 16.1 (11.8–19.5) |
| Physical | 5.5 (4.38–6.13) | 5.5 (4.63–6.38) | 5.5 (4.13–6.13) | 5.1 (3.9–5.9) | 5.4 (4.1–6.3) | 5.8 (4.9–6.5) | 5.3 (4.0–6.0) |
| Psychological | 5.86 (4.29–6.71) | 5.86 (4.57–6.57) | 5.71 (4.14–6.71) | 5 (4.0–6.6) | 5.4 (4.4–6.4) | 6.4 (4.7–6.9) | 5.9 (4.0–6.7) |
| Social | 5.75 (4.5–6.75) | 5.75 (5.0–6.75) | 5.75 (4.5–6.75) | 5.8 (4.5–6.8) | 5.6 (4.5–6.5) | 6.5 (4.5–7) | 5.5 (4.3–6.8) |
- —NIHR
- —Nottingham Biomedical Research Centre
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Inflammatory Myopathies and Dermatomyositis · Systemic Sclerosis and Related Diseases
Introduction
Interstitial lung disease (ILD) encompasses a heterogeneous group of inflammatory and fibrotic conditions of the lung parenchyma associated with substantial morbidity and mortality.1 Idiopathic pulmonary fibrosis (IPF) is often considered the archetypal progressive fibrotic ILD, yet a significant proportion of patients with other fibrotic ILDs including fibrotic hypersensitivity pneumonitis (fHP), rheumatoid arthritis-related ILD (RA-ILD) and unclassifiable ILD (uILD) demonstrate progressive disease behaviour and respond to antifibrotic therapies,24 suggesting potential common mechanistic pathways regardless of aetiology.
International consensus statements and expert perspectives have proposed criteria to define progressive pulmonary fibrosis (PPF) utilising a combination of clinical, physiological and radiological parameters.1 5 While these criteria are effective in identifying patients at increased risk of poor outcomes, crucially they primarily rely on the manifestation of irreversible fibrosis and lung function decline, rather than enabling the early identification of patients prior to disease progression. The recent extension of antifibrotic therapies to encompass PPF has generated an urgent need to identify novel biomarkers that can predict disease behaviour, facilitate early prognostication and guide therapy stratification, thereby enabling personalised medicine. Furthermore, such biomarkers have the potential to enhance our understanding of common disease pathways across fibrotic ILDs and inform future drug development. Although blood-based biomarkers reflecting various mechanistic pathways have been described in IPF,6 7 there remains a significant gap in our understanding of biomarkers applicable to other fibrotic ILDs.
The It’s Not JUST Idiopathic Pulmonary Fibrosis Study (INJUSTIS) is an on-going prospective, longitudinal cohort study across 24 sites in the UK involving incident diagnoses of IPF, fHP, RA-ILD, asbestosis and uILD.8 The study aims to explore and identify genetic, blood-based and clinical biomarkers that may distinguish distinct phenotypes of progressive fibrotic phenotypes irrespective of aetiology and traditional clinical, radiological and pathological phenotyping. We hypothesise that certain biomarkers and pathways are common to progressive fibrotic ILDs. Herein, the baseline demographic and medical characteristics of participants enrolled in INJUSTIS are presented, providing crucial insights and laying the foundation for subsequent analyses exploring predictive biomarkers and therapeutic targets.
Methods
Study design and participants
The comprehensive design and methodology for the INJUSTIS study have been previously described.8 The study enrolled participants aged 18 and older with multidisciplinary-confirmed diagnoses of fibrotic ILD, evidenced by reticulation and traction airway dilatation attributed to fHP, RA-ILD, asbestosis or uILD. Recruitment occurred at outpatient clinics across 24 UK sites. All participants with fibrotic ILD, irrespective of their progression status, were eligible for inclusion. Exclusions comprised individuals with inflammatory radiological changes lacking fibrosis, or those diagnosed more than 18 months before study commencement. RA-ILD was selected due to its established enriched association with a fibrotic, progressive phenotype compared with other connective tissue disease (CTD)-ILDs.9 Efforts were made to maintain consistency in recruitment numbers for each of the ILD subtypes to allow for meaningful comparisons. Additionally, a reference cohort comprising participants with IPF, diagnosed in accordance with internationally accepted criteria,1 10 was recruited. All patients presenting at outpatient clinics who met the study’s inclusion and exclusion criteria were approached for participation. The study was conducted in accordance with the protocol,8 and all participants provided written informed consent. The study was registered on clinicaltrials.gov (NCT03670576).
Participant history and procedures
Following enrolment and written informed consent, participants underwent a baseline visit where demographic characteristics and relevant medical information including comorbidities, medications, occupation and exposure history were recorded (online supplemental material). Blood samples were obtained for routine laboratory tests including a full blood count, with additional samples collected and processed, according to standardised operating procedures and stored at −80ºC prior to analysis. Antibody results, along with liver function tests and bone profile, were gathered from historical records. Physiological investigations, including spirometry, gas transfer and 6-min walk tests, were performed according to the American Thoracic Society (ATS)/European Respiratory Society (ERS) standards.11 12 DL_CO_ and FVC percent predicted values were calculated using Global Lung Initiative equations.13 14 Significant asbestos exposure was defined as 1 year of heavy exposure or 5–10 years of moderate exposure.
Patient-reported outcome measures were collected using standardised questionnaires. The Leicester Cough Questionnaire was used to evaluate cough impact, encompassing physical, psychological and social domains, with higher scores indicating reduced cough-related symptoms and improved quality of life.15 The Medical Research Council (MRC) dyspnoea scale was used to assess breathlessness severity based on activity level, up to a maximum score of 5, with higher scores indicating increased exertional breathlessness.16 IPF Prognostic Assessment and Referral to Care (IPARC) evaluated distress of IPF symptoms and their impact on daily activities, yielding a maximum score of 33, with higher scores indicative of greater symptom severity.17 King’s Brief ILD Questionnaire (KBILD) comprised breathlessness, activities and psychological domains, providing an overall score ranging from 0 to 100, with higher scores denoting better health-related quality of life (HRQOL).18 EuroQol 5-dimension 5-level(EQ-5D-5L) measured holistic health across physical, psychological and social domains, with an index score ranging up to 1, and a quantitative self-perceived health score ranging from 0 to 100, with 0 representing the worst imaginable health state and 100 representing the best.19
Data management and analyses
Locally generated data were entered into an encoded electronic case report form and stored (medrio EDC) under anonymous identifiers. Internal consistency checks were performed, and data were verified against source documents. The baseline database was locked on 29 January 2024, and statistical analyses were conducted using Stata V.18.0. Descriptive analyses were conducted to characterise the study population and provide an overview of baseline demographics and clinical characteristics, presented in tabular format, enabling comparisons between ILD subtypes. Categorical variables were summarised as frequencies and percentages, while continuous variables were described using means and SD or medians and IQRs. Group differences were analysed using independent t-tests or one-way analysis of variance for normally distributed continuous variables, Wilcoxon rank sum or Kruskal-Wallis test for non-normally distributed continuous variables and χ^2^ or Fisher’s exact tests for categorical variables. A significance level of p <0.05 was considered statistically significant. Missing data were handled by excluding cases with incomplete information from the respective analyses.
Patient and public involvement
Patients were actively involved in the design of the study and contributed to shaping its objectives and methodology. Patient representatives also reviewed and provided feedback on all patient-facing materials to ensure they were accessible, appropriate and aligned with patient priorities. A steering committee including an independent chairperson, clinicians, researchers and patient representatives was established and convened regularly.
Results
A total of 272 participants with a confirmed diagnosis of fibrotic ILD were recruited between November 2018 and May 2023, distributed across five diagnostic subtypes: IPF (n=67), asbestosis (n=54), fibrotic HP (n=54), RA-ILD (n=47) and uILD (n=50). The recruitment period was extended due to the COVID-19 pandemic, which adversely impacted patient recruitment. Although completion of recruitment to the IPF cohort preceded that of other subtypes, enrolment persisted across all subtypes until the predetermined sample size for each ILD subtype was attained to mitigate potential time-related bias. The median time from diagnosis to recruitment was 5.8 months (IQR 1.9–14) in the entire cohort, with no significant difference in time from diagnosis to enrolment across the ILD subtypes (p=0.17).
Clinical and demographic characteristics
All participants received a confirmed diagnosis through multidisciplinary team assessment, with surgical lung biopsy performed in 10 (3.7%) cases. Cryobiopsies were not performed, and bronchoalveolar lavage was carried out in 11 participants as part of an optional substudy. The IPF and non-IPF cohorts were predominantly male (76.1% IPF, 66.8% non-IPF), of white ethnicity (100% IPF, 93.7% non-IPF), with a smoking history (62.1% IPF, 68.3% non-IPF) and mean ages of 72.3±7.8 and 71.0±9.4 in IPF and non-IPF, respectively (table 1). Participants with asbestosis were older than other ILD subtypes on average (75.9 years ±6.3) and had the greatest proportion of male participants (98.1%). A positive family history of ILD in first-degree or second-degree relatives was reported in 15.2% (IPF) and 10.2% (non-IPF) of participants. Baseline percent predicted forced vital capacity (FVC) and gas transfer for carbon monoxide (DL_CO_) was comparable between IPF (FVC 90.6±19.8, DL_CO_ 58.3±15.5) and non-IPF (FVC 88.5±21.5, DL_CO_ 57.7±17.9). Participants with fibrotic HP had the greatest impairment in percent predicted lung function (FVC 80.0±21.1, DL_CO_ 53.5±17.0). The mean (SD) 6-min walk distance was 311 m±132 (IPF) and 299±116 (non-IPF), with notably reduced exercise tolerance observed in participants with asbestosis (276 m±114 m). The median ILD-gender-age-physiology(GAP) score was 3 in both IPF (IQR 3–4) and non-IPF (IQR 2–4) groups. Across specific ILD subtypes, median scores were consistent at 3, with a slightly higher lower bound (IQ 3–4) observed in asbestosis. Body mass index was 29.0±4.9 in IPF participants and 29·2±5.6 in non-IPF participants, showing little difference across the ILD subtypes.
Comorbidities and medications
Variations in the prevalence of comorbidities were observed, highlighting the diverse clinical profiles within the study population. Systemic hypertension emerged as the most prevalent comorbidity (40.8% overall) affecting 29.9% of IPF and 44.4% of non-IPF participants (figure 1, online supplemental table). The prevalence of systemic hypertension across non-IPF subtypes ranged between 40% and 50% (p=0.23). Notable prevalence rates were also observed for type 2 diabetes mellitus (16.5% overall; 13.4% IPF, 17.6% non-IPF), ischaemic heart disease (14.3% overall; 13.4% IPF, 14.6% non-IPF) and asthma (11.4% overall; 6% IPF, 13.2% non-IPF). Lower rates were observed for venous thromboembolism (3.3% overall; 1.5% IPF, 3.9% non-IPF) and a previous history of cerebrovascular accident (4.8% overall; 4.5% IPF, 4.9% non-IPF). Anxiety and depression were reported in 16.9% of participants (4.5% IPF, 21% non-IPF), suggesting potential associations between ILD subtype and mental health comorbidities. Within the non-IPF subtypes, the highest occurrence of anxiety and depression was in the uILD group (28%).
Baseline co-morbidities stratified by ILD subtypes. HP, hypersensitivity pneumonitis; ILD, interstitial lung disease; IPF, idiopathic pulmonary fibrosis; RA-ILD, rheumatoid arthritis ILD; uILD, unclassifiable ILD.
Treatments with protein pump inhibitors (54.4%), statins (52.6%) and anticoagulation (24.6%) were common, with no significant difference between IPF and non-IPF groups (online supplemental table). Among non-IPF participants (n=205), 103 individuals (50.2%) were not receiving any disease-specific treatment at baseline. A larger proportion of participants with non-IPF were receiving either corticosteroid or immunomodulatory therapy (43.9%) when compared with IPF subjects (9%). The difference was largely driven by immunosuppressant use among participants with fibrotic HP (53.7%) and RA-ILD (80.9%). In contrast, only 11.1% of individuals with asbestosis were receiving immunosuppressive therapy. Antifibrotics were prescribed to 13.6% of participants, with a higher prevalence in IPF (26.9%) compared with the non-IPF (9.3%) group (p<0.001).
Bloods
No significant differences were observed in alanine aminotransferase (ALT), albumin, calcium, haemoglobin levels or white cell counts (WCC) between IPF and non-IPF groups (table 2). Lower WCCs and neutrophil counts were observed in individuals with asbestosis compared with other ILD subtypes (p=0.02 and p=0.005, respectively). Platelet counts were comparable between IPF (246.2±61.8) and non-IPF groups (257·1±70.2). Significantly elevated platelet counts were observed in RA-ILD patients relative to other ILD subtypes (p=0.008), indicating potential inflammatory activity. Eosinophil, monocyte and lymphocyte counts did not significantly differ between IPF and non-IPF groups or across the different ILD subtypes. In terms of autoimmune markers, there were no significant differences in the prevalence of antinuclear antibodies, perinuclear antineutrophil cytoplasmic antibodies, cytoplasmic antineutrophil cytoplasmic antibodies, rheumatoid factor (RhF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies between IPF and non-IPF groups. Within ILD subtypes, RhF was markedly more prevalent in RA-ILD, with 61.7% testing positive compared with much lower percentages in other subtypes (p<0.001). Anti-CCP antibodies showed a similar pattern with 36.2% positivity in RA-ILD, significantly higher than other ILD subtypes (p<0.001).
Exposures
Previous occupational exposure was reported in 68.8% of participants (64.2% IPF, 70.2% non-IPF) (table 3). Asbestos exposure was the most prevalent, affecting 36% of the overall cohort (22.4% IPF, 40.5% non-IPF). Among non-asbestosis participants, 20.2% reported asbestos exposure, with significant exposure reported in 9.2%. Exposure to other agents was also common in the overall cohort, including mineral dust (25.4%), metal dust (22.1%), welding fumes (20.2%) and wood dust (19.5%). Bird exposure history was reported by 40.4% of all participants, with 41.8% of IPF and 40% of non-IPF reporting such exposure. There were no significant differences in bird exposure within the ILD subtypes (p=0.35). Among the cohort reporting bird exposure, budgies were the most frequently implicated (60%), followed by parrots (10.9%) and canaries (7.3%).
Quality of life scores
Participants reported a significant impact on HRQOL across various instruments (table 4). The median IPARC distress score was 9.5 (IQR 5–10), with no difference observed between IPF and non-IPF groups (p=0.07). The mean overall KBILD score was 57.1±14.6, with lower scores in the activity domain (44·7±21.3), compared with the breathlessness (65·1±24.9) and psychological domains (58·9±19.8). These observations were consistent across both IPF and non-IPF groups. The median MRC score was 2 (IQR 2–3) indicating significant breathlessness on exertion, with no variation between IPF and non-IPF (p=0.17). The median EQ-5D-5L index was 0.8 (IQR 0.66–0.92), indicating relatively poorer health states among non-IPF individuals (0.79, IQR 0.62–0.90), compared with those with IPF (0.83, IQR: 0.73–0.94) (p=0.03). The median visual analogue scale score was 70 (IQR: 50–85) with no difference observed between IPF and non-IPF (p=0.25). The overall LCQ score was 17.0 (IQR 13.2–19.4), with no discernible variation between IPF and non-IPF groups. However, significant divergence was observed in the physical domain across ILD subtypes (p=0.04) with lower scores recorded in asbestosis (5.1, IQR: 3.9–5.9) and higher scores noted in RA-ILD (5.8, IQR: 4.9–6.5).
Discussion
The INJUSTIS study aims to identify genetic, proteomic and clinical biomarkers that can predict progressive fibrotic phenotypes from more stable ones, regardless of aetiology. This comprehensive analysis of baseline demographic and clinical characteristics from recruited participants offers valuable insights that deepen our understanding of the nuanced similarities and differences across fibrotic ILD subtypes.
The participant demographic consistently comprised predominantly older white males with a history of smoking, aligning with established knowledge about common ILD risk factors.20 Male predominance was less pronounced in non-IPF conditions, suggesting potential differences in aetiology or exposure histories. The exception was in asbestosis, which was almost exclusively male, underscoring the occupational link to traditionally male-dominated industries such as construction and shipbuilding, where asbestos exposure is prevalent.21 Similarities in family history were reported across ILD subtypes, highlighting the possibility of shared genetic factors that could influence susceptibility or disease progression.22 Similarities in the impairment of baseline pulmonary function, specifically FVC and DL,CO, were observed across ILD subtypes, suggesting comparable severity at diagnosis, despite possible differences in aetiological factors. The relatively low proportion of IPF participants on antifibrotic therapy likely reflects early-stage disease at the point of recruitment, the short interval between diagnosis and enrolment and evolving access to antifibrotics over the recruitment period, which overlapped with updates to National Institute for Health and Care Excellence guidelines and prescribing practices.
Widespread presence of comorbid conditions including hypertension, ischaemic heart disease and diabetes was observed. While these findings may reflect the older, predominantly male demographic with a smoking history, further research is needed to explore the potential links between systemic inflammation, fibrosis and impacts on multiple organ systems.23 The systemic nature of these comorbidities highlights their potential role as risk factors for the development or progression of ILD. Biomarkers that can delineate the impact of such systemic diseases on ILD progression could be invaluable and may include markers of systemic inflammation, oxidative stress or other metabolic syndromes that exacerbate fibrotic pathways.24 25 These findings reiterate the importance of holistic care strategies and emphasise the need for complete cardiovascular and metabolic management alongside respiratory care.
Individuals with uILD exhibited higher rates of anxiety and depression compared with other ILD subtypes. In contrast, the lowest prevalence of anxiety and depression was observed in the IPF group. The inherent uncertainty and variability associated with a uILD diagnosis may lead to greater psychological stress and a diminished sense of control over the disease process. In IPF, the availability of more structured diagnostic and treatment pathways, alongside better-established support networks and greater understanding of natural history, likely provides patients with a clearer understanding of their condition and more effective psychological coping mechanisms. These findings indicate that psychosocial factors and mental health support need to be tailored specifically for different ILD subtypes, acknowledging that patient experiences and mental health needs can vary significantly depending on the nature and prognosis of the underlying disease. Despite the severity and variability of these diseases, HRQOL scores were similar across all subtypes, reinforcing the substantial impact of ILD on daily living and overall well-being. This observation reinforces the importance of incorporating quality of life measurements into routine clinical assessments and trials, ensuring that treatment plans and novel therapies address both the physical and emotional aspects of ILD.
The similarities in bird exposure across different ILD subtypes prompt a critical re-evaluation of how bird-related exposures are interpreted in the diagnostic process, particularly in fibrotic HP, where such exposures have traditionally been viewed as primary causative factors.26 27 This observation suggests that some diagnostic criteria may rely on anecdotal or unsubstantiated links between exposure and disease, which could lead to misclassification or overemphasis on certain environmental factors.28 Our findings suggest that bird exposure may represent a generalised environmental risk factor that could predispose or exacerbate underlying pulmonary conditions. This highlights the need for further research into gene-environment interactions in ILD as well as the importance of detailed environmental assessments and the development of biomarkers that can differentiate between aetiological factors.
This baseline analysis provides a foundation for further research on ILD biomarkers and disease mechanisms that could identify common fibrogenic pathways across ILD aetiologies. Future biomarker studies should aim to dissect the complex interactions between genetic susceptibility, environmental exposures and clinical manifestations of ILD. This integration of clinical, environmental and psychosocial factors should enable the development of predictive models of disease progression, response to therapy and overall patient outcomes. This multifaceted approach will foster personalised medicine strategies that effectively address the complex nature of ILD, enhancing prognostication and treatment for patients across various ILD subtypes. By addressing these elements comprehensively, future research can transcend traditional diagnostic boundaries, offering new insights into the aetiology of ILDs and fostering the development of innovative treatment paradigms.
The INJUSTIS study has several strengths, notably its prospective, multicentre design across 24 UK sites, providing a comprehensive baseline evaluation that includes detailed demographic, clinical and exposure histories, alongside extensive physiological and quality of life assessments. These elements contribute to a robust dataset that facilitates nuanced analyses of disease characteristics.
However, this study has limitations. The cohort predominantly consists of older white males with a history of smoking, which may limit the applicability of the findings to more diverse populations, including women and individuals from different ethnic backgrounds. The overall sample size was designed to distinguish between progressive and stable fibrotic ILD over the follow-up period and is not sufficient for granular ILD subtype comparisons. However, notable differences consistent with underlying diagnoses were observed (eg, treatment in non-IPF ILD; immunology in RA-ILD and exposures in asbestosis) alongside a surprising absence of differences in avian exposure. The median time from diagnosis to recruitment was under 6 months. Despite this, the IPF group was generally milder than other cohorts.29 Recruitment delays due to the COVID-19 pandemic led to potential survivor bias. In addition, the recruitment period was extended due to the COVID-19 pandemic, potentially introducing temporal biases. For instance, changes in treatment protocols and patient management practices over the extended recruitment period could affect the comparability of data collected at different times. Additionally, the reliance on patient-reported exposure histories and family history is subjected to recall bias, which may not accurately reflect environmental or inherited risk. Finally, the study faced challenges in recruiting equal numbers of participants across all ILD subtypes, particularly in the IPF group where recruitment was completed earlier. However, we mitigated this by over-recruiting in this group until the other subtypes achieved their target recruitment.
In conclusion, this baseline study provides a comprehensive evaluation of a fibrotic ILD cohort, offering insights into the similarities and distinctions across ILD subtypes. The demographic, clinical and exposure data, coupled with longitudinal follow-up, establish a robust foundation for future planned research integrating advanced genomic, transcriptomic and proteomic analyses, with a vision to support personalised treatment strategies in PPF.
Supplementary material
10.1136/bmjresp-2024-003112online supplemental file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Raghu G Remy-Jardin M Richeldi L et al Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline Am J Respir Crit Care Med 2022205 e 184710.1164/rccm.202202-0399 ST 35486072 PMC 9851481 · doi ↗ · pubmed ↗
- 2Ley B Newton CA Arnould I et al The MUC 5B promoter polymorphism and telomere length in patients with chronic hypersensitivity pneumonitis: an observational cohort-control study Lancet Respir Med 201756394710.1016/S 2213-2600(17)30216-328648751 PMC 5555581 · doi ↗ · pubmed ↗
- 3Ley B Torgerson DG Oldham JM et al Rare Protein-Altering Telomere-related Gene Variants in Patients with Chronic Hypersensitivity Pneumonitis Am J Respir Crit Care Med 201920011546310.1164/rccm.201902-0360 OC 31268371 PMC 6888660 · doi ↗ · pubmed ↗
- 4Flaherty KR Wells AU Cottin V et al Nintedanib in Progressive Fibrosing Interstitial Lung Diseases N Engl J Med 201938117182710.1056/NEJ Moa 190868131566307 · doi ↗ · pubmed ↗
- 5Pugashetti JV Adegunsoye A Wu Z et al Validation of Proposed Criteria for Progressive Pulmonary Fibrosis Am J Respir Crit Care Med 2023207697610.1164/rccm.202201-0124 OC 35943866 PMC 9952866 · doi ↗ · pubmed ↗
- 6Khan FA Stewart I Saini G et al A systematic review of blood biomarkers with individual participant data meta-analysis of matrix metalloproteinase-7 in idiopathic pulmonary fibrosis Eur Respir J 202259210161210.1183/13993003.01612-202134588192 PMC 9202487 · doi ↗ · pubmed ↗
- 7Maher TM Oballa E Simpson JK et al An epithelial biomarker signature for idiopathic pulmonary fibrosis: an analysis from the multicentre PROFILE cohort study Lancet Respir Med 201759465510.1016/S 2213-2600(17)30430-729150411 · doi ↗ · pubmed ↗
- 8Khan F Stewart I Howard L et al The Its Not JUST Idiopathic pulmonary fibrosis Study (INJUSTIS): description of the protocol for a multicentre prospective observational cohort study identifying biomarkers of progressive fibrotic lung disease BMJ Open Respir Res 20196 e 00043910.1136/bmjresp-2019-000439 PMC 656138231258922 · doi ↗ · pubmed ↗