A Rare Case of Allergic Bronchopulmonary Aspergillosis With Endobronchial Aspergilloma Causing Total Lung Collapse
Shakithya Thavakumar, Mohamed A Abdulla

TL;DR
A rare case shows how a fungal infection caused a lung to collapse and was successfully treated with a combination of procedures and medications.
Contribution
This paper presents a rare clinical case linking allergic bronchopulmonary aspergillosis with endobronchial aspergilloma leading to lung collapse.
Findings
A 70-year-old man's lung collapse was caused by a fungal ball in the bronchus.
Treatment with bronchoscopy, corticosteroids, and voriconazole led to full recovery.
The case emphasizes the need to consider fungal causes in atypical lung collapse presentations.
Abstract
We present a rare case of allergic bronchopulmonary aspergillosis (ABPA) with endobronchial aspergilloma in a 70-year-old man who presented with acute total collapse of the left lung. Initial imaging raised concern for malignancy, but bronchoscopy revealed a fungal ball obstructing the left main bronchus. Serological markers confirmed ABPA. Treatment with bronchoscopy-guided clearance, oral corticosteroids, and voriconazole led to complete clinical and radiological recovery. This case highlights the importance of considering fungal aetiologies in atypical presentations of lung collapse.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
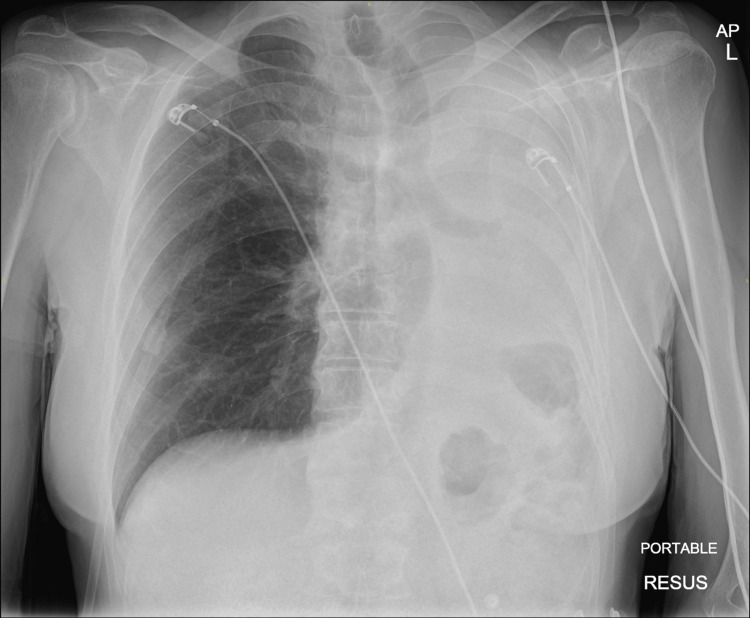 Figure 1
Figure 1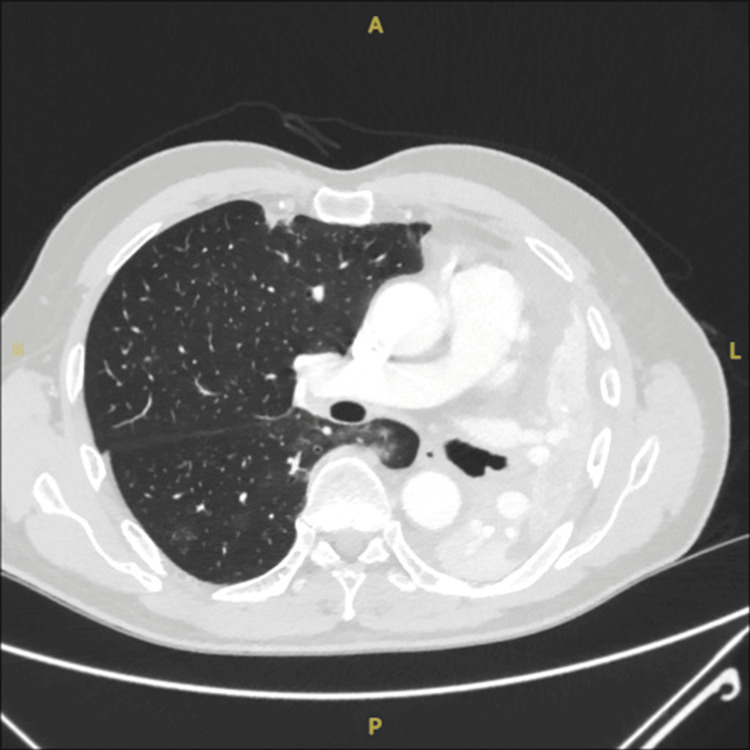 Figure 2
Figure 2 Figure 3
Figure 3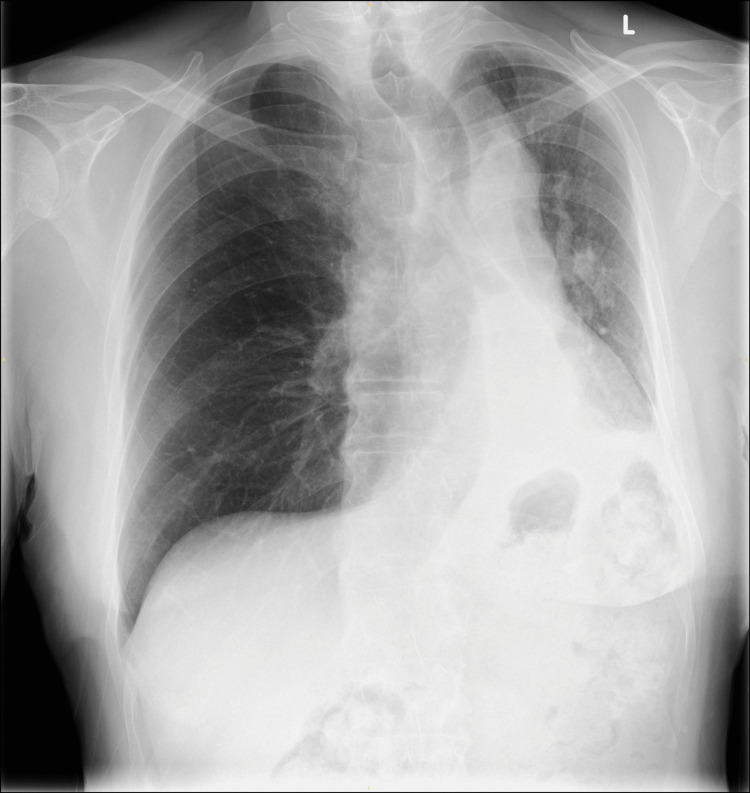 Figure 4
Figure 4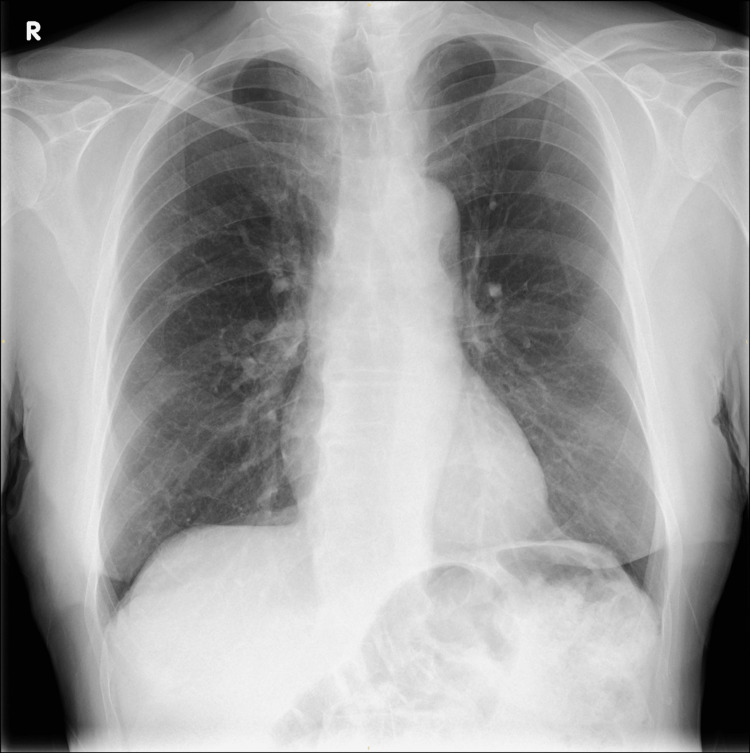 Figure 5
Figure 5| Parameter | Result | Reference Range |
| Haemoglobin | 14.2 g/dL | 13.5–17.5 g/dL |
| WBC | 10.5 ×10⁹/L | 4.0–11.0 ×10⁹/L |
| CRP | 12 mg/L | <5 mg/L |
| Eosinophils | 1.80 ×10⁹/L | 0.0–0.5 ×10⁹/L |
| Platelets | 250 ×10⁹/L | 150–400 ×10⁹/L |
| Creatinine | 65 mmol/L | 59–104 mmol/L |
| eGFR | >90 ml/min/1.73m2 | 60-89 ml/min/1.73m2 |
| Test | Result | Reference Range |
| Total IgE | 2855 IU/ml | <100 IU/ml |
| Aspergillus-specific IgE | 3.69 kUA/L | <0.35 kUA/L |
| Aspergillus-specific IgG | 107 mgA/L | <40 mgA/L |
| Vasculitis screen | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Infectious Diseases and Mycology · Fungal Infections and Studies
Introduction
Allergic bronchopulmonary aspergillosis (ABPA) is a hypersensitivity reaction to Aspergillus fumigatus, typically seen in patients with asthma or cystic fibrosis [1,2]. It is characterised by airway inflammation, eosinophilia, and elevated IgE levels, which can lead to bronchiectasis and lung damage if untreated [1,2]. Studies report that ABPA is found in approximately 2.5% of adults with asthma worldwide [3].
Aspergillomas usually form within lung cavities; however, endobronchial aspergilloma (EBA) is a rare manifestation in which fungal colonisation occurs within the bronchial lumen rather than the lung parenchyma [4-6]. EBA can present as an obstructive mass mimicking malignancy when associated with complete lung collapse [4-6]. Early recognition is crucial to avoid unnecessary oncological investigations and to initiate effective antifungal therapy [4,6].
Case presentation
A 70-year-old gentleman presented to the emergency department with a one-day history of acutely worsening shortness of breath at rest, accompanied by a persistent cough. He denied chest pain, haemoptysis, or weight loss. Over the preceding month, he had experienced a three-week history of exertional dyspnoea, cough, and intermittent low-grade fever, which he self-managed with paracetamol. He also received a salbutamol inhaler, a course of antibiotics and steroids from his primary care doctor; however, his respiratory symptoms failed to improve and progressively deteriorated, prompting hospital admission.
His past medical history is notable for childhood asthma, though he has had no recent respiratory symptoms and no history of smoking. In 2006, he underwent a cystectomy for bladder cancer, followed by neobladder reconstruction using intestinal tissue.
He had occupational exposure to various chemicals and oils while working as an electrician and later worked in underground mining management. During the COVID-19 pandemic lockdown, he acquired an allotment and spent time working on it.
He had no exposure to farm animals or birds but did have some contact with wet grass on his allotment prior to the onset of his illness.
On examination, he was visibly breathless while speaking. There were absent chest movements and breath sounds on the left side, with dullness to percussion. Heart sounds were normal. Oxygen saturation was 88% on room air, requiring FiO₂ 50% to maintain the target oxygen saturation of >94%. Heart rate was 123 bpm, regular; blood pressure was elevated at 173/93. He was afebrile on admission. Abdominal and neurological examinations were unremarkable.
Initial investigations
The initial laboratory investigations are shown in Table 1.
Imaging
Admission CXR showed complete white out of the left lung with tracheal deviation to the left indicating likely left lung collapse (Figure 1).
Chest X-ray showing complete white-out of the left lung with tracheal deviation.
CT Thorax/Abdomen/Pelvis confirmed complete collapse of the left lung with no mass identified (Figures 2, 3).
Slice of the CT scan just below the carina to show obstruction in the left main bronchus causing total left lung collapse.
CT thorax in the coronal section showing complete obstruction in the left main bronchus and complete left lung collapse with hyperinflation of right lung and mediastinal shift to the left with left rib crowding.
Initial diagnosis and management
Imaging raised suspicion for malignancy versus severe infection.
The patient was managed empirically with intravenous co-amoxiclav and oral clarithromycin, as well as supplemental oxygen to maintain adequate oxygenation.
Further investigations
The serology results are presented in Table 2.
The elevated total IgE and Aspergillus-specific IgE levels confirmed ABPA, while a negative vasculitis screen helped exclude other systemic inflammatory causes.
Due to the acute presentation with total lung collapse, urgent bronchoscopy was performed.
Bronchoscopy revealed a yellow, cheese-like fungal ball and mucus obstructing the left main bronchus. This provided both diagnostic confirmation and partial therapeutic clearance of the obstructing fungal mass.
The bronchoalveolar lavage sample confirmed Aspergillus fumigatus growth in culture. Histology was unfortunately not obtained.
Treatment
Following the identification of Aspergillus fumigatus and elevated serological markers of ABPA, antifungal therapy was initiated with intravenous voriconazole, which was later transitioned to oral therapy. As per the British Thoracic Society guidelines, in patients with more rapidly progressive ABPA or those with a large volume of disease, the recommended first-line antifungal therapy is voriconazole 200 mg twice daily [7].
Oral corticosteroids (prednisolone 30 mg once daily) were started to manage the hypersensitivity component of ABPA. All antibiotics were discontinued once the fungal aetiology was confirmed. Oxygen supplementation was successfully weaned within 24 hours post-bronchoscopy, and post-procedure imaging showed partial re-expansion of the left lung (Figure 4).
Chest X-ray performed on the day of discharge showing partial left lung re-expansion.
Outcome and follow-up
The patient was discharged on oral voriconazole for three months and a tapering corticosteroid regimen, with regular outpatient monitoring of liver function and serum drug levels by the respiratory pharmacist.
At follow-up, he had complete symptom resolution, normalised eosinophil count with normal chest X-ray (Figure 5) and successful steroid weaning.
Chest X-ray performed at the three-month follow-up in the respiratory clinic showing complete re-inflation of the left lung.
Discussion
EBA is a rare form of pulmonary aspergillosis, characterised by fungal growth within the bronchial lumen rather than the parenchyma [4-6]. Unlike classical aspergillomas, which typically form within pre-existing lung cavities, EBA produces endobronchial obstruction composed of fungal hyphae, mucus, and necrotic debris. This form of disease is often misdiagnosed due to its radiological resemblance to malignancy, especially when presenting with complete lung collapse [4,6,8].
Most reported cases occur in individuals with underlying lung conditions, including previous tuberculosis, bronchiectasis, or immunosuppression [5,8]. Our patient had no active asthma or structural lung disease, making this presentation particularly unusual. The absence of haemoptysis, weight loss, or systemic symptoms further complicated the initial diagnosis, leading to a working differential of malignancy versus infection.
Bronchoscopy plays a pivotal role in both diagnosis by allowing direct visualisation and management for relieving the obstructing fungal mass [1,4,9]. In our case, the visual identification of a cheesy yellow mass in the left main bronchus, along with positive cultures for Aspergillus fumigatus, confirmed the diagnosis. Histology was not obtained, which is a limitation, but serological markers, including elevated total IgE and Aspergillus-specific IgE, supported ABPA with EBA [2].
EBA is more frequently found in the left lung, possibly due to anatomical predisposition related to bronchial angulation and airflow patterns [10].
Reviews have shown that a combined management of bronchoscopy intervention and antifungal therapy, most commonly voriconazole, was effective in achieving resolution [1,5,6,9]. Corticosteroids are indicated in ABPA to control immune-mediated inflammation and prevent disease progression [2,6].
Another comprehensive review emphasised the importance of early bronchoscopy and fungal culture to avoid misdiagnosis and unnecessary oncological investigations [2].
Conclusions
This case highlights the importance of considering fungal aetiologies, including EBA, in patients presenting with acute lung collapse, even in the absence of classical risk factors.
Early bronchoscopy and fungal serology are essential for accurate diagnosis. Combined management with bronchoscopic clearance, systemic antifungal therapy, and corticosteroids can lead to complete clinical and radiological recovery, emphasising that EBA is a rare but treatable cause of airway obstruction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Endobronchial aspergilloma: a case report and literature review Exp Ther Med Huang D Li B Chu H 547554142017 https://pubmed.ncbi.nlm.nih.gov/28672965/2867296510.3892/etm.2017.4540 PMC 5488507 · doi ↗ · pubmed ↗
- 2Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria Clin Exp Allergy Agarwal R Chakrabarti A Shah A 850873432013 https://pubmed.ncbi.nlm.nih.gov/23889240/2388924010.1111/cea.12141 · doi ↗ · pubmed ↗
- 3Prevalence and features of allergic bronchopulmonary aspergillosis, United States, 2016-2022 P Lo S One Benedict K Gold JA Toda M Hsu J 0202025 https://pmc.ncbi.nlm.nih.gov/articles/PMC 11734977/10.1371/journal.pone.0317054 PMC 1173497739813272 · doi ↗ · pubmed ↗
- 4Endobronchial aspergilloma: report of 10 cases and literature review Yonsei Med J Ma JE Yun EY Kim YE 787792522011 https://pmc.ncbi.nlm.nih.gov/articles/PMC 3159936/2178644410.3349/ymj.2011.52.5.787PMC 3159936 · doi ↗ · pubmed ↗
- 5Endobronchial aspergilloma-a comprehensive literature review with focus on diagnosis and treatment modalities Eur J Clin Microbiol Infect Dis Ngu S Narula N Abureesh M Li JJ Chalhoub M 601605392020 https://pubmed.ncbi.nlm.nih.gov/31741102/3174110210.1007/s 10096-019-03726-5 · doi ↗ · pubmed ↗
- 6A case of endobronchial aspergilloma coexisting with lung adenocarcinoma Cureus El Hage H Fagel L 0122020 https://pubmed.ncbi.nlm.nih.gov/33403168/10.7759/cureus.11736 PMC 777329033403168 · doi ↗ · pubmed ↗
- 7British Thoracic Society Clinical Statement on Aspergillus-related chronic lung disease Thorax Brown JS Armstrong-James D Ayling-Smith J 321802025 https://thorax.bmj.com/content/80/Suppl_1/34040429410.1136/thorax-2024-222567 · doi ↗ · pubmed ↗
- 8Allergic bronchopulmonary aspergillosis Annu Rev Med Cockrill BA Hales CA 303316501999 https://pubmed.ncbi.nlm.nih.gov/10073280/1007328010.1146/annurev.med.50.1.303 · doi ↗ · pubmed ↗