Antimicrobial resistance in bloodstream isolates of Escherichia coli and Staphylococcus aureus from a provincial hospital, Cambodia, 2020–2022
Sivhour Chiek, Vichet Orn, Rina Dork, Sreypeou Hem, Sophanna Phai, Phally Kheng, Bunranai Thoeun, Seila Kak, Sidonn Krang, Sovann Ly, Sopheap Oeng, Paul Turner

TL;DR
This study reports high antimicrobial resistance rates in blood culture isolates of E. coli and S. aureus from a Cambodian hospital over three years.
Contribution
The study provides new data on AMR prevalence in provincial Cambodia, a region with limited surveillance.
Findings
74% of E. coli isolates were resistant to ceftriaxone, a common first-line antibiotic.
32% of S. aureus isolates were methicillin-resistant, but no vancomycin resistance was observed.
Only 2% of E. coli isolates showed resistance to imipenem, indicating lower resistance to this carbapenem.
Abstract
Antimicrobial resistance (AMR) is a global concern. However, in Cambodia, as in other countries in the World Health Organization’s Western Pacific Region, the magnitude of the problem is largely unknown. Thus, this study aimed to determine the prevalence of AMR in common pathogens, namely Escherichia coli and Staphylococcus aureus, isolated from blood cultures at one provincial hospital, a national sentinel site for AMR surveillance, during a 3-year period. Sample processing and analysis were conducted at the hospital’s on-site microbiology laboratory. Blood cultures were processed manually, and conventional methods were used for bacterial identification. Antibiotic susceptibility testing (AST) was performed by disk diffusion and Etest minimum inhibitory concentration measurement, in accordance with current Clinical and Laboratory Standards Institute guidelines. Blood culture data from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
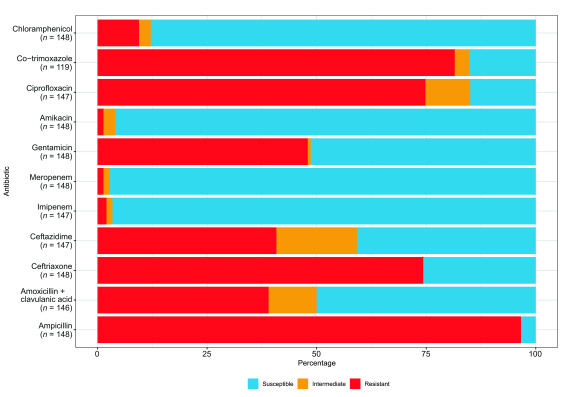 Fig. 1
Fig. 1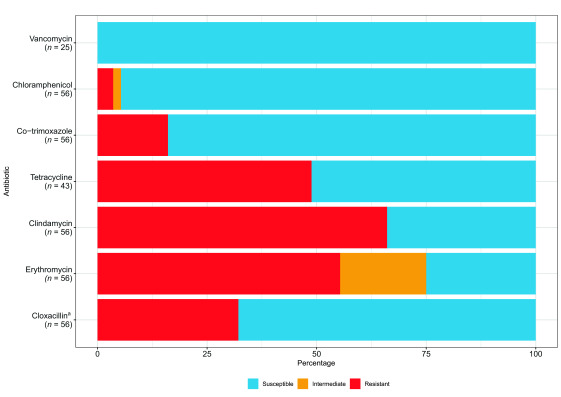 Fig. 2
Fig. 2| Species or species group | No. of isolates | % of true positive isolates |
|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Antimicrobial class | Antibiotic | Adulta | Paediatrica | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Susceptible | Intermediate | Resistant | Total | Susceptible | Intermediate | Resistant | ||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
| Antimicrobial class | Antibiotic | Adulta | Paediatrica | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Susceptible | Intermediate | Resistant | Total | Susceptible | Intermediate | Resistant | ||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Identification and Susceptibility Testing · Antimicrobial Resistance in Staphylococcus · Antibiotic Use and Resistance
Antimicrobial resistance (AMR) has emerged as a significant global public health threat, with nearly 5 million deaths linked to resistant bacteria in 2019. (1) Bacterial AMR also leads to treatment difficulties and longer hospital stays, resulting in increased health-care costs. (2)
It is essential to understand the true scale of AMR to inform risk management and identify opportunities for timely mitigation. The World Health Organization (WHO) established the Global Antimicrobial Resistance and Use Surveillance System (GLASS) in 2015 to enable countries to collect and share microbiological and antimicrobial use data. (3) This surveillance system targets six bacterial species commonly isolated from clinical samples globally, including Escherichia coli and Staphylococcus aureus, both dominant causes of bloodstream infections.
By the end of 2022, 92 countries had contributed AMR data to GLASS, including 10 from WHO’s Western Pacific Region. Despite the growth of the GLASS database, large gaps remain in the global AMR data set. (1) Although Cambodia has been reporting some data to GLASS since 2018, according to a review published in 2019, the scale of the AMR problem in Cambodia remains largely unknown. (4) This study aimed to provide contemporary data about AMR in Cambodia by determining its prevalence in E. coli and S. aureus isolated from blood cultures submitted between 2020 and 2022 to Battambang Provincial Referral Hospital (BPRH), one of several sentinel sites belonging to Cambodia’s national AMR surveillance system.
Methods
Study site
BPRH, located in the north-west of the country, is a complete level-3 health-care facility, with a catchment area of around 1 million people. The hospital has 390 beds and departments for adult medicine, surgery, paediatrics, intensive care and obstetrics. The on-site microbiology laboratory processes around 3600 clinical samples per year from hospitalized patients and those attending surrounding health-care facilities. The laboratory participates in the national external quality assurance programme.
Blood culture practices and processing
National standard operating procedures for AMR surveillance recommend blood culture for hospitalized patients with fever and a suspected bacterial infection. At BPRH, blood cultures are processed manually. For adults, 10 mL of blood are collected for culture from two different sites and inoculated into a pair of 100-mL aerobic culture bottles (containing brain–heart infusion broth + 0.025% sodium polyanethol sulfonate). For children, 1–5 mL of blood are inoculated into a single 50-mL aerobic bottle. The blood culture bottles are then incubated in a static incubator at 35 °C (± 2 °C) for up to 7 days. All bottles are checked daily for signs of growth, including for turbidity, gas bubbles and haemolysis. If growth is detected, the bottle is Gram stained and subcultured onto a range of media. Additionally, blind subculture to chocolate agar and Gram stain are performed after 1 day of incubation for all bottles. Bacterial identification is done using conventional methods: catalase and coagulase for S. aureus; and oxidase, indole, and a panel of five biochemical tests for E. coli and other Gram-negative bacteria.
Antimicrobial susceptibility tests (ASTs) are done by disk diffusion and measurement of Etest minimum inhibitory concentration, following Clinical and Laboratory Standards Institute guidelines and standards (M02 and M100). (5, 6) Specific species or groups of species were tested against standard panels of antimicrobial agents. Susceptibility to cefoxitin was tested as a surrogate agent for oxacillin and methicillin to report S. aureus resistance results for cloxacillin and cefazolin. Vancomycin was tested against S. aureus isolates only when cefoxitin resistance was detected.
Data analysis
Microbiology data were extracted from the national laboratory information system into a Microsoft Excel spreadsheet. Data were deduplicated to include only those results obtained from the first isolate per patient per year for each species (E. coli and S. aureus). Data summaries and graphs were generated using R, version 4.3.0 (R Core Team, Vienna, Austria), with the AMR, Harrell Miscellaneous (known as Hmisc) and tidyverse packages. (7) The χ^2^ test was used to explore trends in resistance to key GLASS surveillance antimicrobials (i.e. ceftriaxone for E. coli and methicillin for S. aureus).
Results
Hospital and laboratory summary
Between 1 January 2020 and 31 December 2022, 52 326 patients were admitted to BPRH: 17 947 in 2020, 16 312 in 2021 and 18 067 in 2022. During this period, 6102 blood cultures were processed by the microbiology laboratory: 5107 (84%) from hospitalized patients and 995 (16%) from patients attending external health-care facilities.
Blood culture data
Growth was detected in 826/6102 (14%) blood cultures. Of these, 297 were contaminated by skin flora (growth of coagulase-negative staphylococci, Micrococcus spp., Corynebacterium spp. or Bacillus spp.), leaving a total of 529 true positives. E. coli and S. aureus were the most common pathogens isolated from blood cultures, detected in 150 (28%) and 65 (12%) of positive cultures, respectively (Table 1).
Antimicrobial susceptibility data
Escherichia coli
After deduplication, there were 148 E. coli blood culture isolates with AST data (Fig. 1). Resistance to the following was common: ampicillin (143/148, 97%; 95% confidence interval [CI]: 92–99%), ceftriaxone (110/148, 74%; 95% CI: 67–81%), co-trimoxazole (97/119, 82%; 95% CI: 73–88%) and ciprofloxacin (110/147, 75%; 95% CI: 67–82%). Resistance to the following was rare: amikacin (2/148, 1%; 95% CI: 0–5%), imipenem (3/147, 2%; 95% CI: 0–6%) and meropenem (2/148, 1%; 95% CI: 0–5%). AST results stratified by patient’s age (< 18 years, ≥ 18 years) are summarized in Table 2. There was no trend in resistance to ceftriaxone over time (73% [30/41] in 2020, 77% [49/64] in 2021, and 72% [31/43] in 2022; χ^2^ for trend P = 0.90) (data not shown).
Antimicrobial resistance in Escherichia coli blood isolates, Battambang, Cambodia, 2020–2022
Staphylococcus aureus
After deduplication, there were 56 S. aureus blood culture isolates with AST data (Fig. 2). Resistance to methicillin was detected in around one third of isolates (18/56, 32%; 95% CI: 20–46%), but there was no evidence of resistance to vancomycin in the subset of isolates tested (0/25, 0%; 95% CI: 0–14%). AST results stratified by patient’s age are summarized in Table 3. There was no trend in methicillin resistance over time (44% [7/16] in 2020, 17% [3/18] in 2021, and 36% [8/22] in 2022; χ^2^ for trend P = 0.75) (data not shown).
Antimicrobial resistance in Staphylococcus aureus blood isolates, Battambang, Cambodia, 2020–2022
Discussion
Analysis of blood culture data from BPRH for 2020–2022 revealed that the most frequently isolated pathogens associated with bloodstream infections were E. coli and S. aureus; resistance to key first-line antibiotics was common in both species. More specifically, our study found that 74% of E. coli isolates were resistant to ceftriaxone and that 32% of S. aureus isolates were resistant to methicillin, proportions that are considerably higher than the 48% and 22%, respectively, reported by a nongovernmental hospital-based study conducted in Phnom Penh in 2007–2010. (8) However, resistance rates were similar to those reported to GLASS in 2022, when data were pooled from Cambodia’s eight sentinel surveillance sites (including this hospital). According to the pooled data, 74% (95% CI: 69–79%) of E. coli isolates were resistant to third-generation cephalosporins and 68% (95% CI: 62–100%) of S. aureus isolates were methicillin-resistant.
The AMR rates at BPRH for 2020–2022 were higher than those reported to GLASS by adjacent countries. For 2022, Thailand reported rates of 34% (95% CI: 31–36%) for resistance to third-generation cephalosporins in E. coli and 8% (95% CI: 6–9%) for methicillin resistance in S. aureus, with Lao People's Democratic Republic reporting rates of 53% (95% CI: 46–59%) and 56% (95% CI: 39–72%), respectively. Unfortunately, Viet Nam did not submit AMR data for 2022 to GLASS. (9)
With the current data, it is difficult to make meaningful comparisons of AMR rates between countries in the Region. Inherent biases in surveillance data, which can arise from differences in patient populations and selective utilization of clinical diagnostic microbiology, (10) are likely to generate either under or overestimates of the true burden of AMR prevalence. In many locations, including Cambodia, AMR surveillance is in the early stages of implementation, and prevalence estimates are prone to these types of biases. Nevertheless, several factors may be more specific to Cambodia and may have a bearing on its rates of AMR. For example, in many parts of the country, it is common for patients to seek treatment from private health-care providers or use antibiotic self-treatment before being admitted to a government hospital. This practice may contribute to the selection of AMR in bacteria and thus overestimate the true prevalence of AMR in blood cultures, by inhibiting the growth of susceptible organisms. (11) Such practices may also be indicative of the wider issue of the inappropriate and excessive use of antibiotics. Om et al., for example, found that the drivers of AMR in Cambodia encompass the improper use of antibiotics in humans, (12) marked by excessive reliance on broad-spectrum antibiotics such as ceftriaxone. (13)
There are several limitations to this current study. First, the data cover only a 3-year period and involve a relatively small number of isolates, limiting their representativeness. In addition, the data set is a blend of community-acquired and hospital-acquired infections. Furthermore, the absence of clinical data and the lack of comprehensive information regarding the patient population present challenges in determining the impact of AMR.
However, the study also has several strengths. The blood culture positivity rate was 9%, suggesting that clinician uptake of diagnostic microbiology services was reasonable, and this reflects a positive attitude towards identifying bacterial infections in patients presenting to BPRH. However, confirming adequate coverage would require an audit of the clinical records of patients with relevant clinical syndromes to determine blood culture collection metrics. Other strengths include good laboratory practice: the hospital laboratory had an established quality management system in place and followed Clinical and Laboratory Standards Institute guidance for AST, including annually updating breakpoints.
Based on the findings, recommendations for further work can be suggested. The national AMR surveillance system should be strengthened to include patient-level data to improve understanding of the impact of resistance on clinical outcomes and to guide targeted interventions. Given the widespread misuse of antibiotics, it will be important to begin to monitor antimicrobial use and its appropriateness, at least at national sentinel sites for AMR surveillance. Surveillance data should be collated regularly and used to inform the development of or changes to treatment guidelines and to optimize empirical therapy. Given the issues around inappropriate antibiotic use in Cambodia, surveillance data should be used to raise public awareness about the seriousness of AMR and to promote the responsible use of antibiotics.
In conclusion, high rates of AMR were demonstrated in E. coli and S. aureus isolates from patients with bloodstream infections from a Cambodian provincial referral hospital. Further work is required to understand the clinical impacts of this resistance and to identify potential mitigation strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Murray CJL, Ikuta KS, Sharara F, Swetschinski L, Robles Aguilar G, Gray A, et al.; Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022 Feb 12;399(10325):629–55. 10.1016/S 0140-6736(21)02724-035065702 PMC 8841637 · doi ↗ · pubmed ↗
- 2Prestinaci F, Pezzotti P, Pantosti A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog Glob Health. 2015;109(7):309–18. 10.1179/2047773215 Y.000000003026343252 PMC 4768623 · doi ↗ · pubmed ↗
- 3Global antimicrobial resistance surveillance system: manual for early implementation. Geneva: World Health Organization; 2015. Available from: https://iris.who.int/handle/10665/188783, accessed 27 July 2025.
- 4Reed TAN, Krang S, Miliya T, Townell N, Letchford J, Bun S, et al.; Cambodia Technical Working Group on Antimicrobial Resistance. Antimicrobial resistance in Cambodia: a review. Int J Infect Dis. 2019 Aug;85:98–107. 10.1016/j.ijid.2019.05.03631176035 · doi ↗ · pubmed ↗
- 5Performance standards for antimicrobial disk susceptibility tests. 13th ed. Wayne (PA): Clinical and Laboratory Standards Institute; 2018.
- 6Performance standards for antimicrobial susceptibility testing. 29th ed. Wayne (PA): Clinical and Laboratory Standards Institute; 2019.
- 7R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2025. Available from: https://cran.rstudio.com/manuals.html, accessed 23 July 2024.
- 8Vlieghe ER, Phe T, De Smet B, Veng HC, Kham C, Lim K, et al. Bloodstream infection among adults in Phnom Penh, Cambodia: key pathogens and resistance patterns. P Lo S One. 2013;8(3):e 59775. 10.1371/journal.pone.005977523555777 PMC 3612098 · doi ↗ · pubmed ↗