Healthy Lifestyle Interventions for Non-communicable Disease Prevention in Saudi Arabia: A Scoping Review
Alla Alhumaid, Abdulaziz Alotaibi, Mashael Tayeb, Yousef Alqhatani, Ibrahim Walbi

TL;DR
This review explores lifestyle interventions to prevent non-communicable diseases in Saudi Arabia, emphasizing diet, physical activity, and culturally tailored programs.
Contribution
The study synthesizes evidence on lifestyle interventions for NCD prevention in Saudi Arabia, highlighting culturally tailored and structured approaches.
Findings
Lifestyle interventions improved blood pressure, weight, and NCD risk reduction in Saudi populations.
Community initiatives and healthcare programs enhanced intervention effectiveness across diverse groups.
Culturally tailored programs and policy interventions are recommended to sustain long-term health benefits.
Abstract
Non-communicable diseases (NCDs), including diabetes, cardiovascular disease (CVD), and obesity, are considered major contributors to mortality and morbidity. Modifiable lifestyle determinants, including unhealthy diets and physical inactivity, play a major role in their progression. Interventions such as lifestyle modification are critical to reduce the onset of NCDs and improve the overall health of the population. This study aimed to synthesize the evidence on lifestyle interventions targeting NCD risk reduction among the population of Saudi Arabia by highlighting the implementing strategies, key outcomes, and recommendations. A scoping review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines, given the heterogeneity of the evidence in terms of population, study design, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
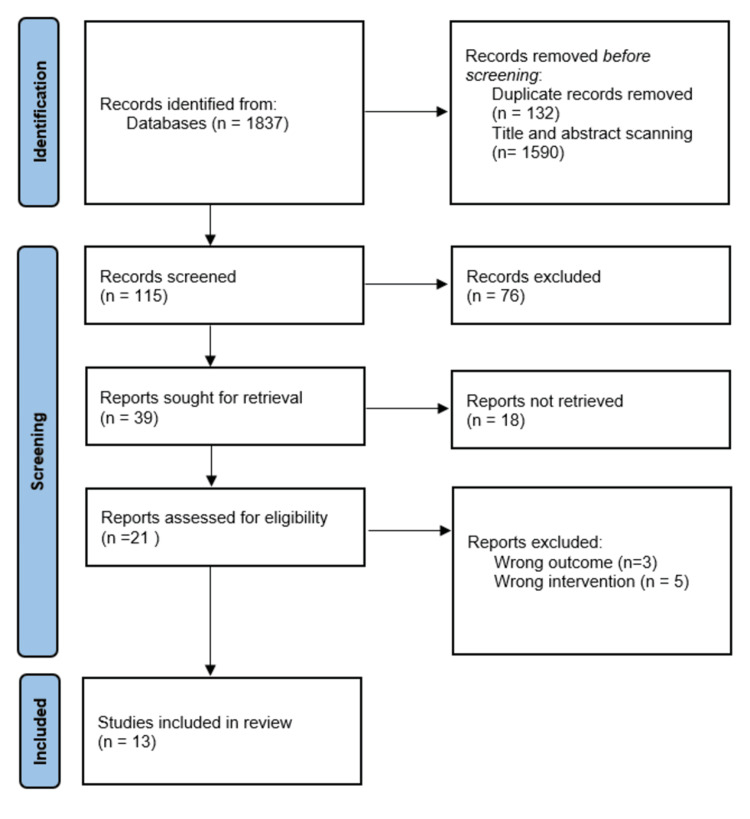 Figure 1
Figure 1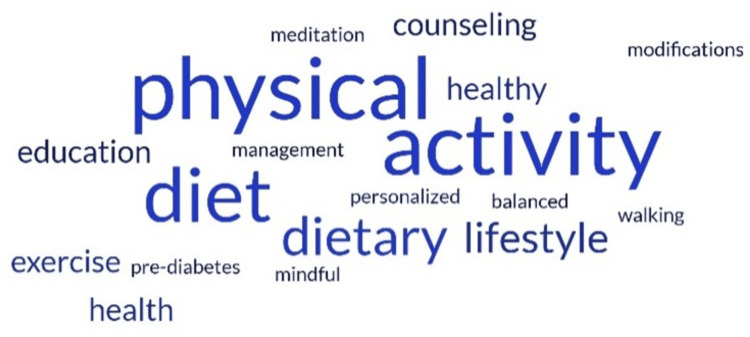 Figure 2
Figure 2| Item | Description |
| Population | General population of Saudi Arabia |
| Intervention | Lifestyle interventions such as physical activity, dietary modification, and mindfulness |
| Comparison | Not appliable |
| Outcome | Reduction in NCDs and risk factors |
| Study | Year | Research design | Lifestyle intervention | Effectiveness of intervention | Summary outcome | Recommendation |
| [ | 2016 | Clinical practice guideline | Personalized lifestyle interventions (diet + physical activity) | More effective than usual care; individualized counseling preferred | Strong emphasis on lifestyle interventions with physical activity + diet; conditional use of metformin, orlistat, and bariatric surgery | Recommend lifestyle interventions over usual care, individualized counseling, physical activity with diet, and conditional pharmacological/surgical interventions for obese adults |
| [ | 2023 | Systematic review | Physical activity, healthy diet, mindful meditation | Reduces risk or severity of cardiovascular disease (CVD) | Physical activity, mindful meditation, and diet effectively reduce CVD risk and address physical inactivity and poor diet in the Saudi population | Recommend regular physical activity, mindful meditation, and a balanced diet to reduce CVD risk and address lifestyle-related risk factors |
| [ | 2025 | Retrospective cross-sectional | Exercise (walking) and dietary changes for type 2 diabetes | Positive uptake; improved energy levels and well-being | 54.9% exercised regularly, 65.6% made dietary changes; culturally sensitive interventions were effective | Promote culturally sensitive exercise and diet interventions; implement policies supporting lifestyle advice in diabetes programs |
| [ | 2023 | Systematic review | Physical activity, dietary changes, and obesity reduction | Effective for reducing CVD risk | Physical inactivity (69.4%), unhealthy diets (34.4%), obesity, and smoking are major risk factors | Urgently promote lifestyle modifications; increase physical activity, improve diet, reduce obesity; public health campaigns are essential |
| [ | 2020 | Randomized controlled trial | Health education, exercise, and diet counseling | Significant improvements in blood pressure (BP), glucose, Framingham risk score (FRS) | Intervention group reduced systolic BP by 9.2 mmHg, glucose by 45 mg/dL, and FRS by 13.6 | Implement personalized lifestyle modification programs with health education, exercise, and diet counseling to reduce CVD risk among women |
| [ | 2021 | Retrospective before-and-after | Tawazon program: diet + physical activity for pre-diabetes | HbA1c, weight, body mass index (BMI), and lipid profiles improved | Phase I & II showed reductions in HbA1c, weight, BMI, and improved lipids | Implement maintenance sessions and online versions to sustain outcomes and expand accessibility |
| [ | 2022 | Systematic review | Physical activity counseling, structured programs | Improved physical activity levels, health parameters | Counseling improved smoking, diet, and exercise habits; barriers include lack of time and training | Train healthcare professionals in physical activity counseling; implement structured programs with educational materials and consultation time |
| [ | 2025 | Clinical practice guideline | Saudi Healthy Plate 2024 (balanced diet) | Nutritionally adequate, culturally appropriate | Meets most macro/micronutrient requirements; gaps in vitamin E and choline | Promote SHP-2024 dietary patterns; future updates should address nutrient gaps (vitamin E, choline) |
| [ | 2023 | Review | Diet + physical activity for obesity | Effective first-line therapy | Low-fat, low-calorie, low-carb, high-protein, low-glycemic index diets were effective; pharmacotherapy/surgery is reserved for later stages | Implement lifestyle management as first-line therapy; encourage exercise and diet; policy interventions to reduce obesity prevalence |
| [ | 2023 | Cohort | Blood pressure lifestyle management (BLSM) program | Mixed outcomes; subgroup improvements | Systolic BP decreased in hyperlipidemia and females; increased in males | Tailor the BLSM program to more participants; increase follow-up frequency for better BP control |
| [ | 2010 | Cross-sectional analysis | Health education via PHC (primary healthcare clinic) | Modest but significant improvements in diet and physical activity | Target vulnerable groups; improved dietary practices and physical activity | Emphasize high-quality health education in PHC; target women, older adults, and those with low education |
| [ | 2025 | Cross-sectional | Physical activity and dietary modifications | Associated with lower metabolic syndrome prevalence | Low activity and poor diet increased risk; interventions needed | Promote physical activity and a healthy diet among adults; implement public health education programs |
| [ | 2023 | Systematic literature review | Dietary modification | Addresses diabetes risk | Increased processed/sugary foods linked to higher diabetes prevalence | Develop interventions targeting dietary habits; promote healthier eating; and public health initiatives to reduce diabetes |
| Category | Description | Example |
| Individual factors | Personal limitations that hinder the adoption of healthy behaviors | Lack of motivation; low self-efficacy; poor adherence; limited awareness of disease risks |
| Behavioral barriers | Habits that conflict with healthy lifestyle choices | Unhealthy dietary habits; physical inactivity; smoking; stress eating |
| Sociocultural factors | Cultural norms and social expectations influencing behaviors | Social events centered on high-calorie foods; limited culturally tailored dietary guidance; norms discouraging regular exercise (especially among women) |
| Economic barriers | Financial limitations affecting access to healthy options | Costs of healthy foods; gym memberships; transportation to exercise facilities |
| Environmental and community factors | Physical environment that limits healthy choices | Limited availability of parks or walkways; lack of safe exercise spaces; limited access to fresh foods |
| Healthcare system barriers | Challenges within healthcare services that affect lifestyle counseling | Limited counseling time; insufficient provider training; low availability of structured programs; inadequate follow-up systems |
| Policy-level barriers | Gaps in national or institutional policies that reduce support for lifestyle change | Lack of large-scale public campaigns; inconsistent implementation of guidelines; limited monitoring or incentives |
| Technological barriers | Issues related to accessing digital or remote health tools | Low digital literacy; limited access to online platforms or apps; poor integration of technology in primary healthcare clinics |
| Psychological barriers | Mental or emotional obstacles that affect readiness for change | Stress, anxiety, depression, fear of failure, lack of perceived susceptibility to disease |
| Time and lifestyle constraints | Competing priorities and time limitations | Workload; family responsibilities; irregular schedules preventing routine exercise or meal planning |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes, Cardiovascular Risks, and Lipoproteins · Nutritional Studies and Diet · Health Promotion and Cardiovascular Prevention
Introduction and background
Non-communicable diseases (NCDs) such as diabetes, obesity, cardiovascular disease (CVD), and metabolic syndrome represent a major cause of mortality and morbidity across the world and are on the rise in Saudi Arabia, accounting for approximately 73.2% of all mortality and morbidity in the Kingdom [1]. Certain lifestyle risk factors, such as unhealthy dietary habits, smoking, and physical inactivity, exacerbate these conditions. Addressing these modifiable risks through targeted interventions is critical to reduce disease burden and improve population health outcomes [1,2].
Recent studies have emphasized the effectiveness of lifestyle interventions that integrate physical activities, dietary modifications, behavioral strategies, and structured counseling. Furthermore, clinical practice guidelines highlight the importance of personalized approaches that combine exercise counseling, diet, and, when necessary, pharmacological or surgical intervention for the treatment of severe obesity. The Saudi Healthy Plate 2024 (SHP-2024) further provides valuable recommendations in the context of Saudi Arabia [2,3]. However, despite existing guidelines and evidence supporting the effectiveness of lifestyle interventions in Saudi Arabia, several barriers remain, including limited training for healthcare providers, insufficient patient awareness, and low adherence to or compliance with the recommended practices [4]. As a result, public health initiatives play a crucial part in promoting lifestyle modification, particularly among populations at high risk, such as older adults and those with lower levels of education, given that previous studies reported a significant relationship between increased physical activity and optimal weight (p = 0.04) [5-7].
Despite the increasing burden of NCDs in Saudi Arabia, evidence on lifestyle interventions remains fragmented, as existing studies frequently focus on specific diseases, individual behaviors, and/or non-Saudi populations, thereby limiting their relevance to the local context. Therefore, this scoping review aims to summarize, synthesize, and evaluate the current evidence on lifestyle interventions targeting NCD risk reduction in Saudi Arabia by mapping the interventions, key outcomes, and recommendations. Lifestyle interventions are defined as structured or semi-structured programs managing behaviors in terms of dietary modification, physical activity, and weight management, while NCDs refer to chronic conditions including diabetes, cardiovascular diseases, and obesity. While NCDs risk reduction is operationalized as improvements in clinical, behavioral, or metabolic outcomes associated with lower disease risk. By consolidating the evidence, this review provides insights into effective and contextually appropriate strategies to reduce the burden of NCDs and improve population health in Saudi Arabia.
Review
Methods
Literature Search Strategy
This scoping review was conducted by using major databases and search engines, including PubMed, Web of Science, and Google Scholar, which cover recent studies published from January 2015 to September 2025. The keywords used in the search included “lifestyle interventions,” “physical activity,” “diet modification,” “weight management,” “cardiovascular disease,” “diabetes,” “Saudi Arabia,” and “non-communicable diseases.” In each database and search engine, the Boolean operators (AND, OR) were used to combine keywords and refine the search term (Appendix 1). Additionally, to improve the coverage of local and context-relevant interventions, other sources were included, such as government reports (e.g., SHP-2024) and clinical practice guidelines. Moreover, references from the identified studies were also screened for additional studies that were not captured in the initial search. Title/abstract and full-text screening were conducted by two independent reviewers, and any disagreements were resolved through discussion and consensus.
To assess a wide spectrum of interventions, the scoping review included primary and secondary studies, such as randomized controlled trials, clinical practice guidelines, systematic reviews, and retrospective studies following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. Table 1 shows the elements of the research question, which was developed based on the PICO (Population, Intervention, Comparison, and Outcome) model [8].
Inclusion and Exclusion Criteria
The studies included in this review examined lifestyle interventions implemented in Saudi Arabia, focusing on dietary changes, behavioral counseling, or mindfulness-based programs, and reported effectiveness outcomes such as increased physical activity or reduced risk factors. Studies that focused solely on surgical or pharmacological interventions without a lifestyle component were excluded. Commentaries, editorials, and conference abstracts were also excluded if they lacked sufficient methodological detail or were conducted outside Saudi Arabia.
Data Extraction
A standardized data extraction form was created to systematically capture key information from each study, including year of publication, study design, type of lifestyle intervention, effectiveness outcomes, summary findings, and recommendations. Data extraction was performed independently by two reviewers, with any discrepancies resolved through consensus.
Data Synthesis
A comprehensive narrative synthesis approach was used due to the heterogeneity of the research designs, interventions, and outcomes. This approach highlights the key findings and summary outcomes. The recommendations from each study were integrated to identify and unify common themes and evidence-based guidance applicable to the Saudi population through a word cloud and the development of a theme. This involved developing a preliminary synthesis through structured tabulation, examining patterns and relationships across the studies, and presenting an evidence-based narrative summary in accordance with scoping review methodology and the Popay et al. [9] framework.
Results
Characteristics of Included Studies and Interventions
This review synthesized findings across 13 studies examining lifestyle interventions for reducing risk factors of NCDs in the context of Saudi Arabia. The studies involved employed diverse research designs such as clinical practice guidelines, systematic review, retrospective design, cross-sectional, and randomized controlled trials (Figure 1).
Flow chart depicting the study selection process
Among these studies, the most commonly reported lifestyle interventions included physical activities, diet modifications, and structured health education, as well as certain mindfulness practices or cultural programs (Table 2).
Effectiveness of Lifestyle Interventions and Cultural Sensitivity
Clinical practice guidelines emphasize personalized and customized lifestyle interventions, which combine physical activity and diet modification more effectively than usual care. Individualized counseling was also preferred over generic approaches, and surgical options or pharmacological interventions such as metformin or orlistat were suggested for severe obesity among adults [10]. Similarly, the SHP-2024 guideline [3] provided culturally appropriate dietary recommendations that met most macronutrient and micronutrient requirements, though gaps in vitamin E and choline were identified, underscoring the need for targeted updates in future dietary guidelines.
Certain conditions revealed the impact of lifestyle modification on CVD and metabolic health conditions. For instance, one study revealed that physical activity, a balanced diet, and mindfulness mitigated disease severity and reduced CVD risk [11]. Another study reported that unhealthy diets (34.4%), physical inactivity (69.4%), obesity, and smoking were major contributors to CVDs [13]. Moreover, recommendations that were reported to overcome risks and improve health included public health campaigns targeted at lifestyle interventions. Additionally, structured physical activity counseling improved patient adherence to exercise, diet, and smoking habits. Barriers were noted, however, such as training for healthcare providers and limited time [16].
Other research designs, such as cohort studies and randomized controlled trials, provided valuable evidence of intervention effectiveness. For instance, programs such as personalized interventions, including exercise, health education, and diet counseling, resulted in significant improvements in blood glucose (−45 mg/dL), systolic blood pressure (−9.2 mmHg), and Framingham risk score (−13.6) among females at moderate to high CVD risk [14]. Other programs, such as the Tawazon program, produced observable reductions in weight, body-mass index, HbA1c, in addition to lipid profiles in adults with pre-diabetes. Additionally, recommendations were made to maintain online adaptations and sessions to sustain healthy outcomes and enhance accessibility [15].
In terms of cultural sensitivity, one study showed that 54.9% of patients with type 2 diabetes exercised frequently in addition to adopting regular dietary changes (65.6%), which improved overall well-being and energy levels [12]. Another study evaluated a blood pressure lifestyle management program and found positive outcomes overall in terms of improvements in systolic blood pressure among patients with hyperlipidemia, which indicates that a program aiming at lifestyle management can be effective and can vary by demographic and health status [18].
Integration, Public Health, and Sustainability of Lifestyle Interventions
In regard to the primary healthcare role and public health initiatives, health education significantly improved physical activity and dietary practices, in particular among older adults, women, and lower-educated populations. Given the urgency reported in terms of poor dietary habits and low physical activity, which are associated with a higher prevalence of risk factors related to health outcomes, there is a need for targeted public health interventions promoting healthy eating and exercise [19, 20].
Certain recommendations were made to address dietary factors, including the consumption of processed and sugary foods, which contribute to a higher diabetes prevalence. Recommendations include promoting healthier eating habits and controlling diets [21]. Furthermore, combining diet with physical activity serves as a first-line therapy for obesity management, with surgical and pharmacotherapy interventions reserved for severe or treatment-resistant conditions [17].
This evidence collectively indicates that lifestyle interventions that combine and integrate dietary modifications, physical activity, and health education are considered effective in reducing NCDs and the risk factors in Saudi Arabia. Furthermore, structured programs demonstrate robust methods of intervention with the greatest impact. In addition to public health programs, which involve ongoing monitoring and policy support, are essential to sustain long-term population-wide benefits.
Barriers and Core Components of Lifestyle Interventions
Table 3 lists the potential barriers associated with lifestyle modification. These barriers include differences in personal habits, environmental limitations, gaps in the healthcare system, and cultural and traditional factors. For instance, many people struggle with poor motivation due to improper eating habits or physical inactivity. Similarly, healthcare providers frequently lack the necessary expertise or time to provide lifestyle counselling to patients in order to reduce the burden of NCDs and improve care.
Figure 2 illustrates the word cloud, which provides the most prominent keywords in terms of lifestyle interventions such as “physical activity”, “diet”, “dietary”, and “lifestyle”, demonstrating the central position of these concepts in this comprehensive review. Furthermore, certain high-frequency keywords reported, such as “healthy”, “balanced”, “personalized”, and “management”, highlight the need for individualized and structured approaches to lifestyle modification. Nonetheless, Additional terms reported, such as “education”, “exercise”, “walking”, “mindful”, “meditation”, and “counseling”, reflect the broader educational components and behavioral acts commonly integrated into lifestyle interventions. While words such as “pre-diabetes”, “health”, and “modifications” suggest a coherent core on risk reduction, NCD prevention, and maintaining the modification of healthy behavior. Overall, the word cloud reflects the research domain dominated by the integration of physical activity and dietary change as foundational pillars of lifestyle management.
Lifestyle intervention word cloudAuthor creation via https://www.freewordcloudgenerator.com/generatewordcloud
Discussion
Overview of Findings
This scoping review examines lifestyle interventions targeted at the reduction of NCDs and their risk factors in Saudi Arabia. The collective evidence indicates that culturally tailored programs and interventions combining personalized physical activity, structured counseling, and dietary modifications in addition to behavioral strategies are effective in improving health outcomes, including cardiovascular and metabolic outcomes across diverse populations. Interventions involving physical activities were reported to improve energy balance and overall well-being and reduce cardiovascular risk, which corroborates global evidence that physical activities such as exercise are a cornerstone of NCD prevention. Similarly, dietary interventions including culturally adapted guidelines such as the SHP-2024 were reported to be associated with significant improvement in glycemic control, lipid profiles, and weight management, although certain gaps were identified in micronutrient intake [3].
Key Components of Lifestyle Interventions
The terms identified across these studies, such as “physical activity,” “diet,” and “dietary lifestyle,” underscore their importance as cornerstones of lifestyle interventions. Furthermore, their prominence implies a robust consensus that increasing physical activity and modifying nutritional management constitute the major strategies for managing and preventing NCDs, particularly metabolic risk conditions and diabetes. Moreover, the presence of terms such as “personalized,” “healthy,” “balanced,” and “management” points toward a shift to patient-centered approaches, aligning with recent guideline endorsements, which advocate for structured behavioral support and individualized counseling. In addition, keywords such as “counseling,” “education,” “meditation,” “mindful,” and “walking” suggest that lifestyle interventions are increasingly integrating physical, educational, and behavioral activities, which broadens the scope beyond traditional and generic diet and exercise frameworks. These multifactorial interventions, which combine nutrition management, psychological approaches, physical activity, and continual education, have long-term effects.
Effectiveness of Public Health Initiatives and Personalized Interventions
Regarding prevention and management, the inclusion of “pre-diabetes” and “health” shows the significance of these interventions in terms of lifestyle modification, particularly among populations with elevated health risks. Furthermore, the word cloud illustrates and aligns with the literature, reflecting the comprehensive understanding and development of lifestyle intervention concepts as a multidimensional approach in improving the population’s health.
Personalized and customized lifestyle interventions, which incorporated physical activities and diet alongside counseling and behavioral management, contributed to clinically meaningful risk-factor reduction, including cardiovascular factors, BMI, HbA1c, and blood pressure [22]. Similarly, the Tawazon program reinforced the effectiveness of personalized interventions, particularly when supplemented with adaptations and maintained sessions to enhance adherence [3]. Furthermore, mindfulness and behavioral approaches further verified the long-term commitment, reinforcing the benefit of resolving barriers to lifestyle modifications [23].
Public health and primary healthcare service initiatives played a major role in lifestyle management across various populations, in particular among lower-education groups, which highlights the urgent need for targeted interventions for high-risk populations [23]. Various barriers were reported, however, such as a lack of consistent program implementation, inadequate training of the healthcare provider, and low adherence among certain populations, which could reduce the efficiency of interventions [24].
Implications for Policy and Practice
The results provide valuable contributions for policy and practice, given the culturally sensitive nature, in addition to the personalized and structured lifestyle interventions, which promote and prioritize among the community and clinical settings that are supported by health campaigns, health policies, in addition to digital health approaches, which ultimately improve accessibility and sustainability.
Limitations and Future Research Directions
As with any review, the findings are influenced by the availability and quality of the included studies, which varied in design, sample size, and follow-up duration. Additionally, the scope of the search and inclusion criteria may have limited the comprehensiveness of the evidence captured, such as language restriction in English or publication bias. These factors should be considered when interpreting the results, and the findings should be viewed as a broad overview of the current state of knowledge rather than definitive conclusions. Future studies should focus on the analysis of cost-effectiveness and long-term follow-up of interventions that integrate digital and behavioral tools to optimize outcomes and adherence.
Conclusions
Personalized and contextual lifestyle interventions that integrate physical activity and dietary modification in addition to behavioral and structured counseling can effectively support the reduction of NCDs and their risk factors in Saudi Arabia. Research designs from various intervention types consistently provide evidence for the reduction of risk, such as CVD, weight increase, and high lipid profiles. Moreover, optimal impact can be achieved by combining lifestyle interventions and behavioral strategies, with enhancement in access to primary healthcare and public health initiatives that improve adherence among high-risk groups. To sustain long-term benefits at the population level, however, these interventions must be systematically monitored, and policy implementation at the national level must be improved by leveraging digital health solutions and addressing barriers for healthcare providers and patient adherence in the Kingdom of Saudi Arabia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Noncommunicable Diseases in Saudi Arabia: Toward Effective Interventions for Prevention Alqunaibet A Herbst C El-Saharty S Algwaizini A Washington, DC World Bank 2021 https://agris.fao.org/search/en/providers/122582/records/647481 f 9bf 943c 8c 7988 a 447
- 2Lifestyle diseases: the link between modern lifestyle and threat to public health Saudi J Med Pharm Sci Balwan W Kour S 17918442021
- 3Saudi Healthy Plate-2024: framework for developing, modeling, and evaluating Saudi Arabia's dietary guidelines BMC Nutr Alhumaidan OA Alkhunein SM Alakeel SA 1601120254077536710.1186/s 40795-025-01146-7PMC 12330179 · doi ↗ · pubmed ↗
- 4Factors associated with non-compliance with healthcare accreditation in Saudi Arabia: a systematic review and meta-analysis Healthcare (Basel) Alkhurayji KS Alsuhaimi A Alangari H Alrayes SA Alumran A 5713202510.3390/healthcare 13060580 PMC 1194228040150430 · doi ↗ · pubmed ↗
- 5Staff perceptions of addressing lifestyle in primary health care: a qualitative evaluation 2 years after the introduction of a lifestyle intervention tool BMC Fam Pract Carlfjord S Lindberg M Andersson A 991320122305215010.1186/1471-2296-13-99PMC 3515336 · doi ↗ · pubmed ↗
- 6Public health and primary health care: opportunities and challenges Med Flum Slivšek G. Vitale K Škarić-JurićT 89602024
- 7Challenges to lifestyle modification of chronic disease patients attending primary health care centers in Riyadh J Family Med Prim Care Alshammari SA Al Dhayan AZ Saad Al-Essa OM Alosaimi MM Al-Badr BM Ali AB Ajlan QA 61866193920203368106210.4103/jfmpc.jfmpc_1037_20PMC 7928105 · doi ↗ · pubmed ↗
- 8The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review J Med Libr Assoc Eriksen MB Frandsen TF 42043110620183027128310.5195/jmla.2018.345PMC 6148624 · doi ↗ · pubmed ↗