A PTH Value at 6 Hours Postsurgery Predicts the Diagnosis of Transient and Permanent Hypoparathyroidism
Ana Segarra-Balao, Juan de Dios Barranco-Ochoa, María de Damas-Medina, Beatriz Andrea Sánchez-Arquelladas, Eva Antonaya-Rubia, Carmen Rosa-Garrido, María Josefa Martínez-Ramírez, Alberto José Moreno-Carazo

TL;DR
A PTH level measured 6 hours after thyroid surgery can accurately predict whether a patient will develop temporary or permanent hypoparathyroidism.
Contribution
The study identifies a specific PTH threshold at 6 hours post-surgery that effectively predicts both transient and permanent hypoparathyroidism.
Findings
A PTH level <10.10 pg/mL at 6 hours postsurgery predicts transient hypoparathyroidism with high accuracy (AUC = 0.991).
The same PTH threshold also effectively predicts permanent hypoparathyroidism (AUC = 0.961).
Measuring PTH at 6 hours is more accurate than later calcium measurements for predicting hypocalcemia risk.
Abstract
PTH+ levels after thyroid surgery are generally used to detect patients at risk of developing postoperative hypoparathyroidism. However, there is still a lack of consensus about the threshold value regarding its evaluation, the definition of gland function recovery, and the classification of hypoparathyroidism as permanent. PTH levels (determined 6 hours after total thyroidectomy) could be effective for early prediction of the risk of postsurgical hypocalcemia and IV calcium requirements during hospitalization, comparing it with the predictive capacity of serum calcium levels at 24 and 48 hours after surgery. We also aim to study the efficacy of the measurement of PTH levels for the predictive diagnosis of permanent hypoparthyroidism. Prospective cohort study between September 2021 and November 2023. A public tertiary care hospital (Jaén, Spain). We collected data on 105 patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
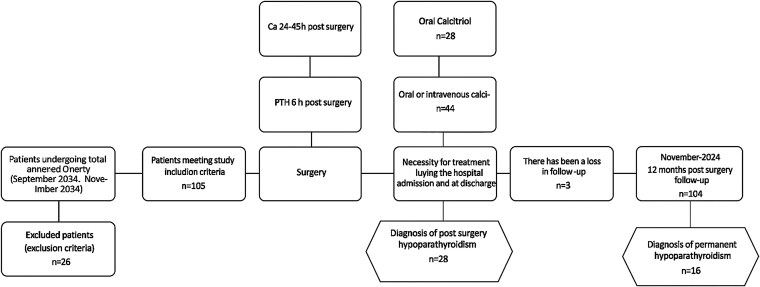 Figure 1
Figure 1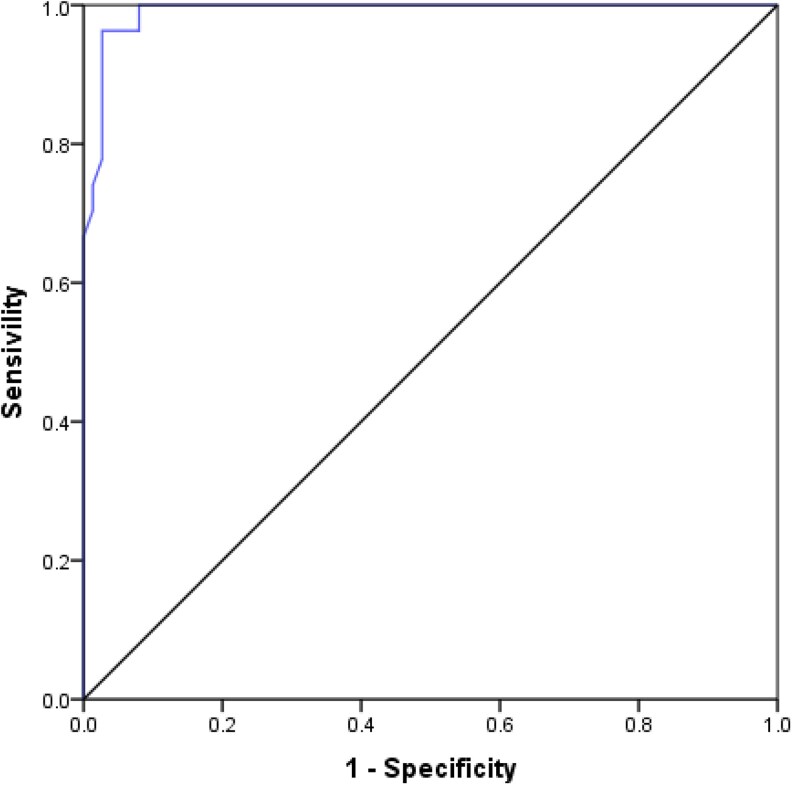 Figure 2
Figure 2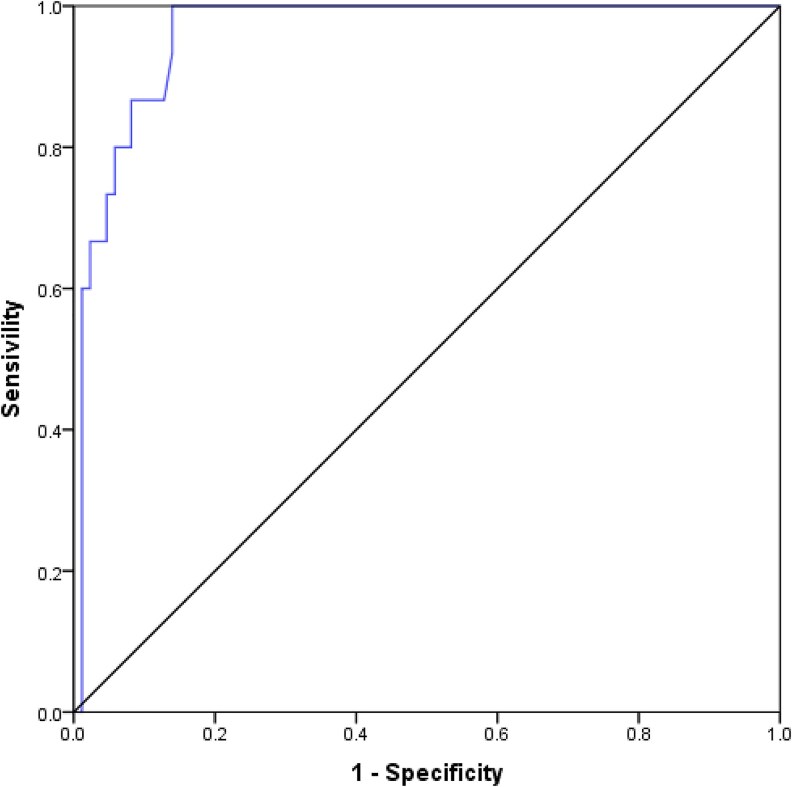 Figure 3
Figure 3| Total (105) | Female (84) | Male (21) |
| |
|---|---|---|---|---|
| Age (years), mean ± SD | 54.9 ± 14.9 | 53.4 ± 14.4 | 61.0 ± 15.9 |
|
| Cause of total thyroidectomy, n (%) | ||||
| Tumor | 53 (50.5) | 42 (50.0) | 11 (52.4) | .675 |
| Goiter | 46 (43.8) | 36 (42.9) | 10 (47.6) | |
| Graves’ disease | 6 (5.7) | 6 (7.1) | 0 (0.0) | |
| Type of surgery, n (%) | ||||
| Hemithyroidectomy to complete a previous one | 9 (8.6) | 9 (10.7) | 0 (0.0) | .199 |
| Total thyroidectomy | 96 (91.4) | 75 (89.3) | 21 (100.0) | |
| Central neck dissection, n (%) | ||||
| No | 78 (74.3) | 63 (75.0) | 15 (71.4) | .955 |
| Yes | 27 (25.7) | 21 (25.0) | 6 (28.6) | |
| Lateral neck dissection, n (%) | ||||
| No | 99 (94.3) | 79 (94.0) | 20 (95.2) | 1.000 |
| Yes | 6 (5.7) | 5 (6.0) | 1 (4.8) | |
| Parathyroid visualization, n (%) | ||||
| No | 17 (16.2) | 13 (15.5) | 4 (19.1) | .737 |
| Yes | 87 (82.9) | 71 (845) | 16 (76.2) | |
| Unknown | 1 (0.9) | 0 (0.0) | 1 (4.7) | |
| PTH 6 hours, mean ± SD | 31.7 ± 33.6 | 33.4 ± 35.9 | 25.0 ± 22.1 | .358 |
| PTH 6 hours at discharge, n (%) | ||||
| <10.10 | 28 (26.7) | 22 (26.2) | 6 (28.6) | 1.000 |
| =>10.10 | 74 (70.5) | 59 (70.2) | 15 (71.4) | |
| Unknown | 3 (2.8) | 3 (3.6) | 0 (0.0) | |
| Postoperative complications, n (%) | ||||
| No | 96 (91.5) | 75 (89.3) | 21 (100.0) | .354 |
| Yes | 8 (7.6) | 8 (9.5) | 0 (0.0) | |
| Unknown | 1 (0.9) | 1 (1.2) | 0 (0.0) | |
| Signs and symptoms of hypocalcemia, n (%) | ||||
| No | 89 (84.8) | 70 (83.3) | 19 (90.5) | .518 |
| Yes | 16 (15.2) | 14 (16.7) | 2 (9.5) | |
| Calcium presurgery, mean ± SD | 9.4 ± 0.6 | 9.5 ± 0.7 | 9.1 ± 0.3 | .371 |
| Calcium corrected 24 hours, mean ± SD | 8.9 ± 0.7 | 8.8 ± 0.7 | 9.0 ± 0.7 | .431 |
| Calcium corrected 48 hours, mean ± SD | 8.7 ± 0.8 | 8.7 ± 0.9 | 8.9 ± 0.7 | .303 |
| Calcium corrected at discharge, mean ± SD | 9.0 ± 0.7 | 9.0 ± 0.7 | 9.0 ± 0.6 | .688 |
| Oral calcium requirement, n (%) | ||||
| No | 74 (70.5) | 58 (69.0) | 16 (76.2) | .708 |
| Yes | 31 (29.5) | 26 (31.0) | 5 (23.8) | |
| Calcitriol requirement, n (%) | ||||
| No | 77 (73.3) | 61 (72.6) | 16 (76.2) | .956 |
| Yes | 28 (26.7) | 23 (27.4) | 5 (23.8) | |
| Intravenous calcium requirement, n (%) | ||||
| No | 92 (87.6) | 72 (85.7) | 20 (95.2) | .458 |
| Yes | 13 (12.4) | 12 (14.3) | 1 (4.8) | |
| Diagnosis of hypoparathyroidism at discharge, n (%) | ||||
| No | 77 (73.3) | 61 (72.6) | 16 (76.2) | .956 |
| Yes (with treatment) | 28 (26.7) | 23 (27.4) | 5 (23.8) | |
| Diagnosis permanent hypoparathyroidism (at 1 year), n (%) | ||||
| No | 64 (61.0) | 50 (59.5) | 14 (66.7) | .440 |
| Yes (with treatment) | 12 (11.4) | 11 (13.1) | 1 (4.8) | |
| Follow-up less than 1 year | 29 (27.6) | 23 (27.4) | 6 (28.5) | |
| Total (105) | |
|---|---|
| PTH 6 hours, mean ± SD | 31.7 ± 33.6 |
| PTH 6 hours, median [P25-P75] (R) | 23.1 [9.0-45.1] (235.5) |
| Presurgical calcium, mean ± SD | 9.4 ± 0.6 |
| Calcium corrected 24 hours, mean ± SD | 8.9 ± 0.7 |
| Calcium corrected 48 hours, mean ± SD | 8.7 ± 0.8 |
| Calcium corrected at discharge, mean ± SD | 9.0 ± 0.7 |
| Presurgical calcium, median [P25–P75] (R) | 9.2 [9.0-9.6] (2.4) |
| Calcium corrected 24 hours, median [P25–P75] (R) | 9.0 [8.4-9.4] (3.8) |
| Calcium corrected 48 hours, median [P25–P75] (R) | 8.6 [8.1-9.4] (3.9) |
| Calcium corrected at discharge, median [P25–P75] (R) | 9.0 [8.5-9.4] (3.5) |
| Univariate logistic regression | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | n | B | SE | Wald | Degrees of freedom |
| Odds ratio | 95% confidence interval for odds ratio | |
| Lower limit | Upper limit | ||||||||
| Sex (male) | 105 | −0.188 | 0.568 | 0.109 | 1 | .741 | 0.829 | 0.272 | 2.522 |
| Age (years) | 105 | −0.020 | 0.015 | 1.877 | 1 | .171 | 0.980 | 0.952 | 1.009 |
| Cause of total thyroidectomy | 105 | 2.080 | 2 | .353 | |||||
| Tumor | 53 | −0.057 | 0.915 | 0.004 | 1 | .950 | 0.944 | 0.157 | 5.672 |
| Goiter | 46 | −0.721 | 0.942 | 0.585 | 1 | .445 | 0.486 | 0.077 | 3.085 |
| Graves’ disease | 6 | Reference category | |||||||
| Central neck dissection | 105 | 1.131 | 0.478 | 5.599 | 1 | .018 | 3.100 | 1.214 | 7.913 |
| Lateral neck dissection | 105 | 0.339 | 0.896 | 0.143 | 1 | .705 | 1.404 | 0.243 | 8.122 |
| PTH 6 hours (pg/mL) | 102 | −0.886 | 0.309 | 8.227 | 1 | .004 | 0.412 | 0.225 | 0.755 |
| Multivariate logistic regression | |||||||||
| PTH 6 hours (pg/mL) | 98 | −0.885 | 0.309 | 8.183 | 1 | .004 | 0.413 | 0.225 | 0.757 |
| Univariate logistic regression | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | n | B | SE | Wald | Degrees of freedom |
| Odds ratio | 95% confidence interval for odds ratio | |
| Lower limit | Upper limit | ||||||||
| Sex (male) | 76 | −1.125 | 1.087 | 1.070 | 1 | .301 | 0.325 | 0.039 | 2.735 |
| Age (years) | 76 | −0.030 | 0.020 | 2.123 | 1 | .145 | 0.971 | 0.933 | 1.010 |
| Cause of total thyroidectomy | 76 | 0.888 | 2 | .641 | |||||
| Tumor | 39 | Due to the small sample size, statistics cannot be calculated. | |||||||
| Goiter | 33 | ||||||||
| Graves’ disease | 4 | Reference category | |||||||
| Central neck dissection | 76 | 1.520 | 0.656 | 5.376 | 1 | .020 | 4.573 | 1.265 | 16.533 |
| Lateral neck dissection | 76 | 1.036 | 1.268 | 0.668 | 1 | .414 | 2.818 | 0.235 | 33.809 |
| PTH 6 hours (pg/mL) | 73 | −0.477 | 0.169 | 7.941 | 1 | .005 | 0.620 | 0.445 | 0.865 |
| Multivariate logistic regression | |||||||||
| PTH 6 hours (pg/mL) | 70 | −0.477 | 0.170 | 7.933 | 1 | .005 | 0.620 | 0.445 | 0.865 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid and Parathyroid Surgery · Thyroid Cancer Diagnosis and Treatment · Parathyroid Disorders and Treatments
Hypocalcemia due to hypoparathyroidism is currently considered the most common complication of total thyroidectomy (1). The incidence varies depending on the definition of hypoparathyroidism, with an estimated prevalence of 30% in the immediate postsurgical period (2).
The etiologies include parathyroid gland injury, disruption of blood supply, or inadvertent parathyroid tissue resection. Postsurgical hypoparathyroidism is categorized as either transient or permanent, with the 12-month postoperative period being the most frequently used time marker to distinguish between these forms (3).
This condition holds significant clinical importance. Hypocalcemia can be associated with adverse health-related outcomes and increased healthcare costs, including IV treatment requirements, prolonged hospital stays, and a negative impact on patients’ quality of life (4). Permanent hypoparathyroidism requires lifelong calcium and vitamin D supplementation as well as continuous biochemical monitoring.
Postsurgical hypocalcemia has a delayed onset, typically emerging within 48 to 72 hours following surgery. Thus, serial serum calcium measurements and/or monitoring of hypocalcemic signs and symptoms for at least 72 hours postoperatively are essential for its detection.
To predict its early occurrence, various methods have been developed, including the postsurgery determination of PTH (1, 4, 5). However, neither the optimal timing of assessment nor the definitive PTH cutoff values, whether based on an isolated reading or as a percentage drop from presurgical values, have been clearly established (6-9). Currently, there is limited evidence regarding the utility of postoperative PTH as a predictor of long-term permanent hypoparathyroidism.
Therefore, the primary objective of this study is to assess whether the PTH level (determined 6 hours after total thyroidectomy) can accurately predict the risk of postsurgical hypocalcemia and the need for IV calcium treatment during hospitalization more effectively than calcium levels measured at 24 and 48 hours postsurgery.
The secondary objective is to evaluate the predictive capability of this early PTH measurement for diagnosing a well-defined 1-year mark of permanent hypoparathyroidism.
Material and Methods
This was a prospective cohort study of consecutive patients undergoing total thyroidectomy at the Hospital Universitario de Jaén (Spain) between September 2021 and November 2023. Patients were followed from the immediate postsurgical period up until 1 year after surgery.
Eligibility criteria included patients over 16 years of age undergoing first-time total thyroidectomy for multinodular goiter, Graves’ disease, or thyroid cancer, as well as those undergoing completion thyroidectomy following a previous hemithyroidectomy. Exclusion criteria included concomitant parathyroidectomy, a history of previous parathyroidectomy, preexisting parathyroid disorders, or subtotal thyroidectomy. The study was approved by our local ethics committee (CEI number: A01037777), in accordance with all applicable regulations. Informed consent was obtained from all participants.
We collected demographic variables such as age and sex, along with clinical variables traditionally associated with the risk of postthyroidectomy hypocalcemia, including the type of thyroidectomy, surgical indication, and extent of lymph node dissection. Postoperatively, serum PTH levels were measured at 6 hours (PTH6h) during the postanesthesia care unit stay. Following transfer to the hospital ward, daily clinical and laboratory monitoring was performed by the endocrinology department, including serum calcium corrected for total protein levels at 24 hours (Ca24h) and 48 hours (Ca48h) postsurgery to ensure normocalcemia.
Calcium supplementation requirements (oral or IV), both during hospitalization and at discharge, were documented. At 1-year follow-up, all patients underwent a comprehensive thyroid evaluation and laboratory testing, including serum PTH and calcium levels.
Calcium levels were determined by the colorimetric 5-nitro-5′-methyl-BAPTA method and intact PTH by electrochemiluminescent immunoassay. The manufacturer of the assays is Roche Diagnostics. PTH (6 hours postoperatively) and calcium levels (24-48 hours postoperatively) were measured in the same laboratory as appropriate. The reference values for calcemia were 8.6 to 10 mg/dL with a coefficient of variation of 3.05% and a lower limit of detection of 0.8 mg/dL; and for intact PTH they were 15 to 65.7 pg/mL, with a coefficient of variation of 3.05% and a lower limit of detection of 2.4 pg/mL.
A postsurgical hypoparathyroidism diagnosis was established based on corrected serum calcium levels under 8 mg/dL and if calcium treatment (oral or IV) was needed during hospital admission and at the time of discharge. Patients with hypocalcemia and elevated PTH were excluded from the study. IV calcium supplementation was deemed necessary if the patient exhibited severe tetany symptoms or if serum calcium levels were under 7.5 mg/dL without associated symptoms, following the protocol outlined in the consensus published by the Spanish Endocrine Society (5). Permanent hypoparathyroidism was defined as protein-corrected calcium below 8 mg/dL or PTH levels below 15 pg/mL while receiving calcium and calcitriol supplementation at the 12-month postsurgical evaluation. The standard treatment protocol at discharge consisted of calcitriol 0.25 to 0.5 mcg daily and oral calcium carbonate 1.25 g (1-6 tablets daily). Calcium citrate was considered as an alternative in cases of absorption difficulties or when high calcium carbonate requirements (>6 g/day) were needed.
Statistical analysis was performed using SPSS version 21. For the descriptive study, we utilized frequencies for qualitative variables and mean and SD for quantitative variables. Appropriate parametric or nonparametric tests (t-test, Mann-Whitney U test, chi-square test with Fisher's correction when applicable) were employed when comparing means or frequencies of groups. Additionally, group comparisons were evaluated by binary logistic regression analysis. A P-value <.05 was considered statistically significant.
To determine the combined effect of the variables on the diagnosis of transient or permanent hypoparathyroidism, a multivariate logistic regression model was developed using the forward method.
To select the predictors, binary logistic regressions were calculated to evaluate each of the independent variables. From the results of these individual regressions, those variables with a P-value of less than .05 were selected as candidate independent variables to be included in the multiple logistic regression study. It is usual to select variables with P-values less than .20 (10) but the criteria of Peduzzi (11) recommend using between 10 and 15 events per variable included in the model. For this reason, the number of independent variables was reduced by changing the criterion of P less than .20 to P less than .05.
To evaluate the quality of the obtained multivariate model, its prognostic capacity for the diagnosis of permanent hypoparathyroidism was assessed using the receiver operating characteristic curve and calculated area under the curve (AUC). Contingency tables were used to determine optimal cutoff values of PTH6h for maximum accuracy, sensitivity, and specificity in predicting both transient and permanent hypoparathyroidism.
Results
We collected data on 105 patients undergoing total thyroidectomy from September 2021. A total of 104 patients who completed the 12-month postsurgical follow-up protocol were evaluated for permanent hypoparathyroidism; we lost 1 patient's data due to death. Figure 1 shows these data in a flow chart. The study population had a mean age of 54.9 ± 14.9 years, comprising 84 females (80%) and 21 males (20%). Surgical indications included suspicion of carcinoma in 53 patients (50.5%), benign goiter in 46 patients (43.8%), and Graves’ disease in 6 patients (5.7%). Total thyroidectomy was performed in 91.4% (96 patients), while only 9 patients (8.6%) underwent completion thyroidectomy following previous hemithyroidectomy. Central neck dissection was performed in 27 patients and lateral neck dissection in 6 patients. Additional postsurgical complications were documented in 8 patients (7.6%). Baseline characteristics for all study subjects are presented in Table 1.
Flow diagram.
The mean presurgery serum calcium value was 9.4 ± 0.6 mg/dL (range 2.4). Postoperative calcium values varied according to measurement timing: 8.9 ± 0.7 mg/dL (range 3.8) at 24 hours, 8.7 ± 0.8 mg/dL (range 3.9) at 48 hours, and 9.0 ± 0.7 mg/dL (range 3.5) at discharge. These data are summarized in Table 2.
Postoperative hypoparathyroidism was diagnosed in 28 patients (26.7%). Significant differences were observed between patients who developed transient hypoparathyroidism and those who did not, specifically in calcium levels at 24 hours (Ca24h; 8.24 ± 0.57 mg/dL vs 9.09 ± 0.58 mg/dL; P < .001), calcium levels at 48 hours (Ca48h; 8.09 ± 0.90 mg/dL vs 9.03 ± 0.58 mg/dL; P < .001), PTH6h (5.64 ± 2.7 pg/mL vs 41.03 ± 34.63 pg/mL; P < .001), and the rate of central neck dissection (44.4% vs 20.5%; P = .023).
Permanent hypoparathyroidism was diagnosed in 16 patients (15.4%) among the 104 patients who completed annual follow-up. Similarly, when comparing patients who developed permanent hypoparathyroidism vs those who did not, statistically significant differences were found in Ca24h (8.32 ± 0.51 vs 8.97 ± 0.67; P < .001), Ca48h (8.26 ± 1.07 vs 8.84 ± 0.72, P = .015), PTH6h (4.92 ± 2.41 vs 36.67± 34.29; P < .001), and central neck dissection (25.9% vs 11.7%; P = .118).
To determine the diagnostic accuracy of postoperative levels of PTH6h and central neck dissection in predicting transient and permanent hypoparathyroidism, the multivariate model identified PTH6h as the sole significant predictor for both transient and permanent hypoparathyroidism (Tables 3 and 4).
Higher PTH6h levels demonstrated a protective effect against developing permanent hypoparathyroidism. For each unit increase in PTH6h, the risk of diagnosis decreases by 38.0% [odds ratio 0.62, 95% confidence interval (CI) 0.495-0.830], with this risk reduction being statistically significant (P = .001).
For transient hypoparathyroidism, the model correctly classified 99.1% of patients (AUC = 0.991, 95% CI 0.978-1.000). The optimal cutoff value for PTH6h that best discriminated between patients with and without transient hypoparathyroidism was determined to be 10.10 pg/mL. This threshold identified 99% of patients who developed hypocalcemia requiring IV calcium supplementation during hospitalization (Fig. 2).
Receiver operating characteristic curve of PTH 6 hours for transient hypoparathyroidism.
For permanent hypoparathyroidism, PTH6h demonstrated excellent discriminatory ability with an AUC of 0.961 (95% CI 0.925-0.997). The optimal PTH6h cutoff point for predicting permanent hypoparathyroidism was also determined to be 10.10 pg/mL. All patients with PTH6h values below this threshold were diagnosed with permanent hypoparathyroidism within 1 year of follow-up (Fig. 3).
Receiver operating characteristic of PTH 6 hours for permanent hypoparathyroidism.
Discussion
Hypoparathyroidism (transient and permanent) represents a highly prevalent complication that poses a significant clinical challenge for endocrinology units monitoring patients undergoing total thyroidectomy. Accurately predicting which patients may develop transient and/or permanent complications is crucial for optimizing patient management, reducing hospital stay duration, and minimizing healthcare costs associated with this procedure (9, 12-14).
Despite numerous research efforts addressing this issue, the optimal approach for identifying patients at risk of developing postsurgical hypoparathyroidism remains undefined.
Multiple studies have explored factors associated with complications following thyroid surgery, including patient characteristics (age, sex), gland pathology (enlargement, fibrosis, inflammation), surgical variables (extent of thyroidectomy, lymph node dissection) (15), procedural factors (surgical extensiveness, repeated interventions), and surgeon expertise (15, 16). Various predictors of immediate postthyroidectomy hypocalcemia have been identified, including single postoperative intact PTH values, percentage decrease of intact PTH from baseline, 25-hydroxyvitamin D levels, and underlying thyroid disorders such as Graves’ disease (17-19).
Some clinicians advocate prophylactic calcium supplementation for all postthyroidectomy patients, resulting in unnecessary treatment for approximately 70% of patients.
Postoperative PTH levels serve as excellent predictors of hypocalcemia. However, until recently, the percentage decrease in PTH levels after surgery has been the most commonly studied parameter, necessitating logistically challenging serial analytical determinations within short timeframes in the context of scheduled surgeries. The optimal timing for postsurgical PTH determination has not been clearly established when utilizing a single measurement approach (20-22).
Previous studies have examined PTH measurements at various intervals (0 hours, 4 hours, 12 hours, 24 hours) primarily for diagnosing rather than predicting hypoparathyroidism. Furthermore, standardized PTH cutoff points have not been established, and improved follow-up strategies for hypoparathyroidism classification as permanent, based on well-defined diagnostic criteria, are needed (7).
Monitoring PTH levels during patient follow-up should ideally predict parathyroid function recovery and guide decisions regarding discontinuation of replacement therapy. This requires a more precise diagnosis of permanent hypoparathyroidism (7, 18) and more accurate postsurgical PTH cutoff points than those determined in previous retrospective studies (5).
This study demonstrates that measuring a single PTH value at 6 hours postthyroidectomy—without requiring preoperative PTH baselines or calculating absolute/relative percentage decreases—provides superior predictive value for accurately defined hypoparathyroidism compared to corrected calcium values determined during the first 48 hours postsurgery. Additionally, this approach effectively identifies patients likely to require IV calcium supplementation during hospitalization. Early identification and treatment of hypocalcemia facilitate reduced hospital stays and appropriate discharge planning. To our knowledge, this represents the first prospective evaluation of PTH at 6 hours postthyroidectomy as a predictor of permanent parathyroid gland damage.
Our study has limitations, including a small sample size and challenges in standardizing PTH cutoff values as a single-center investigation. Center-specific cutoff values and establishing a precise timing for postoperative PTH determination that is applicable to clinical practice would likely be necessary for broader implementation. In conclusion, our findings introduce an easily reproducible preventive protocol based on a single PTH determination in the immediate postsurgical period, enabling more effective monitoring of patients at high risk for hypocalcemia while potentially reducing hospitalization duration and associated healthcare costs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Villarroya-Marquina I, Sancho J, Lorente-Poch L, Gallego-Otaegui L, Sitges-Serra A. Time to parathyroid function recovery in patients with protracted hypoparathyroidism after total thyroidectomy. Eur J Endocrinol. 2018;178(1):103‐111.29066572 10.1530/EJE-17-0589 · doi ↗ · pubmed ↗
- 2Mehanna HM, Jain A, Randeva H, Watkinson J, Shaha A. Postoperative hypocalcemia—the difference a definition makes. Head Neck. 2010;32(3):279‐283.19691027 10.1002/hed.21175 · doi ↗ · pubmed ↗
- 3Stack BC, Bimston DN, Bodenner DL, et al American Association of Clinical Endocrinologists and American College of endocrinology disease state clinical review: postoperative hypoparathyroidism—definitions and management. Endocr Pract. 2015;21(6):674‐685.26135962 10.4158/EP 14462.DSC · doi ↗ · pubmed ↗
- 4Samargandy S, Wadie J, Msallak H, et al Parathyroid hormone-driven algorithms after thyroid surgery: not one-size-fits-all. Head Neck. 2023;45(3):595‐603.36571430 10.1002/hed.27272 · doi ↗ · pubmed ↗
- 5Castro A, Oleaga A, Parente Arias P, Paja M, Gil Carcedo E, Álvarez Escolá C. Resumen ejecutivo del documento de consenso SEORL CCC-SEEN sobre hipoparatiroidismo postiroidectomía. Endocrinol Diabetes Nutr. 2019;66(7):459‐463.10.1016/j.endinu.2019.03.01531182347 · doi ↗ · pubmed ↗
- 6Khan AA, Bilezikian JP, Brandi ML, et al Evaluation and management of hypoparathyroidism summary statement and guidelines from the second international workshop. J Bone Miner Res. 2022;37(12):2568‐2585.36054621 10.1002/jbmr.4691 · doi ↗ · pubmed ↗
- 7Ritter K, Elfenbein D, Schneider DF, Chen H, Sippel RS. Hypoparathyroidism after total thyroidectomy: incidence and resolution. J Surg Res. 2015;197(2):348‐353.25982044 10.1016/j.jss.2015.04.059PMC 4466142 · doi ↗ · pubmed ↗
- 8Al-Dhahri SF, Mubasher M, Mufarji K, Allam OS, Terkawi AS. Factors predicting post-thyroidectomy hypoparathyroidism recovery. World J Surg. 2014;38(9):2304‐2310.24728582 10.1007/s 00268-014-2571-6 · doi ↗ · pubmed ↗