Age-dependent prognostic significance of neutrophil-to-HDL ratio in hepatocellular carcinoma patients
Qingjun Li, Ting Wang, Xiangjun Qian, Hang Xing, Zhongyi Li, Zhengzheng Wang, Shuaiya Ma, Bo Meng, Xianzhou Zhang, Feng Han, Hao Wang, Jinxue Zhou, Yongmei Li, Hao Zhuang

TL;DR
This study explores how the neutrophil-to-HDL ratio predicts outcomes in older patients with liver cancer, but not in younger ones.
Contribution
The study reveals that the neutrophil-to-HDL ratio has age-dependent prognostic value in hepatocellular carcinoma patients.
Findings
NHR and age were significant prognostic factors for HCC recurrence in the training cohort.
NHR's prognostic value was significant in older patients but not in younger ones.
ROC analysis showed moderate predictive performance for NHR and age.
Abstract
Hepatocellular carcinoma (HCC) is a highly heterogeneous malignancy, with variability in molecular features, clinical presentations, and treatment responses. Postoperative recurrence and disease-free survival (DFS) are important prognostic indicators for patient outcomes. The neutrophil-to-HDL ratio (NHR) is recognized as an inflammatory-lipid marker, however its age-dependent predictive value in HCC remains unclear and is not established in clinical practice. Therefore, we aimed to evaluate the prognostic significance of NHR in HCC patients undergoing surgical resection, with a focus on its age-dependent effects. We retrospectively analyzed 121 HCC patients undergoing surgical resection and randomly divided them into training (n = 95) and validation (n = 26) cohorts. Multivariate logistic regression, Receiver operating characteristic (ROC) analysis, and nomogram construction were used…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
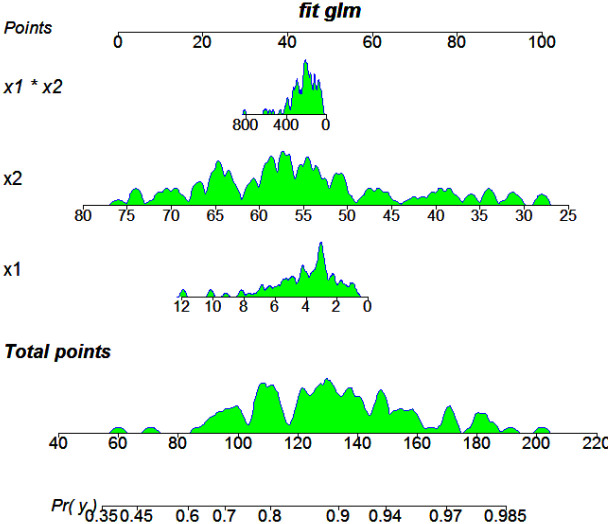 Figure 1
Figure 1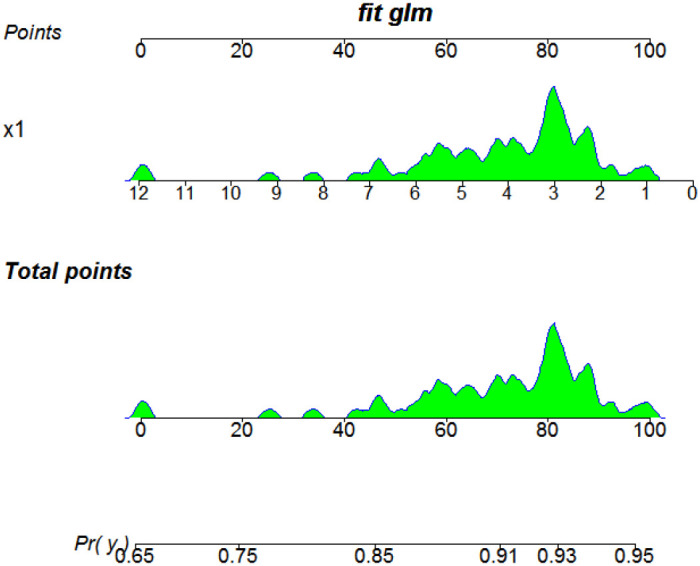 Figure 2
Figure 2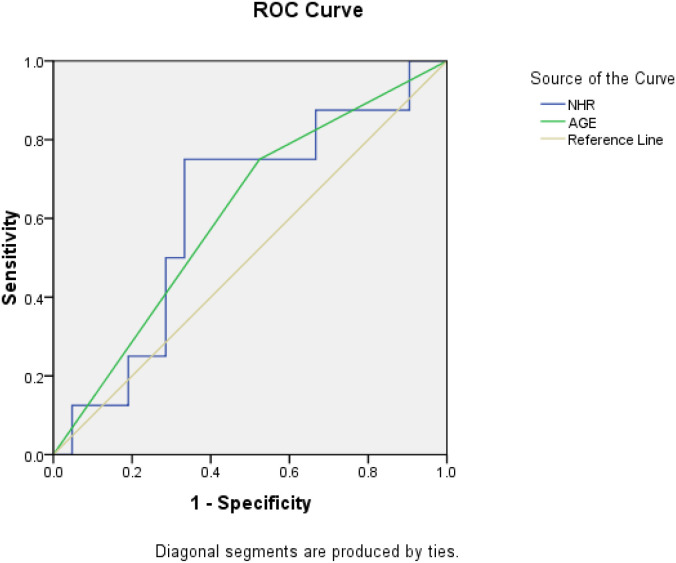 Figure 3
Figure 3| Variable | Better prognosis | Worse prognosis |
|
| ||
|---|---|---|---|---|---|---|
| Age | 0.200 | 57.50 ± 6.00 | 53.75 ± 11.54 | 1.391 | 0.242 | |
| Tumor differentiation | Lower | 11 | 27 | 0.142 | 0.110 | |
| higher | 2 | 32 | ||||
| Tumor number | <0.001 | 1.00 (1.00, 5.00) | 1.00 (1.00, 1.00) | -0.585 | 0.558 | |
| Operation duration (min) | 0.200 | 205.01 ± 101.22 | 184.62 ± 79.14 | 0.690 | 0.409 |
| Variable | Better prognosis | Worse prognosis |
|
| |
|---|---|---|---|---|---|
| WBC | 0.200 | 6.19 ± 1.76 | 6.45 ± 2.65 | 0.114 | 0.736 |
| Neutrophils | 0.200 | 3.88 ± 1.27 | 4.21 ± 2.17 | 0.297 | 0.587 |
| Lymphocyte | <0.001 | 1.96 (1.13, 2.61) | 1.65 (1.07, 2.18) | -1.222 | 0.222 |
| Platelet | 0.200 | 91.40 ± 24.43 | 88.72 ± 10.92 | 0.035 | 0.851 |
| PLR | 0.200 | 99.82 ± 16.35 | 117.89 ± 8.60 | 0.805 | 0.372 |
| NLR | 0.200 | 2.29 ± 0.37 | 3.07 ± 0.35 | 0.997 | 0.321 |
| PWR | 0.200 | 29.62 ± 3.60 | 29.59 ± 1.70 | 0.001 | 0.996 |
| TC | 0.200 | 3.05 ± 0.83 | 3.57 ± 0.92 | 2.086 | 0.153 |
| HDL-C | 0.200 | 0.79 ± 0.08 | 1.09 ± 0.23 | 11.402 |
|
| LDL-C | 0.200 | 1.97 ± 0.73 | 2.46 ± 0.76 | 2.563 | 0.114 |
| VLDL-C | <0.001 | 0.11 (0.02, 0.17) | 0.22 (0.17, 0.25) | -2.778 |
|
| LDL-HDL-Ratio | 0.200 | 2.51 ± 0.40 | 2.37 ± 0.13 | 0.118 | 0.732 |
| TC-HDL-Ratio | 0.200 | 3.88 ± 0.47 | 3.44 ± 0.16 | 0.744 | 0.391 |
| Non-HDL | 0.200 | 2.25 ± 0.32 | 2.51 ± 0.11 | 0.556 | 0.458 |
| RC | 0.200 | 0.28 ± 0.08 | 0.22 ± 0.02 | 0.995 | 0.323 |
| LHR | <0.001 | 2.45 (1.49, 3.06) | 1.41 (1.11, 2.05) | -1.825 | 0.068 |
| NHR | 0.200 | 5.26 ± 1.34 | 4.04 ± 2.16 | 2.115 | 0.150 |
| Variable |
|
|
|
| 95% |
|
|---|---|---|---|---|---|---|
| Age | 0.872 | 0.181 | 23.263 | 2.392 | 1.678- 3.410 | < 0.001 |
| Tumor differentiation | 1.875 | 0.812 | 5.331 | 6.519 | 1.328 - 32.007 | 0.021 |
| Tumor nnumber | -0.481 | 0.236 | 4.141 | 0.618 | 0.389 - 0.982 | 0.042 |
| HDL-C | 2.430 | 0.443 | 30.041 | 11.356 | 4.763 - 27.076 | < 0.001 |
| VLDL-C | 11.229 | 4.691 | 5.730 | 7.530 | 7.649 - 74.128 | 0.017 |
| NHR | -0.508 | 0.239 | 4.516 | 0.601 | 0.376 - 0.961 | 0.034 |
| Age | -0.150 | 0.063 | 5.730 | 0.861 | 0.761 - 0.973 | 0.017 |
| Variable | Younger patients | Older patients |
|
| |
|---|---|---|---|---|---|
| Male:female | 34:5 | 21:4 | 0.768 | 0.456 | |
| Tumor differentiation | Lower | 16 | 27 | 0.498 | 0.286 |
| higher | 17 | 20 | |||
| Tumor number | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.50) | -2.587 |
| |
| Operation duration (min) | 197.43 ± 97.66 | 186.18 ± 73.48 | 0.381 | 0.539 | |
| WBC | 6.66 ± 2.44 | 6.01 ± 2.51 | 1.498 | 0.224 | |
| Neturophils | 4.46 ± 2.28 | 3.96 ± 1.86 | 1.307 | 0.256 | |
| Lymphocyte | 2.05 (1.22, 2.28) | 1.58 (1.06, 1.94) | -2.125 |
| |
| Platelet | 204.33 ± 88.42 | 154.03 ± 82.62 | 7.565 |
| |
| PLR | 95.52 (53.13, 158.22) | 89.94 (70.90, 130.68) | -0.785 | 0.432 | |
| NLR | 1.89 (0.98, 4.53) | 2.56 (1.90, 3.07) | -0.651 | 0.515 | |
| PWR | 31.67 (20.45, 36.95) | 26.18 (19.85, 33.35) | -1.758 | 0.079 | |
| TC | 3.49 ± 0.64 | 3.58 ± 1.10 | 0.180 | 0.672 | |
| HDL-C | 1.09 ± 0.21 | 1.02 ± 0.24 | 1.593 | 0.211 | |
| LDL-C | 2.35 ± 0.57 | 2.49 ± 0.94 | 0.621 | 0.433 | |
| VLDL-C | 0.22 (0.08, 0.22) | 0.22 (0.18, 0.27) | -1.353 | 0.176 | |
| LDL-HDL-Ratio | 2.18 ± 0.40 | 2.60 ± 1.37 | 2.880 | 0.094 | |
| TC-HDL-Ratio | 3.26 ± 0.50 | 3.73 ± 1.63 | 2.536 | 0.115 | |
| Non-HDL | 2.41 ± 0.55 | 2.60 ± 1.07 | 0.923 | 0.340 | |
| RC | 0.12(0.12, 0.24) | 0.19 (0.12, 0.35) | -1.578 | 0.115 | |
| LHR | 2.05 (1.15, 2.56) | 1.36 (1.10, 1.97) | -0.892 | 0.373 | |
| NHR | 4.29 ± 2.33 | 4.16 ± 2.07 | 0.062 | 0.804 |
| Variable |
|
|
|
|
|
|
|---|---|---|---|---|---|---|
| Univariate regression analysis among younger patients | ||||||
| Tumor number | 1.922 | 0.532 | 13.060 | 6.833 | 2.410 - 19.375 | < 0.001 |
| HDL-C | 3.417 | 1.070 | 10.203 | 30.471 | 3.744 - 247.970 | 0.001 |
| LDL-C | 1.689 | 0.553 | 9.318 | 5.412 | 1.830 - 16.002 | 0.002 |
| VLDL-C | 30.369 | 14.401 | 4.447 | 15.451 | 8.524 - 28.012 | 0.035 |
| LDL-HDL ratio | 1.707 | 0.538 | 10.069 | 5.511 | 1.920 - 15.814 | 0.002 |
| Univariate regression analysis among older patients | ||||||
| Tumor number | -0.587 | 0.283 | 4.299 | 0.556 | 0.319 - 0.968 | 0.038 |
| HDL-C | 2.009 | 0.497 | 16.346 | 7.454 | 2.815 - 19.737 | < 0.001 |
| NHR | 0.294 | 0.096 | 9.275 | 1.341 | 1.110 - 1.621 | 0.002 |
| Multivariate regression analysis among older patients | ||||||
| NHR | -2.441 | 1.153 | 4.478 | 0.087 | 0.009 - 0.835 | 0.034 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Biomarkers in Disease Prognosis · Cancer, Lipids, and Metabolism · Hepatocellular Carcinoma Treatment and Prognosis
Introduction
Hepatocellular carcinoma (HCC) ranks as the sixth most prevalent cancer globally and is the third leading cause of cancer-related deaths (1–3). Despite advances in both surgical and systemic treatments, the prognosis of HCC remains poor due to its biological heterogeneity and high recurrence rates. Five-year survival rates vary widely, from approximately 70% for early-stage disease to less than 16% in advanced stages (4, 5). Accurate prognostic markers are crucial for guiding individualized treatment strategies and improving patient outcomes. Traditional prognostic factors, such as tumor size, stage, and differentiation, often fail to fully capture the complexity of HCC, highlighting the need for more comprehensive and accessible biomarkers to guide clinical decision-making and facilitate the development of individualized treatment strategies.
Systemic inflammation and lipid metabolism dysregulation in cancer progression. Individual markers of pro-inflammatory activity, such as neutrophil count (6, 7), and lipid parameters with anti-inflammatory properties, like high-density lipoprotein cholesterol (HDL-C) (8, 9), have been independently associated with tumor progression and survival. However, single markers may not fully capture the complex interplay between inflammation and lipid metabolism in cancer. The neutrophil-to-HDL ratio (NHR) integrates these two components, reflecting systemic inflammation and metabolic dysregulation more comprehensively than traditional single markers. NHR has demonstrated significant prognostic value across various fields as a biomarker of systemic inflammation and oxidative stress (10–12). NHR effectively predicts all-cause and cardiovascular mortality in the general population (10) and individuals with prediabetes (11). NHR is also reported as a prognostic cancer marker for HCC. Combining NHR with end-stage liver disease scores helps clinicians identify high-risk patients early, facilitating timely and optimized management strategies (12).
Age is a critical factor influencing cancer progression and prognosis through complex biological mechanisms (13–15). Older HCC patients experience immune senescence and lipid metabolism changes, such as impaired neutrophil function and decreased HDL-C levels (16, 17), which may amplify the prognostic relevance of inflammatory-lipid markers like NHR. These age-related changes also contribute to treatment effectiveness and inflammatory responses (13, 18). Consequently, understanding how age modifies the predictive value of NHR is essential for improving risk stratification in elderly HCC patients – a relationship that, to date, remains largely unexplored.
This study focuses on the novel role of the NHR as an age-stratified prognostic marker, aiming to address a critical gap in current models. By evaluating the prognostic value of NHR in HCC patients and exploring its potential age-specific effects, we aim to provide a foundation for more personalized and biologically informed therapeutic strategies.
Methods
A total of 121 HCC patients who underwent surgical resection at Henan Cancer Hospital, China between 2011 and 2012 were included. During this period, neoadjuvant and adjuvant therapies were not recommended by the Chinese liver cancer guidelines, and none of the patients received such treatment, ensuring therapeutic homogeneity within the cohort. Patients were classified as having a “better prognosis” if they remained disease-free for longer than the mean DFS of the cohort and/or had no recurrence at last follow-up. Those with recurrence and/or DFS less than or equal to the mean were classified as having a “worse prognosis”. Among the 121 patients, 95 were randomly assigned to the training dataset for the development the prognostic model, with the remaining 26 formed the validation dataset. Standardized postoperative follow-up (every 3 to 6 months) and consistent recurrence management protocols minimize treatment-related confounders, ensuring the reliability of the NHR analysis.
In the current analysis, tumor differentiation states were categorized according to the Barcelona Clinic Liver Cancer (BCLC) staging system, where lower tumor differentiation was defined as 0 to B stage cases, while higher stages represented others. Patients were stratified into younger and older groups based on the mean age (55.6 ± 8.7 years) of the whole cohort. The lipid-inflammatory profiles in this analysis included both original and derivative indicators. The original indicators comprised low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), total cholesterol (TC), very-low-density lipoprotein cholesterol (VLDL-C), neutrophils, lymphocytes, white blood cells (WBC), and platelets. The derivative indicators consisted of non-HDL, the LDL-to-HDL ratio, the TC-to-HDL ratio, RC (TC-HDL-LDL), and PWR (Platelet-to-WBC ratio). Additionally, the analysis included PLR (platelet-to-lymphocyte ratio), NLR (neutrophil-to-lymphocyte ratio), NHR (neutrophil-to-HDL ratio), and the lymphocyte-to-HDL ratio (LHR). Also, a cutoff of 55 years was used for age stratification in this manuscript, based on the mean age of our cohort (55.6 ± 8.7 years). This approach aligns with similar stratification methods in comparable HCC studies and offers balanced subgroups for our analysis.
Statistical analysis
Double entry was utilized to ensure the accuracy of the data. Normality was evaluated using the univariate and multivariate coefficients of skewness and kurtosis. The comparison of quantitative and categorical data was carried out using ANOVA and the Chi-square/Fisher’s exact test. Non-parametric analysis was applied to the data with a non-normal distribution. Logistic regression models were employed to establish the predictive model for HCC recurrence; subsequently, the nomogram was presented to detail the multivariate regression results and the interaction among predictive factors. To further evaluate the predictive performance of NHR and age as prognostic markers, receiver operating characteristic (ROC) analysis was performed. Considering the potential confounding effect of age, additional stratified analyses by age groups were conduct to assess the consistency of the association between NHR and postoperative recurrence across different age strata. A P-value of less than 0.05 was considered statistically significant. SPSS 16.0 statistical software and R 4.4.2 were utilized for data processing.
Results
General characteristics of the study population
The baseline characteristics of the 121 HCC patients are summarized in Table 1. The demographic and clinical variables distribution, including age, gender, tumor differentiation, tumor number, and operation duration, showed no significant differences between patients with better and worse prognoses (P > 0.05). Tumor differentiation and number were evenly distributed across prognosis groups, indicating a comparable baseline for further analysis.
Inflammatory-lipid profiles and prognosis
The inflammatory-lipid profiles of patients demonstrated significant differences between better and worse prognosis groups (Table 2). HDL-C levels were significantly lower in patients with worse prognoses (0.79 ± 0.08 mmol/L vs. 1.09 ± 0.23 mmol/L, P = 0.001), while VLDL-C levels were significantly higher in this group (0.22 [0.17–0.25] mmol/L vs. 0.11 [0.02–0.17] mmol/L, P = 0.005). Other markers, including NLR and PLR, showed no statistical significance (P > 0.05). Although NHR levels were higher in the worse prognosis group, they did not reach statistical significance in the overall cohort.
Establishment and validation of the prognosis predictive model
Multivariate logistic regression identified NHR and age as statistically significant prognostic variables in the training cohort (P < 0.05, Table 3). A decreasing NHR was significantly associated with a better prognosis (OR = 0.601, 95% CI: 0.376 - 0.961, P = 0.034), while increasing age was predictive of worse outcomes (OR = 0.861, 95% CI: 0.761 - 0.973, P = 0.017). Other variables retained statistical significance in univariate analyses but presented insignificant in the multivariate model.
Based on the regression results, we constructed a prognostic nomogram to visualize these variables’ predictive power, as shown in Figure 1. This model highlights the clinical applicability of integrating NHR and age into individualized prognostic assessments.
Results of multivariate regression for prognosis prediction among all patients. X1: NHR; X2: age.
Age-stratified analysis
To explore the age-dependent effects of NHR, the cohort was divided into two groups: younger patients (< 55 years) and older patients (≧ 55 years). The comparison of inflammatory-lipid profiles and other prognostic factors across these age groups is presented in Table 4. Older patients exhibited significantly higher tumor numbers (P = 0.010) and lower lymphocyte levels (P = 0.034). Platelet counts were also significantly reduced in older patients (P = 0.007), suggesting potential age-related differences in immune and inflammatory responses.
As shown in Figure 2; Table 5, in older patients, NHR demonstrated a strong association with prognosis (OR = 0.087, 95% CI: 0.009 - 0.835, P = 0.034), visualizing this subgroup’s multivariate regression results. In contrast, no significant relationship was observed between NHR and prognosis in younger patients (P > 0.05). Additionally, HDL-C and tumor number retained prognostic significance in older patients but not in the younger subgroup (Table 5). These findings suggest that NHR has better predictive value in older HCC patients, likely due to age-related changes in immune and metabolic responses.
Results of the multivariate regression for predicting prognosis in older patients. X1: NHR.
Model validation
The independent cohort (n = 26) validated the prognostic model. ROC analysis demonstrated that NHR and age were both effective predictors of prognosis, with area under the curve (AUC) values of 0.609 and 0.655, respectively (Figure 3).
ROC for NHR and Age in predicting prognosis among HCC patients.
Collectively, this study highlights NHR as an prognostic marker in HCC, with its predictive value being particularly pronounced in older patients. The nomogram integrating NHR and age provides a practical tool for individualized risk assessment. Additionally, the age-stratified analysis underscores the importance of considering demographic factors, such as age, when evaluating prognosis in HCC patients.
Discussion
This study demonstrated that the NHR is a significant prognostic factor in HCC patients, with its prognostic impact showing age-dependent effect. Specifically, patients with a DFS longer than the mean value of the current and/or no recurrence at the last follow-up were classified as having a better prognosis. Our findings suggest that integrating inflammatory-lipid markers into personalized prognostic models could improve HCC management. Specifically, NHR demonstrated age-dependent prognostic value, with stronger predictive power in older patients, likely due to age-related immune and metabolic changes. In older patients immune senescence, characterized by reduced adaptive immunity and heightened systemic inflammation (13, 14), may amplify the influence of inflammatory markers. Furthermore, age-related changes in lipid metabolism, such as decreased HDL-C levels, could enhance the prognostic relevance of NHR in this population. Notably, the nomogram incorporating NHR, age, and other clinical factors showed strong predictive accuracy and calibration, indicating its potential clinical utility. Compared to traditional inflammatory markers like NLR, NHR uniquely combines inflammatory and lipid components, providing a more comprehensive representation of systemic metabolic states relevant to HCC progression.
The NHR has emerged as a new biomarker reflecting the relationship between inflammation and lipid metabolism in cancer progression, with different age-dependent effects mediated through various molecular mechanisms. Literature suggests the inflammation-lipid crosstalk in aging, such as NHR, might integrate neutrophil-driven inflammation, including IL-6 and oxidative bursts, with HDL’s anti-inflammatory properties (e.g., cholesterol efflux, paraoxonase-1 activity), while aging disrupts this balance. HDL functionality declines while neutrophil activation increases, thus worsening inflammation (19–21). Additionally, metabolic dysregulation varies among age groups. HDL was found to suppress neutrophil extracellular traps (NETs) via apoA-I, maintaining vascular homeostasis in young populations, but HDL dysfunction (e.g., glycation in diabetes) fails to inhibit NETosis, increasing endothelial damage and thrombosis risk during aging (19–23).
Building on these findings, our results highlight the potential of NHR to address key gaps in current models by exploring its distinctive age-dependent effects. Most existing prognostic frameworks tend to generalize across populations, often neglecting the influence of age-specific factors (12, 15, 23–25). By highlighting the age-dependent prognostic relevance of NHR, our study underscores the necessity of incorporating demographic and biological factors, including age, into personalized prognostic assessments. This age-dependent insight not only refines risk stratification but also suggests that incorporating markers like NHR into prognostic models could enable more personalized and biologically informed treatment strategies, addressing the unmet clinical needs of diverse patient populations.
The clinical implications of this study are twofold. First, for older HCC patients, NHR might offer a readily available biomarker and cost-effective tool that can be easily integrated into routine clinical practice to enhance risk stratification, informing individualized follow-up and treatment strategies. Second, the age-dependent findings underscore the need for personalized approaches that account for demographic and biological heterogeneity in HCC patients. For example, interventions targeting neutrophil activation or promoting HDL-mediated lipid transport could improve outcomes, particularly in older patients with elevated NHR.
The NHR is an easily accessible clinical biomarker obtained from routine blood tests during standard patient care. Our current study focuses on validating NHR’s prognostic value due to its practical advantages in clinical workflows, which require no additional invasive procedures beyond standard blood test sampling. While platforms like OStme (26) and TIMER (27) enable analyses of tumor-infiltrating cells and immune cell infiltration patterns. We prioritized establishing NHR as a practical clinical marker first. Future studies could explore the mechanistic relationships between NHR and the tumor immune microenvironment using these bioinformatics tools, which may reveal deeper insights into how systemic inflammation and lipid metabolism interact with local immune responses in the tumor microenvironment.
Several limitations should be acknowledged. The relatively small sample size, particularly in the validation cohort, may limit the generalizability of our findings. This also contributed to the less-than-ideal AUC values in the current manuscript; however, the disconnect between ROC analysis and clinical utility often reveals hidden biological complexity or data flaws rather than algorithm failure. It is worth noting that despite the suboptimal AUC values, the model shows significant clinical relevance in the age-stratified analysis.
In summary, this study emphasizes the age-dependent prognostic value of NHR in HCC postoperative recurrence, providing a new perspective on the relationship between inflammation, lipid metabolism, and aging in cancer progression. Creating a validated prognostic nomogram that includes NHR offers a practical tool for personalized risk assessment, especially for elderly patients. By addressing the heterogeneity of HCC through an integrated biomarker and considering age-specific effects, this study underscores the importance of age-stratified methods in HCC prognosis. It proposes a strategy for future research on inflammatory lipid markers in cancer and their clinical applications aimed at enhancing patient outcomes in this challenging disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Llovet JM Montal R Sia D Finn RS . Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol. (2018) 15:599–616. doi: 10.1038/s 41571-018-0073-4, PMID: 30061739 PMC 12452113 · doi ↗ · pubmed ↗
- 2Jaffe A Taddei TH Giannini EG Ilagan-Ying YC Colombo M Strazzabosco M . Holistic management of hepatocellular carcinoma: the hepatologist’s comprehensive playbook. Liver Int. (2022) 42:2607–19. doi: 10.1111/liv.15432, PMID: 36161463 PMC 10878125 · doi ↗ · pubmed ↗
- 3Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660, PMID: 33538338 · doi ↗ · pubmed ↗
- 4Finn RS Qin S Ikeda M Galle PR Ducreux M Kim T . Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. (2020) 382:1894–905. doi: 10.1056/NEJ Moa 1915745, PMID: 32402160 · doi ↗ · pubmed ↗
- 5Kudo M Finn RS Qin S Han KH Ikeda K Piscaglia F . Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. (2018) 391:1163–73. doi: 10.1016/S 0140-6736(18)30207-1, PMID: 29433850 · doi ↗ · pubmed ↗
- 6Martín-Sierra C Martins R Coucelo M Abrantes AM Caetano Oliveira R Tralhão JG . Tumor resection in hepatic carcinomas restores circulating T regulatory cells. J Clin Med. (2024) 13:6011. doi: 10.3390/jcm 13196011, PMID: 39408071 PMC 11478317 · doi ↗ · pubmed ↗
- 7Zhang J Gu J Wang X Ji C Yu D Wang M . Engineering and targeting neutrophils for cancer therapy. Adv Mater. (2024) 36:e 2310318. doi: 10.1002/adma.202310318, PMID: 38320755 · doi ↗ · pubmed ↗
- 8Faubert B Solmonson A De Berardinis RJ . Metabolic reprogramming and cancer progression. Science. (2020) 368:eaaw 5473. doi: 10.1126/science.aaw 5473, PMID: 32273439 PMC 7227780 · doi ↗ · pubmed ↗