Monocyte IL-1β predicts adverse cardiovascular events and associates with coronary microvascular dysfunction in kidney transplant recipients
Zhengwei Yin, Qingyan Yang, Jianle Han, Junwei Yang, Tao Li, Jingjun Suo, Shuaiping Yang, Xiaobo Wang, Shuailin Zhao, Chang’an Wang

TL;DR
High levels of IL-1β in monocytes before kidney transplant predict higher risk of heart-related deaths and problems, possibly due to microvascular issues.
Contribution
This study identifies IL-1β as a novel independent predictor of cardiovascular outcomes in kidney transplant recipients.
Findings
Elevated pretransplant monocyte IL-1β expression independently predicts death and major adverse cardiovascular events in kidney transplant recipients.
IL-1β correlates with impaired coronary flow reserve and elevated syndecan-1, suggesting a link to coronary microvascular dysfunction.
Other pyroptosis-related genes showed weaker or nonsignificant associations with outcomes.
Abstract
Cardiovascular disease remains the leading cause of death after kidney transplantation. Coronary microvascular dysfunction (CMD) is common in kidney transplant recipients (KTRs), prognostically informative for cardiovascular events, and tightly related to inflammation. We aimed to test whether pretransplant monocytic expression of pyroptosis-related genes (IL-1β, GSDMD, Caspase-1, and NLRP3) independently predicts long-term mortality and major adverse cardiovascular events (MACE) in KTRs, and to evaluate its associations with CMD. We enrolled 305 KTRs. Monocytes were isolated preoperatively and qPCR quantified the four genes (normalized to GAPDH). MACE included death, myocardial infarction, stroke, and heart failure. Multivariable Cox regression was used to adjust for confounders associated with prognosis. CMD was evaluated using coronary flow reserve (CFR) in 41 KTRs and serum…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
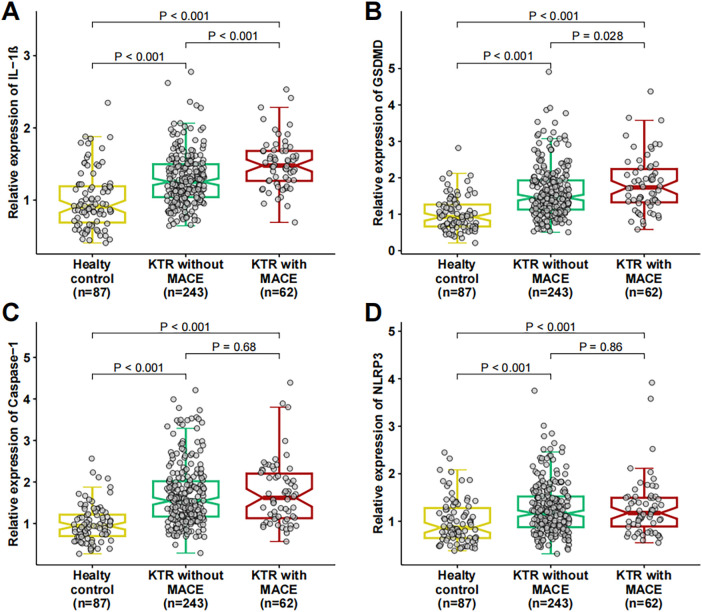 Figure 1
Figure 1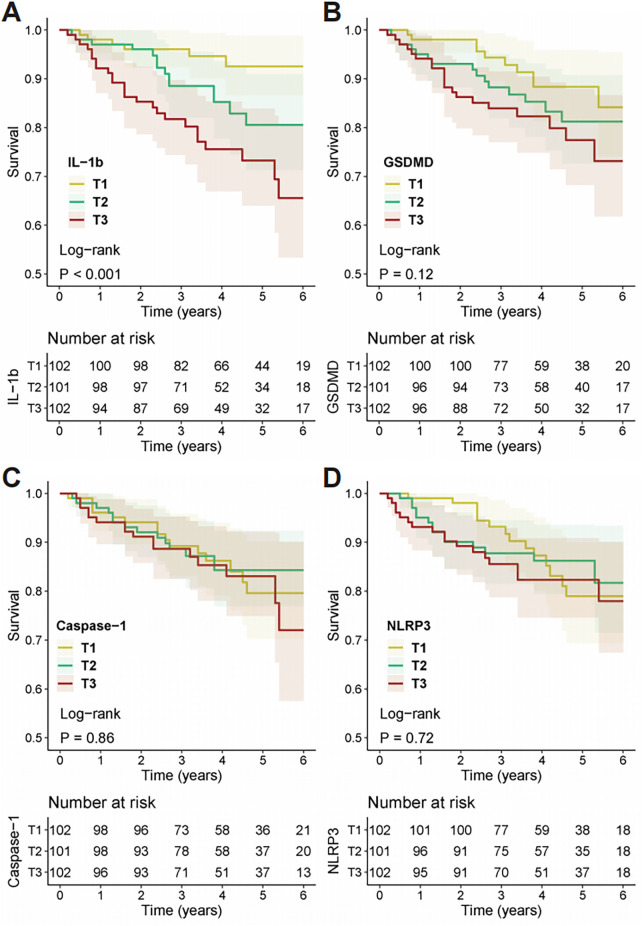 Figure 2
Figure 2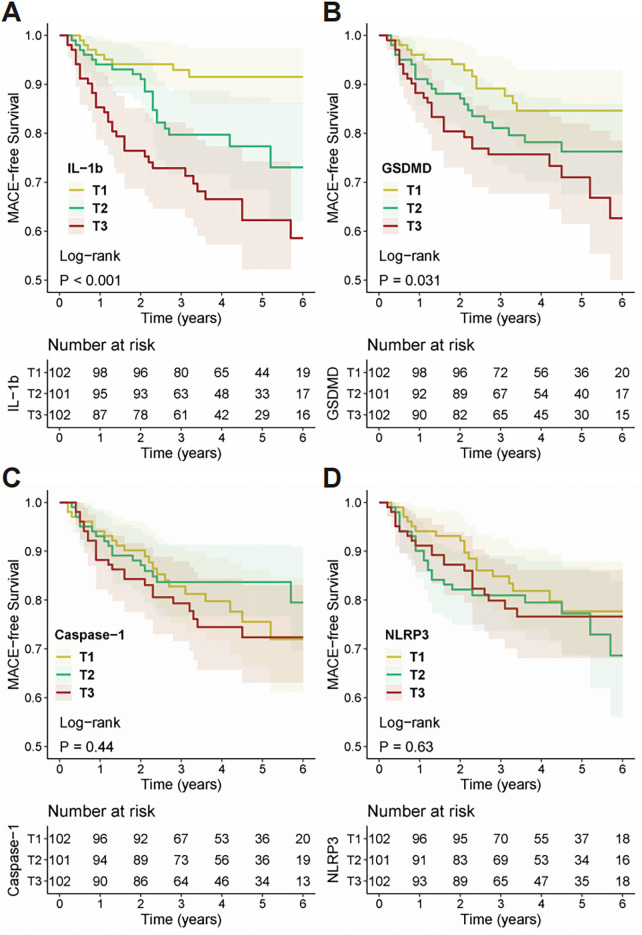 Figure 3
Figure 3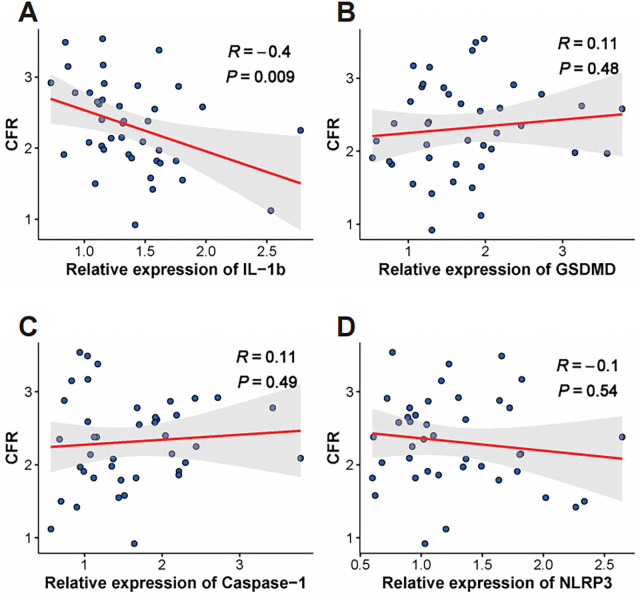 Figure 4
Figure 4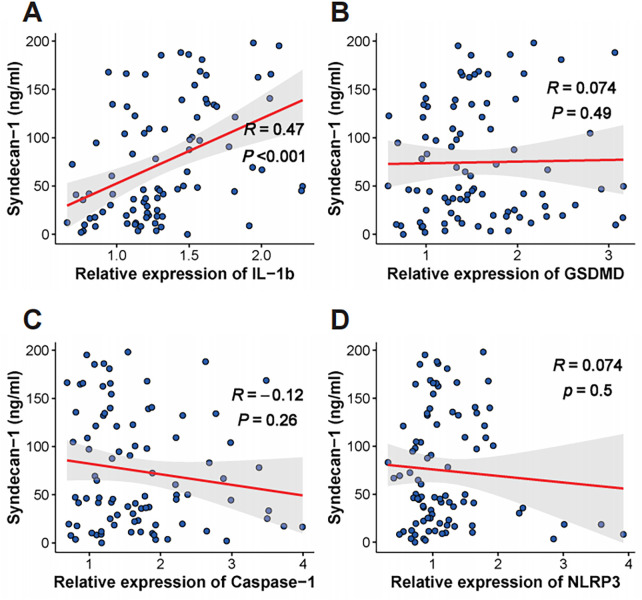 Figure 5
Figure 5| Variables | Healthy controls ( | Total KTR ( | KTR without MACE ( | KTR with MACE ( | ||
|---|---|---|---|---|---|---|
| Age, years | 46.7 ± 11.5 | 50.9 ± 11.7 | 0.003 | 49.84 (11.70) | 54.87 (10.95) | 0.002 |
| Female, | 30 (34.4) | 117 (38.4) | 0.51 | 98 (40.3) | 19 (30.6) | 0.21 |
| Diabetes, | 11 (12.6) | 70 (23.0) | 0.036 | 49 (20.2) | 21 (33.9) | 0.034 |
| Hypertension, | 16 (18.3) | 252 (82.6) | <0.001 | 196 (80.7) | 56 (90.3) | 0.109 |
| Current smoking, | 23 (26.4) | 94 (30.8) | 0.43 | 79 (32.5) | 15 (24.2) | 0.266 |
| First transplant, | – | 272 (89.2) | – | 219 (90.1) | 53 (85.5) | 0.412 |
| LDKT, | – | 40 (13.1) | – | 33 (13.6) | 7 (11.3) | 0.79 |
| Causes of ESKD, | ||||||
| Primary glomerulonephritis | 234 (76.7) | 183 (75.3) | 51 (82.3) | 0.592 | ||
| Diabetic nephropathy | 21 (6.9) | 16 (6.6) | 5 (8.1) | |||
| Polycystic kidney disease | 11 (3.6) | 10 (4.1) | 1 (1.6) | |||
| Lupus nephritis | 9 (3.0) | 8 (3.3) | 1 (1.6) | |||
| Allergic purpura nephritis | 7 (2.3) | 7 (2.9) | 0 (0.0) | |||
| Others | 23 (7.5) | 19 (7.8) | 4 (6.5) | |||
| Induction agent, | ||||||
| Thymoglobulin | 211 (69.2) | 169 (69.5) | 42 (67.7) | 0.963 | ||
| Basiliximab | 80 (26.2) | 63 (25.9) | 17 (27.4) | |||
| Others | 14 (4.6) | 11 (4.5) | 3 (4.8) | |||
| Cytomegalovirus serostatus, | ||||||
| D+/R- | 27 (8.9) | 22 (9.1) | 5 (8.1) | 0.155 | ||
| D+/R+ | 187 (61.3) | 145 (59.7) | 42 (67.7) | |||
| D-/R+ | 81 (26.6) | 70 (28.8) | 11 (17.7) | |||
| D-/R- | 10 (3.3) | 6 (2.5) | 4 (6.5) | |||
| Proteinuria, | ||||||
| Trace | 31 (10.2) | 25 (10.3) | 6 (9.7) | 0.253 | ||
| 1+ | 87 (28.5) | 65 (26.7) | 22 (35.5) | |||
| 2+ | 110 (36.1) | 95 (39.1) | 15 (24.2) | |||
| 3+ | 55 (18.0) | 41 (16.9) | 14 (22.6) | |||
| 4+ | 22 (7.2) | 17 (7.0) | 5 (8.1) | |||
| Dialysis vintage | – | 23.3 ± 10.2 | – | 23.2 ± 10.6 | 23.9 ± 8.5 | 0.619 |
| Previous CAD, | – | 59 (19.3) | – | 45 (18.5) | 14 (22.6) | 0.587 |
| Previous HF, | – | 48 (15.7) | – | 35 (14.4) | 13 (21.0) | 0.284 |
| IL-1b | 0.91 (0.69–1.19) | 1.29 (1.08–1.55) | <0.001 | 1.25 (1.04–1.50) | 1.48 (1.27–1.68) | <0.001 |
| GSDMD | 0.92 (0.66–1.27) | 1.50 (1.16–1.98) | <0.001 | 1.46 (1.13–1.93) | 1.74 (1.33–2.24) | 0.028 |
| Caspase-1 | 0.94 (0.70–1.21) | 1.55 (1.16–2.09) | <0.001 | 1.54 (1.17–2.02) | 1.62 (1.13–2.20) | 0.68 |
| NLRP3 | 0.87 (0.65–1.28) | 1.16 (0.88–1.52) | <0.001 | 1.16 (0.88–1.52) | 1.17 (0.89–1.49) | 0.863 |
| Events | Continuous | Unadjusted model | Adjusted model 1 | Adjusted model 2 | |||
|---|---|---|---|---|---|---|---|
| HR 95% CI | HR 95% CI | HR 95% CI | |||||
| Death | Per 1-SD | 1.579 (1.235–2.019) | <0.001 | 1.565 (1.211–2.023) | 0.001 | 1.530 (1.165–2.009) | 0.002 |
| MACE | Per 1-SD | 1.602 (1.301–1.973) | <0.001 | 1.597 (1.288–1.980) | <0.001 | 1.622 (1.283–2.052) | <0.001 |
| Events | Tertiles | Unadjusted model | Adjusted model 1 | Adjusted model 2 | |||
|---|---|---|---|---|---|---|---|
| HR 95% CI | HR 95% CI | HR 95% CI | |||||
| Death | T2 vs. T1 | 2.537 (0.975–6.604) | 0.056 | 2.239 (0.859–5.835) | 0.099 | 1.979 (0.750–5.224) | 0.168 |
| T3 vs. T1 | 4.740 (1.943–11.559) | 0.001 | 4.043 (1.656–9.874) | 0.002 | 3.771 (1.516–9.384) | 0.004 | |
| MACE | T2 vs. T1 | 2.755 (1.213–6.257) | 0.015 | 2.552 (1.122–5.802) | 0.025 | 2.411 (1.053–5.522) | 0.037 |
| T3 vs. T1 | 5.059 (2.341–10.933) | <0.001 | 4.563 (2.106–9.887) | <0.001 | 4.398 (2.003–9.654) | <0.001 | |
| Events | C-index (baseline model) | C-index (new model) | ΔC-index (95%CI) | |
|---|---|---|---|---|
| Death | 0.699 (0.622–0.776) | 0.731 (0.655–0.807) | 0.032 (0.010–0.055) | 0.008 |
| MACE | 0.674 (0.610–0.738) | 0.716 (0.655–0.777) | 0.042 (0.018–0.065) | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammasome and immune disorders · Pericarditis and Cardiac Tamponade · Cardiac Fibrosis and Remodeling
Introduction
1
Kidney transplantation (KT) is the optimal treatment for patients with end-stage kidney disease (ESKD), significantly improving both survival and quality of life (1, 2). Despite this, cardiovascular disease remains the leading cause of mortality in kidney transplant recipients (KTRs), with rates of major adverse cardiovascular events (MACE) far exceeding those in the general population (1–7). The elevated cardiovascular risk in KTRs is not fully explained by traditional risk factors alone, suggesting the involvement of other pathological mechanisms unique to the uremic and post-transplant environment (1).
Growing evidence implicates coronary microvascular dysfunction (CMD) as a key contributor to adverse cardiovascular outcomes (8–15). CMD, characterized by impaired coronary blood flow regulation in the absence of obstructive epicardial coronary artery disease (CAD) (8, 10), is highly prevalent among patients with chronic kidney disease and KTRs (16–20). Therefore, CMD may represent a crucial pathophysiological link to the heightened incidence of MACE observed after kidney transplantation.
Inflammation is a kye pathogenic driver of CMD (21–26). Pyroptosis, a highly pro-inflammatory form of regulated cell death, has recently emerged as a critical mechanism in the pathogenesis of various cardiovascular diseases (27, 28). This process is typically initiated by the activation of an inflammasome, such as the NLRP3 inflammasome, which leads to the activation of Caspase-1 (29–31). Active Caspase-1 then cleaves gasdermin D (GSDMD) to form pores in the cell membrane and processes pro-interleukin-1β (pro-IL-1β) into its mature, secreted form, thereby amplifying the inflammatory cascade (27–31). Monocytes and macrophages, key players in vascular inflammation, are primary effectors of the pyroptotic pathway (29).
However, it remains unknown whether the pyroptotic activity in peripheral blood monocytes prior to surgery can serve as a biomarker for future cardiovascular risk in KTRs. Therefore, the primary aim of this study was to investigate whether the preoperative expression levels of pyroptosis-related genes (IL-1β, GSDMD, Caspase-1, and NLRP3) in circulating monocytes are independent predictors of long-term MACE in KTRs. A secondary objective was to explore the association between the expression of these genes and the status of coronary microvascular function.
Materials and methods
2
Human subjects and sample collection
2.1
In this study, we recruited 305 KTRs between January 2018 and December 2022 at the Department of Kidney Transplantation and Nephrology Treatment Center, The Seventh People's Hospital of Zhengzhou. The exclusion criteria were: (1) severe liver impairment; (2) presence of severe, active infections; and (3) a history of MACE within the 2 weeks prior to hospital admission. All transplant recipients were consecutively recruited before the kidney transplant surgery, and all had already initiated maintenance dialysis at the time of enrollment. We also enrolled 87 healthy individuals without chronic kidney disease or known cardiovascular disease, who were undergoing routine health check-ups, to serve as a control group.
Peripheral blood samples were collected from all KTRs before the kidney transplant surgery. Monocytes were enriched from whole blood using the RosetteSep™ Human Monocyte Enrichment Cocktail (STEMCELL Technologies, Vancouver, Canada) according to the manufacturer's protocol. Serum was concurrently collected from peripheral blood by centrifugation and stored at −80°C until use.
Clinical data were collected preoperatively and included demographic characteristics, medical history, physical examination findings, and laboratory parameters.
The study protocol was approved by the ethical committee of The Seventh People's Hospital of Zhengzhou. All procedures were conducted in strict accordance with the latest version of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their inclusion in the study.
RNA isolation and real-time PCR
2.2
In this study, the expression levels of four pyroptosis-related genes (IL-1β, GSDMD, Caspase-1, and NLRP3) were evaluated using real-time PCR. Total RNA was extracted from enriched monocytes using Trizol® reagent (Invitrogen, Carlsbad, CA) following the manufacturer's instructions. RNA concentration and purity were assessed by measuring absorbance at 260 nm and 280 nm with a Nanodrop ND-3000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA). For each sample, 300 ng of total RNA was reverse transcribed into cDNA using a cDNA synthesis kit (Thermo Fisher Scientific). Real-time quantitative PCR (qPCR) was performed with TaqMan Gene Expression Assays (Applied Biosystems, Foster City, CA) on a StepOnePlus qPCR system (Applied Biosystems).
The following TaqMan probes were used: IL-1β (Hs01555410_m1), GSDMD (Hs00986748_g1), Caspase-1 (Hs00354836_m1), and NLRP3 (Hs00918082_m1). The expression of the four target genes was normalized to the housekeeping gene GAPDH (Hs02758991_g1). The relative expression of each gene was calculated using the 2-ΔΔCt method. Expression levels in KTRs were presented as a fold change relative to the mean expression level in the 87 healthy controls.
Endpoints
2.3
The primary endpoint was MACE, defined as a composite of all-cause mortality, nonfatal myocardial infarction, nonfatal stroke, or hospitalization due to heart failure (HF). Detailed definitions for each component of the endpoint are provided in Supplementary Table S1. After hospital discharge, patients were followed up at 1 month, 6 months, 1 year, and annually thereafter for up to 6 years, through clinic visits or telephone interviews.
Enzyme-linked immunosorbent assay (ELISA) of syndecan-1
2.4
The previous study have shown that circulating syndecan-1 levels reflect endothelial glycocalyx shedding and are associated with CMD (32). To assess whether monocytic gene expression relates to CMD, we measured serum syndecan-1 concentrations in 88 KTRs (enrolled from June 2021 to December 2022) using a commercial ELISA kit (Human Syndecan-1 ELISA Kit, Abcam, Cambridge, UK) according to the manufacturer's protocol.
Coronary flow reserve (CFR) measurement
2.5
To directly assess coronary microvascular function, we consecutively recruited KTRs for CFR assessment from August 2021 onwards. The main reasons for not completing analyzable CFR in some patients were (1) refusal to undergo the additional imaging and (2) technically inadequate Doppler signals despite acquisition attempts. After excluding examinations with inadequate image quality, a total of 41 KTRs remained for the CFR analysis.
As prevous reported (17, 18), following a baseline echocardiographic evaluation, dipyridamole was infused at a rate of 0.84 mg/kg over 6 min. CFR was calculated as the ratio of hyperemic to basal peak diastolic coronary flow velocity in the left anterior descending artery. Patients were instructed to abstain from methylxanthine-containing beverages for at least 24 h prior to the study.
Statistical analysis
2.6
Continuous variables were presented as mean ± standard deviation (SD) for normally distributed data or median with interquartile range (IQR) for non-normally distributed data. Comparisons between two groups were performed using the independent sample t-test or Mann–Whitney U-test. Categorical variables were expressed as frequencies (percentages) and compared using the chi-square test or Fisher's exact test.
For Kaplan–Meier survival analysis, KTRs were categorized into tertiles based on the expression level of each gene. Kaplan–Meier curves were generated to visualize time-to-first-event data, and differences were assessed with the log-rank test.
Univariate and multivariable Cox proportional-hazards regression models were used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs). The multivariable models were adjusted for potential confounders associated with prognosis, including age, sex, diabetes, hypertension, first kidney transplant, living donor kidney transplantation (LDKT), causes of ESKD (primary glomerulonephritis vs. others), cytomegalovirus serostatus [Donor (D) and Recipient (R): D+/R- D+/R+ vs. D-/R- D-/R+], proteinuria (trace/+/++ vs. +++/++++), dialysis vintage, and history of CAD or HF. Restricted cubic splines (RCS) regression models with four knots (two internal nodes) at the 0th, 35th, 65th, and 100th percentiles were used to assess potential nonlinear associations.
A baseline prognostic model was constructed using the aforementioned confounders. The incremental predictive value of adding IL-1β expression to the baseline model was assessed by comparing Harrell's concordance index (C-index) and calculating the change in C-index (ΔC-index) with 2000 bootstrap replications.
Spearman's correlation was used to analyze relationships between variables.
Multiple comparisons across the four pyroptosis-related genes were adjusted for using the Bonferroni method.
A two-sided P-value <0.05 was considered statistically significant. All analyses were performed using SPSS (Version 22.0, IBM Corp.) and R (Version 4.2.0, R Foundation for Statistical Computing).
Results
3
Baseline characteristics
3.1
The baseline clinical and demographic characteristics of the study population are presented in Table 1. Of the 305 KTRs, 62 (20.3%) experienced MACE during a median follow-up of 4 years (interquartile range: 2.4–5.0 years). Compared to KTRs without MACE, those who developed MACE were significantly older, had a higher prevalence of diabetes, and exhibited lower baseline eGFR (all P < 0.05). All other baseline characteristics were comparable between groups—including sex, hypertension, smoking, transplant-related factors, ESKD etiology, induction regimen, CMV serostatus, proteinuria, and prior CAD/HF (all P > 0.05).
Expression of the four pyroptosis-related genes
3.2
As shown in Figure 1 and Table 1, the expression levels of all four pyroptosis-related genes (IL-1β, GSDMD, Caspase-1, and NLRP3) were significantly elevated in KTRs (with or without MACE) compared to healthy controls (all P < 0.001). Among KTRs, the expression of IL-1β and GSDMD was significantly higher in patients who subsequently developed MACE compared to those who did not [IL-1β: 1.48 (1.27–1.68) vs. 1.25 (1.04–1.50), P < 0.001; GSDMD: 1.74 (1.33–2.24) vs. 1.46 (1.13–1.93), P = 0.028]. No significant differences were observed for Caspase-1 and NLRP3 expression between the KTR groups with and without MACE (P > 0.05).
Expression of pyroptosis-related genes in healthy controls and kidney transplant recipients. Boxplots showing the relative mRNA expression of (A) IL-1β, (B) GSDMD, (C) Caspase-1, and (D) NLRP3 in monocytes. Comparisons are made between healthy controls (n = 87), kidney transplant recipients (KTR) without major adverse cardiovascular events (MACE) (n = 243), and KTR with MACE (n = 62). The horizontal line within the box represents the median, the box boundaries represent the interquartile range, and whiskers extend to 1.5 times the interquartile range. P-values were calculated using the Mann–Whitney U-test.
After applying Bonferroni correction for multiple testing (significance threshold P < 0.0125 for the four genes), IL-1β expression remained significantly higher in KTRs with MACE than in those without MACE, whereas the difference in GSDMD expression between the two groups was no longer statistically significant.
Kaplan–Meier survival analyzing the prognostic significance of the four pyroptosis-related genes
3.3
Kaplan–Meier survival analysis was performed to assess the prognostic significance of the four genes. Based on tertiles of the relative expression for each gene, patients were divided into three groups—T1 (low), T2 (medium), and T3 (high). Kaplan–Meier survival curves (Figures 2, 3) revealed that KTRs with higher IL-1β expression levels had significantly worse clinical outcomes for both all-cause mortality (Log-rank test, P < 0.001) and MACE (Log-rank test, P < 0.001). In contrast, KTRs with higher GSDMD expression levels showed no significant difference in all-cause mortality (Log-rank test, P = 0.12), but had worse prognosis for MACE (Log-rank test, P = 0.031). Furthermore, there were no statistically significant differences in all-cause mortality or MACE outcomes for KTRs with varying levels of Caspase-1 (Death: Log-rank test, P = 0.86; MACE: Log-rank test, P = 0.44) or NLRP3 (Death: Log-rank test, P = 0.72; MACE: Log-rank test, P = 0.63) expression.
Kaplan–Meier analysis of all-cause mortality stratified by pyroptosis-related gene expression. Survival curves for all-cause mortality are shown for kidney transplant recipients categorized into tertiles (T1, T2, T3) based on the expression of (A) IL-1β, (B) GSDMD, (C) Caspase-1, and (D) NLRP3. Tertile 1 (T1) represents the lowest expression, and Tertile 3 (T3) represents the highest. P-values were determined using the log-rank test. The tables below each plot indicate the number of patients at risk in each tertile at specific time points.
Kaplan–meier analysis of MACE-free survival stratified by pyroptosis-related gene expression. Survival curves for MACE-free survival are shown for kidney transplant recipients categorized into tertiles (T1, T2, T3) based on the expression of (A) IL-1β, (B) GSDMD, (C) Caspase-1, and (D) NLRP3. Tertile 1 (T1) represents the lowest expression, and Tertile 3 (T3) represents the highest. P-values were determined using the log-rank test. The tables below each plot indicate the number of patients at risk in each tertile at specific time points.
IL-1β as an independent predictor for outcomes in KTRs
3.4
Kaplan–Meier survival curves indicated that different expression levels of IL-1β could predict the prognosis of KTRs. We further used multivariable Cox regression models to adjust for potential confounders associated with prognosis. IL-1β expression was included in the Cox models either as a continuous variable (per standard deviation increase) or as a categorical variable defined by tertiles (T1, T2, T3). The adjusted Model 1 controlled for age and sex, while model 2 was further adjusted for diabetes, hypertension, first kidney transplant, LDKT, causes of ESKD, cytomegalovirus serostatus, proteinuria, eGFR, dialysis vintage, and history of CAD or HF.
When IL-1β expression was treated as a continuous variable in the Cox regression model, higher levels of IL-1β were significantly associated with both all-cause mortality (Table 2: Per-SD: Unadjusted Model: HR = 1.579, 95% CI = 1.235–2.019, P < 0.001; Adjusted Model 1: HR = 1.565, 95% CI = 1.211–2.023, P = 0.001; Adjusted Model 2: HR = 1.530, 95% CI = 1.165–2.009, P = 0.002) and MACE (Per-SD: Unadjusted Model: HR = 1.602, 95% CI = 1.301–1.973, P < 0.001; Adjusted Model 1: HR = 1.597, 95% CI = 1.288–1.980, P < 0.001; Adjusted Model 2: HR = 1.622, 95% CI = 1.283–2.052, P < 0.001).
When IL-1β expression was modeled categorically by tertiles in the Cox regression model, KTRs with the highest IL-1β expression (T3) compared to those with the lowest expression (T1) had significantly worse outcomes for both all-cause mortality (Table 3: T3 vs. T1: Unadjusted Model: HR = 4.740, 95% CI = 1.943–11.559, P = 0.001; Adjusted Model 1: HR = 4.043, 95% CI = 1.656–9.874 P = 0.002; Adjusted Model 2: HR = 3.771, 95% CI = 1.516–9.384, P = 0.004) and MACE (T3 vs. T1: Unadjusted Model: HR = 5.059, 95% CI = 2.341–10.933, P < 0.001; Adjusted Model 1: HR = 4.563, 95% CI = 2.106–9.887, P < 0.001; Adjusted Model 2: HR = 4.398, 95% CI = 2.003–9.654, P < 0.001).
RCS analysis showed a generally linear association between IL-1β levels and the risk of death and MACE, with no significant evidence of nonlinearity (P for nonlinear = 0.29 and 0.0986, respectively; Supplementary Figure S1).
Furthermore, adding IL-1β expression to the baseline model comprising potential confounders significantly improved the predictive accuracy for both death (C-index increased from 0.699 to 0.731, ΔC-index: 0.032, P = 0.008) and MACE (C-index increased from 0.674 to 0.716, ΔC-index: 0.042, P < 0.001) (Table 4).
Association of IL-1β with coronary microvascular dysfunction
3.5
Given that CMD markedly increases the risk of MACE in KTRs (16), we hypothesized that higher monocytic IL-1β expression contributes to MACE by promoting CMD. Accordingly, we assessed associations between IL-1β expression and two indices that reflect CMD severity—CFR and serum syndecan-1. In 41 KTRs, monocytic IL-1β expression was the only gene to show a significant negative correlation with CFR (R = −0.4, P = 0.009; Figure 4A). In 88 KTRs, IL-1β expression demonstrated a strong positive correlation with serum syndecan-1 levels (R = 0.47, P < 0.001; Figure 5A). The other pyroptosis-related genes showed no significant correlation with either CFR or syndecan-1.
Correlation between pyroptosis gene expression and coronary flow reserve. Scatter plots illustrating the relationship between coronary flow reserve (CFR) and the relative expression of (A) IL-1β, (B) GSDMD, (C) Caspase-1, and (D) NLRP3 in kidney transplant recipients (n = 41). The red line represents the linear regression fit, and the gray shaded area indicates the 95% confidence interval. Pearson's correlation coefficient (R) and the corresponding p-value are displayed for each analysis.
Relationship between pyroptosis gene expression and the endothelial injury marker syndecan-1. Scatter plots show the correlation between serum Syndecan-1 concentration (ng/ml) and the relative mRNA expression of (A) IL-1β, (B) GSDMD, (C) Caspase-1, and (D) NLRP3. The red line indicates the linear regression line, and the shaded gray area represents the 95% confidence interval. Pearson's correlation coefficient (R) and the associated p-value are provided for each plot.
Discussion
4
In this cohort study, we identified that elevated monocytic expression of IL-1β is a powerful and independent predictor of both MACE and all-cause mortality. This association remained robust after adjusting for a comprehensive set of traditional cardiovascular and transplant-related risk factors. Furthermore, we demonstrated a significant correlation between IL-1β levels, markers of endothelial injury, and impaired coronary microvascular function, providing novel mechanistic insights into the pathophysiology of cardiovascular disease in this vulnerable population.
The principal finding of this study is the clinical utility of IL-1β as a prognostic biomarker in KTRs. Cardiovascular disease is the leading cause of death in KTRs (1, 2), yet conventional risk stratification models often fall short (4, 5, 7). Our data show that IL-1β provides incremental prognostic value beyond established risk factors, as evidenced by the significant improvement in the C-index for predicting both MACE and death. The continuous and graded relationship between IL-1β levels and adverse outcomes, as shown in our Cox and restricted cubic spline analyses, suggests that IL-1β could be used to identify high-risk individuals who may benefit from more intensive surveillance, aggressive risk factor management, or targeted anti-inflammatory therapies.
Several potential mechanisms may explain the strong association between elevated IL-1β and poor cardiovascular outcomes in KTRs. Our findings suggest a central role for monocyte-mediated pyroptosis, an inflammatory form of programmed cell death (29). We observed significantly higher expression of not only IL-1β but also GSDMD, the key executioner of pyroptosis (31), in KTRs, particularly in those who developed MACE. This process culminates in the release of potent inflammatory cytokines, including mature IL-1β, which drives a systemic inflammatory state (27–31). This inflammation, in turn, likely contributes to cardiovascular pathology through two interconnected pathways. First, we identified a strong positive correlation between IL-1β and Syndecan-1, a marker of endothelial glycocalyx shedding and injury. Chronic endothelial damage is a foundational step in the development of atherosclerosis and vascular dysfunction. Second, and perhaps most importantly, we provide direct evidence linking IL-1β to CMD. The significant negative correlation between IL-1β expression and CFR suggests that the inflammatory milieu driven by IL-1β impairs the function of the coronary microvasculature, leading to myocardial ischemia and contributing to the heightened risk of MACE.
We acknowledge several limitations in our study. First, as a single-center, observational study, our findings may have limited generalizability and cannot establish causality. The associations observed require validation in larger, multi-center cohorts. Second, although we adjusted for numerous potential confounders, residual confounding cannot be entirely excluded. Third, the gene expression was measured at a single time point, which may not fully capture the dynamic nature of the inflammatory state over the long-term follow-up period. Finally, while our data strongly suggest a link between IL-1β and CMD, we did not directly assess the impact of IL-1β-targeted therapies on coronary microvascular function.
In conclusion, this study establishes monocytic IL-1β expression as a robust, independent predictor of MACE and mortality in KTRs, an association that may be mediated by more severe CMD among patients with higher IL-1β levels.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anderson B Qasim M Evison F Gallier S Townend JN Ferro CJ A population cohort analysis of English transplant centers indicates major adverse cardiovascular events after kidney transplantation. Kidney Int. (2022) 102(4):876–84. 10.1016/j.kint.2022.05.01735716956 · doi ↗ · pubmed ↗
- 2Helve S Helantera I Laine M Nieminen T Finne P Helve J. Trends and specific causes of cardiovascular mortality after kidney transplantation in Finland. Clin J Am Soc Nephrol. (2024) 19(3):355–63. 10.2215/CJN.000000000000036037962909 PMC 10937022 · doi ↗ · pubmed ↗
- 3Emrich IE Scheuer AL Rogacev KS Mahfoud F Wagenpfeil S Fliser D Plasma biomarkers outperform echocardiographic measurements for cardiovascular risk prediction in kidney transplant recipients: results of the HOME ALONE study. Clin Kidney J. (2022) 15(4):693–702. 10.1093/ckj/sfab 21635371467 PMC 8967667 · doi ↗ · pubmed ↗
- 4Colladant M Chabannes M Crepin T Bamoulid J Courivaud C Ducloux D. Triglyceride-glucose index and cardiovascular events in kidney transplant recipients. Kidney Int Rep. (2023) 8(11):2307–14. 10.1016/j.ekir.2023.08.02138025208 PMC 10658270 · doi ↗ · pubmed ↗
- 5Bussalino E Picciotto D Maccio L Parodi A Gandolfo MT Viazzi F. Visit-to-visit systolic blood pressure variability independently predicts cardiovascular events in a kidney transplant recipients’ cohort. J Am Heart Assoc. (2024) 13(15):e 034108. 10.1161/JAHA.124.03410839011950 PMC 11964048 · doi ↗ · pubmed ↗
- 6Huck DM Weber B Schreiber B Pandav J Parks S Hainer J Comparative effectiveness of PET and SPECT MPI for predicting cardiovascular events after kidney transplant. Circ Cardiovasc Imaging. (2024) 17(1):e 015858. 10.1161/CIRCIMAGING.123.01585838227694 PMC 10794031 · doi ↗ · pubmed ↗
- 7Rajnochova Bloudickova S Janek B Machackova K Hruba P. Standardized risk-stratified cardiac assessment and early post-transplant cardiovascular complications in kidney transplant recipients. Front Cardiovasc Med. (2024) 11:1322176. 10.3389/fcvm.2024.132217638327495 PMC 10847279 · doi ↗ · pubmed ↗
- 8Taqueti VR Di Carli MF. Coronary microvascular disease pathogenic mechanisms and therapeutic options: JACC state-of-the-art review. J Am Coll Cardiol. (2018) 72(21):2625–41. 10.1016/j.jacc.2018.09.04230466521 PMC 6296779 · doi ↗ · pubmed ↗