A novel effect of bevacizumab in reducing characteristic pigmentation in Peutz–Jeghers syndrome: a case report and literature review
Delu Wu, Xinyue Liu, Song Wang, Huanyu Zhang, Guofeng Qu, Lina Wang

TL;DR
A patient with Peutz–Jeghers syndrome showed reduced pigmentation and cancer remission after bevacizumab treatment, suggesting a new therapeutic approach.
Contribution
Demonstrates bevacizumab's novel effect on both cancer and pigmentation in Peutz–Jeghers syndrome.
Findings
Bevacizumab therapy led to complete remission of PJS-associated adenocarcinoma.
Perioral melanotic macules progressively faded during bevacizumab treatment.
VEGF inhibition may concurrently affect carcinogenesis and melanin deposition in PJS.
Abstract
Peutz–Jeghers syndrome (PJS) is a rare autosomal dominant disorder characterized by mucocutaneous pigmentation (e.g., perioral melanotic macules) and gastrointestinal hamartomatous polyps, with heightened cancer susceptibility. This report describes a 34-year-old Han Chinese ethnicity woman with familial Peutz–Jeghers syndrome (PJS) and stage IIA HPV-independent gastric-type endocervical adenocarcinoma following bevacizumab therapy. Initial concurrent chemoradiation (paclitaxel with either nedaplatin or cisplatin with volumetric modulated arc therapy) achieved partial response, while subsequent maintenance therapy combining bevacizumab with chemotherapy induced complete radiographic remission. Crucially, progressive fading of pathognomonic perioral melanotic macules demonstrated temporal correlation with bevacizumab administration, with sustained remission at 1-year follow-up. These…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
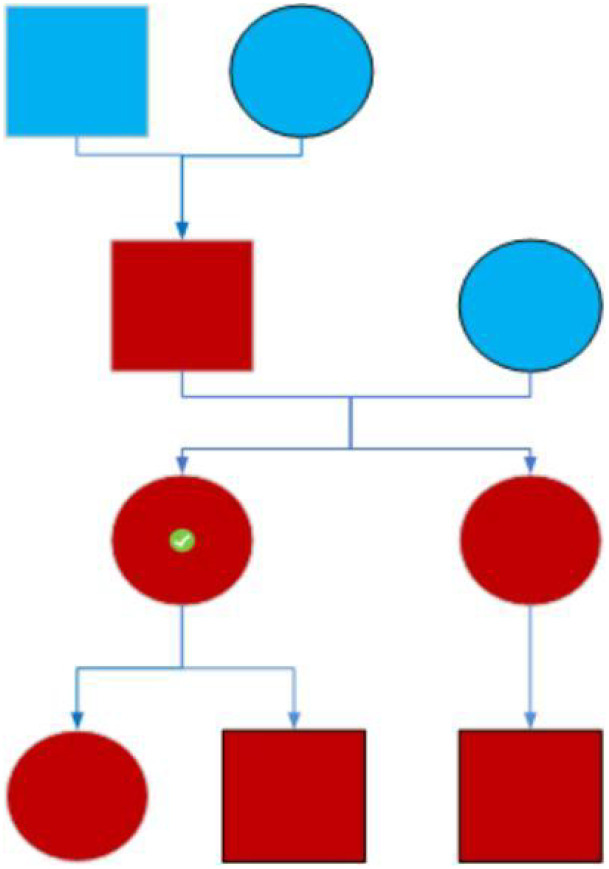 Figure 1
Figure 1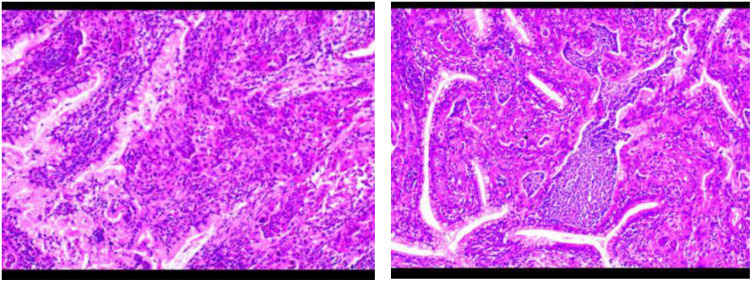 Figure 2
Figure 2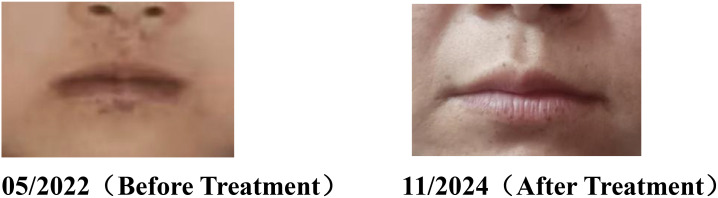 Figure 3
Figure 3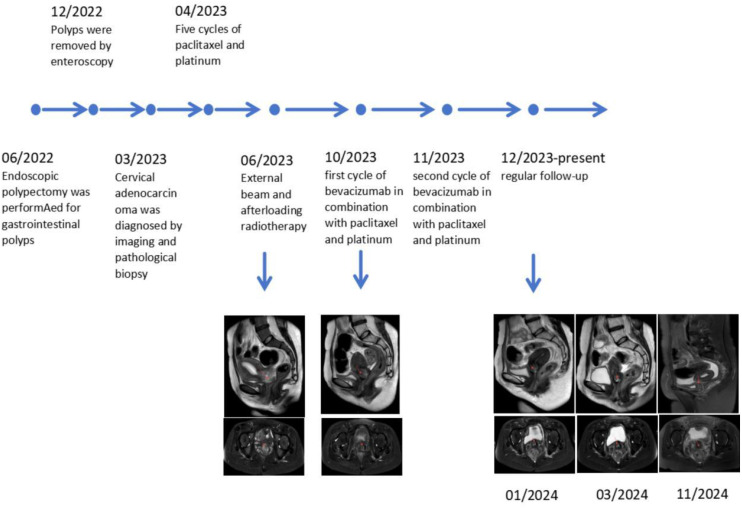 Figure 4
Figure 4| Pathogenic pathway | Mechanistic basis | Potential targets/drugs | References |
|---|---|---|---|
| AMPK/mTOR pathway | STK11/LKB1 inactivation reduces AMPK activity, leading to mTOR hyperactivation and tumorigenesis | AMPK activators (metformin), mTOR inhibitors (rapamycin) | ( |
| Cell polarity regulation | LKB1 loss disrupts PAR-4/MARK kinase-mediated polarity, inducing structural chaos and carcinogenesis | PAR-4/MARK pathway modulators | ( |
| HIF-1α pathway | LKB1 deficiency stabilizes HIF-1α, enhancing angiogenesis and tumor microenvironment adaptation | HIF-1α inhibitors (bevacizumab) | ( |
| MAPK/KRAS pathway | Co-activation of KRAS and MAPK signaling driven by STK11/LKB1 mutations | MEK inhibitors (trametinib) | ( |
| Wnt/β-catenin pathway | Aberrant Wnt activation with β-catenin accumulation in polyps due to LKB1 deficiency | Wnt inhibitors (PORCN inhibitors) | ( |
| Case no. | Age | PJS features (polyps/pigmentation) | GAS diagnostic methods | FIGO stage (2018) | Treatment modalities | Outcome | Reference | Publication year |
|---|---|---|---|---|---|---|---|---|
| 1 | 32 | Intestinal polyps, perioral pigmentation | Cervical biopsy + MRI | IB3 | NACT + RH + ACT | Unknown | ( | 2023 |
| 2 | 39 | Intestinal polyps, perioral/periocular/acral pigmentation | Cervical biopsy + MRI | IB3 | RH + CCRT | NED at 1-year follow-up | ( | 2021 |
| 3 | 32 | Unknown | Abdominal CT + IHC | IV | RH + TP + bevacizumab | Died at 1 year (multiple metastases) | ( | 2023 |
| 4 | 31 | Intestinal polyps, perioral/acral pigmentation | Pelvic MRI + cone biopsy + IHC | IB2 | RH + paclitaxel/oxaliplatin (4 cycles) | NED at 5-year follow-up | ( | 2023 |
| 5 | 45 | Gastrointestinal polyps, perioral/periocular pigmentation | Pelvic MRI + histopathology | IIIC | RH + docetaxel/carboplatin + bevacizumab | CR, NED at 15-month follow-up | ( | 2021 |
| 6 | 36 | Small bowel polyps | Pelvic MRI + cone biopsy + histopathology | IB2 | RH + CCRT (details unknown) | Unknown | ( | 2019 |
| 7 | 24 | Intestinal polyps, perioral pigmentation | Pelvic MRI + IHC | IIIA | RH + adjuvant RT | NED at 12-month follow-up | ( | 2019 |
| 8 | 24 | Intestinal polyps, lip/buccal mucosa/acral pigmentation | Pelvic MRI + IHC | Unknown | Unknown | Unknown | ( | 2024 |
| 9 | 32 | Small bowel polyps, lip/digital mucocutaneous pigmentation | Pelvic MRI + IHC | Unknown | Total hysterectomy | Unknown | ( | 2015 |
| 10 | 38 | Unknown | Pelvic MRI + histopathology | Unknown | RH + carboplatin (6 cycles) | NED at 18-month follow-up | ( | 2024 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic factors in colorectal cancer · Multiple and Secondary Primary Cancers · Cancer Diagnosis and Treatment
Background
Peutz–Jeghers syndrome (PJS), a rare autosomal dominant genetic disorder, manifests pathognomonically through mucocutaneous pigmentation (particularly perioral melanotic macules) and the development of hamartomatous polyposis predominantly in the gastrointestinal tract. This condition carries significant oncogenic potential, with affected individuals demonstrating predisposition to various malignancies, particularly gastrointestinal carcinomas. We present a 34-year-old female proband with familial PJS who underwent multimodal therapy for cervical carcinoma. The patient initially received liposomal paclitaxel with nedaplatin as systemic chemotherapy, which was subsequently transitioned to a paclitaxel–cisplatin regimen administered concurrently with radiotherapy as part of definitive chemoradiation. This treatment approach achieved partial response, and the patient then began maintenance therapy combining bevacizumab with chemotherapy, which culminated in complete radiographic remission. Notably, the therapeutic intervention induced progressive attenuation of characteristic orofacial melanin deposition, with chronological correlation to bevacizumab administration. The treatment course exhibited favorable tolerability without significant adverse events. Mechanistically, bevacizumab—a recombinant humanized monoclonal antibody targeting vascular endothelial growth factor (VEGF)—mediates its anti-neoplastic effects through angiogenesis inhibition, a pathway increasingly recognized as potentially modifiable in PJS-related tumorigenesis. This observation suggests a dual therapeutic potential encompassing both neoplastic control and cutaneous manifestation amelioration in PJS patients.
Case presentation
A 34-year-old Han Chinese ethnicity female patient (Ms. Wu XX) was admitted to the Gastroenterology Department in June 2022 with a 6-month history of diarrhea and hematochezia. Her medical history included open abdominal surgery for intestinal obstruction at age 13. A physical examination revealed multiple perioral melanotic macules. The patient reported a family history of intestinal polyposis and perioral pigmentation in her father and children (see genetic pedigree in Figure 1). No other significant medical or familial history was noted.
Pedigree chart of a family with Peutz–Jeghers syndrome. Symbol key: Red symbols: Individuals exhibiting mucocutaneous pigmentation. Circles: Female family members. Squares: Male family members. Symbol with checkmark (✓): Index case (proband).
Imaging and endoscopic findings (June 2022):
Thoracic and abdominal CT:
Multiple intraluminal enhancing nodules in the gastric body (greater curvature), duodenum, pelvic small bowel, and ascending colon.
Endometrial thickening with heterogeneous myometrial enhancement (suspected fibroids).
Endoscopy:
Gastroscopy: Multiple gastric and duodenal polyps.
Colonoscopy: Small bowel polyposis (consistent with Peutz–Jeghers syndrome).
Histopathology (gastric biopsy):
Hyperplastic polyps with focal mild epithelial dysplasia.
Fundic gland polyps.
Clinical course:
December 2022: Re-admitted for abdominal distension. Repeat CT showed progression of duodenal, small bowel, and colonic polyps. Underwent enteroscopic polypectomy.
March 2023: Evaluated for recurrent diarrhea and hematochezia:
Tumor markers: CA-125: 123.00 U/mL, CA19-9: 462.00 U/mL, CA72-4: 8.60 U/mL.
Transvaginal ultrasound (Figure 2): Cervical mass, endometrial thickening, and uterine fibroids.
Histopathological findings of cervical cancer in a patient with Peutz–Jeghers syndrome. The tumor tissue exhibits irregular glandular and cribriform patterns, characterized by cells with large, hyperchromatic nuclei and abundant cytoplasm, demonstrating invasive growth.
Cervical biopsy: HPV-independent gastric-type endocervical adenocarcinoma (moderately differentiated).
Immunohistochemistry: ER (-), PR (-), PTEN (weak+), PAX-8 (focal+), Ki-67 (50% in hotspot areas), p53 (mutant pattern), CK7 (+), CK20 (-), p16 (patchy+).
Imaging staging:
PET/CT:
Hypermetabolic cervical lesion (right posterior wall) involving the posterior vaginal fornix (FIGO IIA).
Mild FDG uptake in duodenal, ileocecal, and colorectal polyps (consistent with PJS).
Post-polypectomy changes without residual hypermetabolism.
Pelvic MRI: Cervical cancer (T2b), Nabothian cysts, posterior uterine fibroid, and sigmoid polyps.
Endoscopic interventions (2023):
Gastroscopy: Numerous duodenal polyps (2.0–5.0 cm), with 5 large proximal polyps resected.
Colonoscopy: 12 polyps (>2 cm) removed from cecum to sigmoid colon.
Oncologic treatment:
April–May 2023: Received liposomal paclitaxel 200 mg + nedaplatin 120 mg (2 cycles).
June 2023: Volumetric modulated arc therapy (VMAT):
PTV50.4: 5040 cGy/28 fractions.
PGTVnd: 6020 cGy/28 fractions.
Intracavitary brachytherapy: HR-CTV 3000 cGy/5 fractions.
Concurrent chemotherapy (TP regimen):
Nab-paclitaxel 400 mg (d1) + cisplatin 30 mg (d1-3).
September 2023: Partial response (PR) on MRI.
October 2023: TP regimen + bevacizumab 500 mg (d1).
November 2023: Stable disease on MRI.
Follow-up (1 year):
Achieved complete response (CR) with no cervical recurrence.
Notable lightening of perioral pigmentation following polypectomy and bevacizumab therapy (Figure 3).
Comparative analysis of perioral melanotic macules in a Peutz–Jeghers syndrome patient before and after treatment.
Full therapeutic timeline documented (Figure 4).
Therapeutic timeline and radiographic evolution in a Peutz–Jeghers syndrome patient.
Unaffected individuals: Non-consanguineous family members showed no phenotypic abnormalities.
Diagnostic considerations:
The diagnosis of Peutz–Jeghers syndrome (PJS) was established based on clinical criteria, as genetic testing was not performed due to financial constraints. According to established diagnostic guidelines (1), PJS can be confirmed by meeting any of the following criteria:
Presence of two or more histologically confirmed Peutz–Jeghers-type hamartomatous polyps.Any Peutz–Jeghers polyp in conjunction with a family history of PJS.Characteristic mucocutaneous pigmentation (involving oral mucosa, lips, nasal mucosa, periorbital region, genitalia, or digits) with a positive family history of PJS.Characteristic mucocutaneous pigmentation and any Peutz–Jeghers polyp.
Discussion
Peutz–Jeghers syndrome (PJS) is an autosomal dominant disorder with an estimated incidence ranging from 1:200,000 to 1:50,000 (2). The primary pathogenic mechanism involves loss-of-function mutations in the STK11/LKB1 gene, which disrupts multiple signaling pathways, including AMPK-mTOR, Wnt/β-catenin, and PI3K/AKT, leading to polyp formation and increased cancer susceptibility (1, 3, 4). STK11/LKB1 acts as a central regulator of cellular metabolism and proliferation. Its inactivation impairs AMPK-mediated inhibition of mTORC1, resulting in metabolic reprogramming characterized by enhanced glycolysis and lipid synthesis (the “Warburg effect”) to fuel tumor growth (5). Furthermore, STK11/LKB1 deficiency dysregulates the Hippo pathway by promoting nuclear translocation of YAP/TAZ, thereby activating pro-proliferative genes (e.g., CTGF, CYR61) and accelerating gastrointestinal polypogenesis (6). STK11/LKB1 loss also remodels the tumor microenvironment through PI3K/AKT–FOXO axis-mediated apoptosis suppression and aberrant activation of Wnt/β-catenin and Notch pathways, driving epithelial–mesenchymal transition (EMT) and cancer stemness (7, 8). Additionally, disruption of the LKB1–STRAD–MO25 complex compromises intestinal epithelial polarity via PAR1/MARK dysfunction, further impairing barrier integrity (9). Emerging evidence suggests that STK11/LKB1 modulates mitochondrial autophagy and ROS metabolism, forming a dynamic feedback loop with the p53–BAX apoptotic pathway (10, 11), which may explain the early-onset and multifocal malignancies in PJS. Collectively, these mechanisms reflect a triad of metabolic, polarity, and epigenetic dysregulation. Therapeutic strategies targeting the AMPK/mTOR–Hippo axis or combining epigenetic modifiers (e.g., HDAC inhibitors) may offer novel intervention opportunities (12).
Endoscopic polypectomy remains the cornerstone for managing gastrointestinal polyps in PJS. Balloon-assisted enteroscopy (BAE) has significantly reduced surgical needs, enabling the safe resection of polyps ≥1 cm to mitigate intussusception and obstruction risks, though repeated procedures are often required for complete small bowel surveillance (13, 14). Gastroscopy and colonoscopy effectively monitor and remove gastric/colorectal polyps with low complication rates (e.g., 0.25% perforation risk) (14). Surgery is reserved for complications (e.g., bowel necrosis, irreducible intussusception) or malignancies but may increase adhesion-related morbidity (13, 15).
Conventional approaches fail to prevent polyp recurrence or malignant transformation. PJS patients face a 37%–93% lifetime cancer risk, notably colorectal, breast, small intestinal, gastric, and pancreatic cancers (16). Recent studies focus on molecular mechanisms and targeted therapies for PJS-associated malignancies (Table 1). Cervical gastric-type adenocarcinoma (G-EAC), occurring in 11% of female PJS patients (17), exhibits aggressive behavior with early metastasis and poor response to conventional screening (TCT/HPV testing) (18). Treatment relies on surgery combined with chemoradiation and targeted therapies (Table 2), though outcomes remain inferior to HPV-related cervical cancer (19, 20). Preclinical studies explore mTOR inhibitors (e.g., everolimus), PARP inhibitors (e.g., olaparib), and AXL inhibitors (e.g., bemcentinib) to address STK11-related metabolic and DNA repair defects. Notably, combining bemcentinib with PD-1 inhibitors may overcome immunotherapy resistance in STK11-mutant tumors (20). Genetic counseling and preimplantation genetic testing (PGT) effectively prevent STK11 mutation transmission, with successful clinical applications reported (21). For mucocutaneous pigmentation, picosecond laser therapy shows promising cosmetic outcomes (22, 23).
The cervical adenocarcinoma in this case exhibited characteristic features of gastric-type adenocarcinoma (GAS), including HPV negativity and a distinctive immunohistochemical profile: ER (-), PR (-), PTEN (weak+), p53 (mutant pattern), CDX-2 (-), SATB2 (-), villin (-), CK7 (+), CK20 (-), VIM (-), and p16 (patchy+). These findings are consistent with PJS-associated cervical cancer. For limited-stage cervical cancer (IIA2), concurrent chemoradiation (IMRT + cisplatin) remains the standard treatment. However, for GAS-type cervical cancer, the TP regimen (paclitaxel + platinum) is often preferred. Bevacizumab, a monoclonal antibody targeting VEGF, inhibits tumor angiogenesis and is approved for cervical and colorectal cancers. In this case, the addition of bevacizumab to the TP regimen resulted in tumor regression and a complete response (CR), suggesting its potential efficacy in PJS-associated cervical cancer.
The mucocutaneous pigmentation in PJS is primarily caused by localized melanin deposition and dermal vascular proliferation, linked to AMPK/mTOR signaling dysregulation due to STK11/LKB1 inactivation. STK11 mutations activate the mTOR pathway, upregulating HIF-1α and VEGF expression, which stimulates angiogenesis and melanocyte activity (43, 44). VEGF not only promotes tumor angiogenesis but also induces melanocyte proliferation and migration through paracrine signaling (45). Thus, the pigmentation may reflect the systemic activation of the VEGF/mTOR pathway rather than being merely a cutaneous manifestation. Bevacizumab, by inhibiting VEGF and its downstream signaling (e.g., PI3K/AKT/mTOR) (46), may reduce melanocyte activity and melanin deposition, leading to pigmentation regression. Although this phenomenon has not been widely reported in PJS patients, this case suggests that VEGF signaling may play a significant role in the pathogenesis of mucocutaneous pigmentation in PJS. Furthermore, whether pigmentation changes can serve as a biomarker for treatment response in PJS warrants further investigation.
Future perspectives and therapeutic potential
Our study reveals that the VEGF/PI3K/AKT/mTOR signaling axis may concurrently regulate both carcinogenesis and melanin deposition in the pathogenesis of PJS, opening promising avenues to develop novel therapeutic strategies. Beyond conventional synthetic inhibitors, several natural compounds have demonstrated efficacy in modulating these key signaling pathways and warrant further investigation. Notable candidates include conjugated linoleic acid, recognized for its health-promoting properties, and epigallocatechin-3-gallate—the predominant polyphenol in green tea—which not only effectively suppresses PI3K/AKT/mTOR signaling and VEGF expression but also exhibits synergistic effects with chemotherapeutic agents in preclinical studies (47). Although we propose a mechanism whereby bevacizumab may ameliorate cutaneous hyperpigmentation by inhibiting VEGF-driven melanocyte activity—a hypothesis physiologically plausible and supported by our clinical observations—it must be emphasized that this association remains correlative and requires further validation. Our study currently lacks direct histopathological evidence, including comparative analyses of melanin content, melanocyte density, and CD31-stained microvessel density in lesions before and after treatment as well as biochemical quantification of local VEGF levels. Therefore, the inferred causal relationship should be interpreted with caution. Building on these findings, future research should establish STK11-deficient models to systematically evaluate the efficacy of natural compounds in reducing mucocutaneous pigmentation and suppressing hamartomatous polyp growth while simultaneously addressing the evidence gaps in our current study. Specifically, pre- and post-intervention histopathological analyses of model lesions—quantifying changes in melanin content, melanocyte density, microvessel density, and local VEGF levels—would provide direct evidence for the proposed mechanism. Further clinical investigations could explore the potential of natural compounds as adjuncts to targeted therapies such as bevacizumab, employing multidimensional assessments to validate synergistic effects. This approach aims to enhance therapeutic efficacy, reduce dosage requirements, minimize adverse effects, and ultimately improve long-term outcomes for PJS patients.
Author’s note
Bevacizumab is a registered trademark of Qilu Pharmaceutical Co., LTD; however, no financial or promotional relationships exist between the authors and any commercial entity associated with this drug.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Beggs AD Latchford AR Vasen HF Moslein G Alonso A Aretz S . Peutz-Jeghers syndrome: a systematic review and recommendations for management. Gut. (2010) 59:975–86. doi: 10.1136/gut.2009.198499, PMID: 20581245 · doi ↗ · pubmed ↗
- 2Giardiello FM Trimbath JD . Peutz-Jeghers syndrome and management recommendations. Clin Gastroenterol Hepatol. (2006) 4:408–15. doi: 10.1016/j.cgh.2005.11.005, PMID: 16616343 · doi ↗ · pubmed ↗
- 3Hsieh MJ Weng CC Lin YC Wu CC Chen LT Cheng KH . Inhibition of β-catenin activity abolishes LKB 1 loss-driven pancreatic cystadenoma in mice. Int J Mol Sci. (2021) 22:4649. doi: 10.3390/ijms 22094649, PMID: 33924999 PMC 8125161 · doi ↗ · pubmed ↗
- 4Glaviano A Foo ASC Lam HY Yap KCH Jacot W Jones RH . PI 3K/AKT/m TOR signaling transduction pathway and targeted therapies in cancer. Mol Cancer. (2023) 22:138. doi: 10.1186/s 12943-023-01827-6, PMID: 37596643 PMC 10436543 · doi ↗ · pubmed ↗
- 5Shackelford DB Shaw RJ . The LKB 1-AMPK pathway: metabolism and growth control in tumour suppression. Nat Rev Cancer. (2009) 9:563–75. doi: 10.1038/nrc 2676, PMID: 19629071 PMC 2756045 · doi ↗ · pubmed ↗
- 6Mohseni M Sun J Lau A Curtis S Goldsmith J Fox VL . A genetic screen identifies an LKB 1-MARK signalling axis controlling the Hippo-YAP pathway. Nat Cell Biol. (2014) 16:108–17. doi: 10.1038/ncb 2884, PMID: 24362629 PMC 4159053 · doi ↗ · pubmed ↗
- 7Ji H Ramsey MR Hayes DN Fan C Mc Namara K Kozlowski P . LKB 1 modulates lung cancer differentiation and metastasis. Nature. (2007) 448:807–10. doi: 10.1038/nature 06030, PMID: 17676035 · doi ↗ · pubmed ↗
- 8Ollila S MäkeläTP . The tumor suppressor kinase LKB 1: lessons from mouse models. J Mol Cell Biol. (2011) 3:330–40. doi: 10.1093/jmcb/mjr 016, PMID: 21926085 · doi ↗ · pubmed ↗