Effects of preoperative nutritional support combined with esketamine on recovery and analgesia after thoracoscopic radical resection of lung cancer in elderly patients
Yu Hou, Zhiru Zhan

TL;DR
This study shows that combining preoperative nutrition with esketamine improves recovery and reduces pain in elderly lung cancer patients after surgery.
Contribution
The novel approach of combining preoperative nutritional support with esketamine for postoperative pain and recovery in elderly lung cancer patients is evaluated.
Findings
Patients receiving preoperative nutrition and esketamine had lower pain scores and better sedation after surgery.
They required fewer analgesics and had fewer adverse reactions compared to the control group.
The group showed faster recovery, improved immune and nutritional markers, and better quality of life.
Abstract
This study aims to explore the effects of preoperative nutritional support combined with esketamine on recovery and postoperative pain management in elderly patients undergoing thoracoscopic radical resection for lung cancer. A total of 165 elderly patients with lung cancer who underwent thoracoscopic radical resection at our hospital between June 2021 and March 2023 were enrolled and divided into a study group (SG, n = 85) and a control group (CG, n = 80). The SG received patient-controlled analgesia with esketamine, sufentanil, dexamethasone, and dexmedetomidine, while the CG received sufentanil, dexamethasone, and dexmedetomidine. The SG received nutritional support both pre- and postoperatively, whereas the CG received it only postoperatively. We compared resting and coughing visual analog scale (VAS) scores; Ramsay sedation scores at 6, 12, 24, and 48 h post-surgery; the number of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
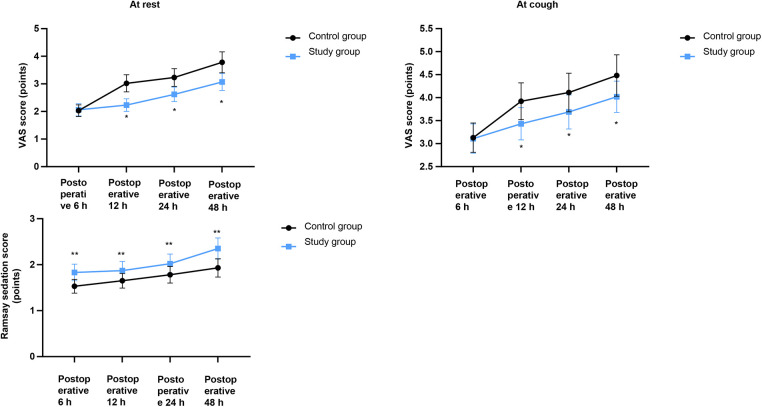 Figure 1
Figure 1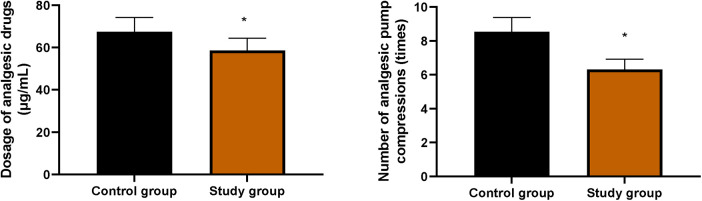 Figure 2
Figure 2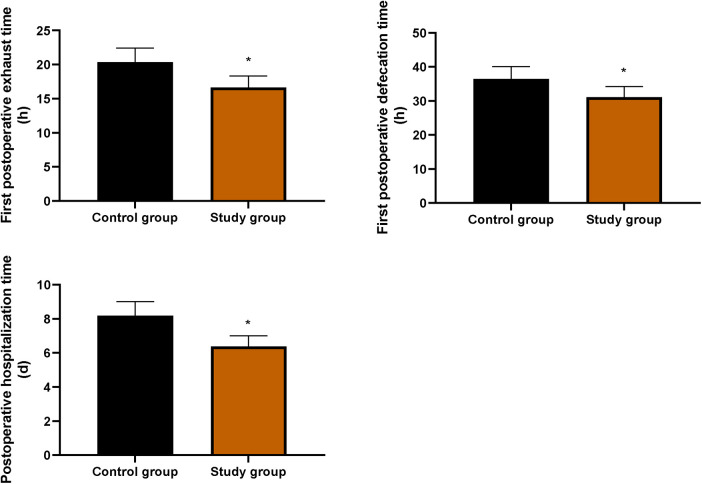 Figure 3
Figure 3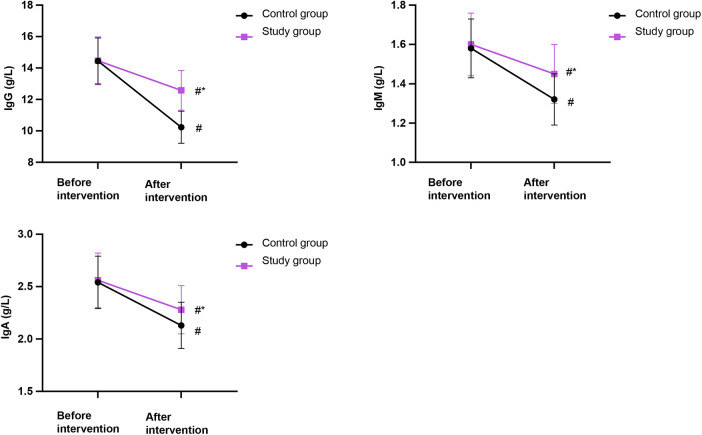 Figure 4
Figure 4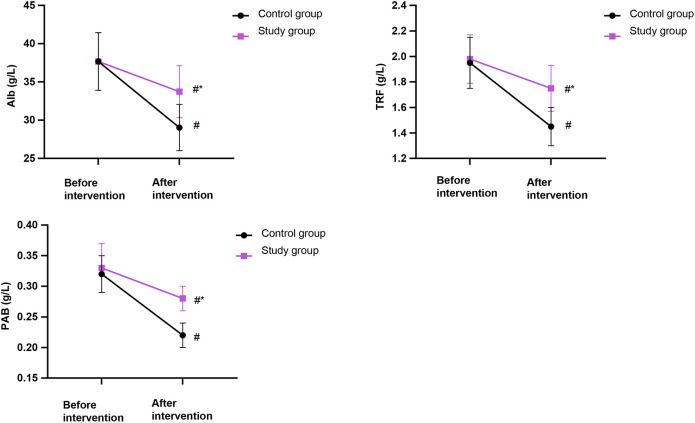 Figure 5
Figure 5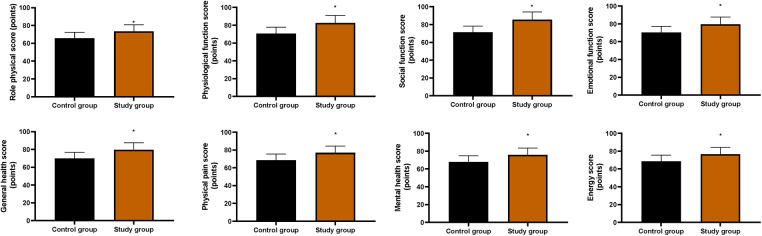 Figure 6
Figure 6| Groups | Cases | Respiratory depression | Hypotension | Nausea and vomiting | Dizziness | Total incidence rate |
|---|---|---|---|---|---|---|
| Control group | 80 | 3 | 2 | 2 | 2 | 9 (11.25%) |
| Study group | 85 | 1 | 0 | 1 | 1 | 2 (2.35%) |
|
| 5.24 | |||||
|
| 0.02 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Stress, Anesthesia, and Immune Response · Enhanced Recovery After Surgery · Nausea and vomiting management
Introduction
Lung cancer is a leading cause of cancer-related mortality worldwide, particularly among the elderly population (1). Radical resection is the primary treatment for stage I and II lung cancer (2), with reported 5-year survival rates reaching up to 80% and generally favorable prognoses (3). Thoracoscopic radical resection has become a common surgical approach offering advantages over traditional thoracotomy, such as less trauma and shorter operation duration (4). However, elderly patients often present with compromised physiological reserves and comorbidities such as chronic obstructive pulmonary disease (5), making them highly vulnerable to postoperative complications arising from surgical stress and pain, such as respiratory dysfunction and delayed recovery, which prolong hospitalization and increase burdens (6).
Effective postoperative analgesia is crucial yet challenging. While opioids are potent analgesics, their use, especially in the elderly, is limited by dose-dependent adverse effects, including respiratory depression, nausea, and the risk of tolerance (7, 8). This underscores the importance of multimodal analgesia strategies. The inclusion of N-methyl-D-aspartic acid (NMDA) receptor antagonists such as esketamine is recommended to improve analgesic efficacy and reduce opioid consumption (9). Esketamine, a novel NMDA receptor antagonist, provides effective analgesia with a favorable safety profile, potentially benefiting elderly patients (10).
Parallel to pain management, nutritional status is a key determinant of surgical outcomes. Surgical stress can lead to a catabolic state and malnutrition, impairing immune function and tissue repair, which is particularly detrimental in elderly cancer patients (11). Although enteral nutrition is essential, postoperative administration alone is often hampered by gastrointestinal intolerance (12). Evidence suggests that actively correcting the nutritional status before surgery and allowing the intestine to adapt to the enteral nutrient solution in advance can improve the compliance of postoperative enteral nutrition (13).
Therefore, we hypothesized that combining preoperative nutritional support with an esketamine-based analgesic regimen would synergistically improve recovery in elderly patients undergoing thoracoscopic lung cancer surgery. This study aimed to explore the effects of this combined approach on analgesia, recovery, immune function, and quality of life.
Methods
Study patients
A total of 165 elderly patients with lung cancer who underwent thoracoscopic radical resection at our hospital between June 2021 and March 2023 were enrolled. Inclusion criteria were as follows: (1) age >60 years; (2) pathological confirmation of lung cancer and scheduled for thoracoscopic radical resection; (3) complete clinical data; and (4) tumor stage I or II. Exclusion criteria were as follows: (1) history of radiotherapy or chemotherapy; (2) other concurrent cancers; (3) chronic pain history, long-term analgesic use or alcohol abuse; (4) allergy to study medications; (5) psychiatric disorders; or (6) severe systemic diseases. Patients were divided into a study group (SG, n = 85) and a control group (CG, n = 80) based on the analgesia protocol. The SG comprised 45 males and 40 females, with a mean age of 68.46 ± 6.35 years (range: 61–82) and 46 stage I/39 stage II cases. The CG comprised 42 males and 38 females, with a mean age of 68.53 ± 6.42 years (range: 62–80) and 45 stage I/35 stage II cases. No significant differences in baseline characteristics were observed between groups (P > 0.05), indicating comparability. All participants provided written informed consent.
Anesthesia methods
All patients fasted and abstained from fluids before surgery. Blood pressure (BP), electrocardiogram (ECG), and blood oxygen saturation (SpO_2_) were monitored.
Peripheral venous access was established. Under local anesthesia, all patients underwent radial artery puncture for invasive arterial pressure monitoring. Combined inhalational and intravenous anesthesia was administered. Anesthesia was induced with intravenous sufentanil (0.4–0.5 µg/kg), etomidate (0.15–0.30 mg/kg), and rocuronium (0.6–0.9 mg/kg). A double-lumen bronchial tube was inserted, with placement confirmed by fiber-optic bronchoscopy before initiating mechanical ventilation. Anesthesia was maintained using intravenous infusions of propofol [4–8 mg/(kg·h)], remifentanil [6–10 µg/(kg·h)], dexmedetomidine [0.25–0.5 µg/(kg·h)], and cisatracurium [0.1 mg/(kg·h)], supplemented with 1%–2% sevoflurane inhalation. Intraoperatively, BP and heart rate were maintained within ±20% of baseline, and nasal temperature was kept at 36°C−37°C by adjusting fluid administration and using vasoactive drugs as needed. Sufentanil 10 µg was injected intravenously before the end of the operation. After patients woke up, the tracheal catheter was removed, and they were sent to the recovery room.
Analgesia methods
Postoperative analgesia was administered via a patient-controlled intravenous analgesia (PCIA) pump. CG: sufentanil (Yichang Renfu Pharmaceutical Co., Ltd., specification 50 µg: 1 mL) 1.5 µg/kg + dexamethasone 5 mg + dexmedetomidine 100 µg.
SG: esketamine (Jiangsu Hengrui Pharmaceutical Co., Ltd., specification 50 mg: 2 mL) 0.2 mg/kg + sufentanil 1.3 µg/kg + dexamethasone 5 mg + dexmedetomidine 100 µg.
Preoperative nutritional support methods
The SG received enteral nutritional support both pre- and postoperatively. One week before surgery, patients received 1,000 kcal/day of Weikaneng Balanced Nutrient (Harbin Byronst Clinical Nutrition Co., Ltd.; 1.0 kcal/mL) orally, in addition to a liquid diet. Postoperatively, on day 1, patients received 250 mL of isotonic sodium chloride solution. On day 2, they received 500 mL of Weikaneng Short Peptide (Harbin BST Clinical Nutrition Co., Ltd.; 0.85 kcal/mL) administered via nasogastric tube using an enteral nutrition pump over 24 h, along with 250 mL of isotonic sodium chloride solution. On day 3, the regimen consisted of 500 mL Weikaneng Short Peptide plus 500 mL Weikaneng Balanced Nutrient. From day 4 to day 9, patients received continuous 24 h infusion of Weikaneng Balanced Nutrient.
The CG received postoperative enteral nutritional support only, following the same postoperative protocol as the SG from day 1 onward.
The nutritional support regimen was administered as a fixed-dose protocol according to our institutional clinical pathway for perioperative care and was not adjusted based on individual patient body weight. Adherence to the oral and enteral nutrition protocol was monitored and recorded by the ward nursing staff. Compliance was defined as consumption of >90% of the prescribed volume.
Observation indicators
(1)Pain and sedation: Visual analog scale (VAS) scores (at rest and during cough) and Ramsay sedation scores were recorded at 6, 12, 24, and 48 h postoperatively.(2)Analgesic consumption: The number of analgesic pump compressions and total analgesic drug dosage within 48 h after surgery were recorded.(3)Adverse reactions: The incidence of adverse reactions within 48 h, including respiratory depression, hypotension, nausea and vomiting, and dizziness, was recorded.(4)Recovery indicators: Postoperative recovery was assessed by measuring the time to first exhaust, first defecation, and the duration of postoperative hospitalization.(5)Immune function: Serum levels of immunoglobulin M (IgM), G (IgG), and A (IgA) were measured using immunoturbidimetry.(6)Nutritional status: A 5 mL sample of cubital venous blood was collected. Nutritional markers—albumin (Alb), transferrin (TRF), and prealbumin (PAB)—were analyzed using an AU5400 automated biochemical analyzer.(7)Quality of life: Quality of life was assessed using the 36-Item Short Form Health Survey (SF-36) prior to discharge. The SF-36 evaluates eight domains: physical functioning, role—physical, bodily pain, general health, vitality, social functioning, role—emotional, and mental health.
Statistical analysis
Data were analyzed using SPSS software (version 24.0). Continuous data were presented as mean ± standard deviation (SD) and were compared using the t-test. Categorical data were expressed as numbers and percentages (n, %) and were compared using the chi-squared (χ^2^) test. A P-value of <0.05 was considered statistically significant. All analyzed variables had complete data for the 165 included patients. Therefore, no specific methods for handling missing data were employed.
Results
VAS scores and Ramsay sedation scores in both groups
As shown in Figure 1, the SG had significantly lower VAS scores at rest and during cough at 6, 12, 24, and 48 h postoperatively compared with the CG (P < 0.05). Concurrently, the SG also demonstrated significantly higher Ramsay sedation scores at all corresponding time points (P < 0.05).
*VAS scores and Ramsay sedation scores in both groups. VAS, visual analog scale. Data were presented as mean ± standard deviation. SG, study group [esketamine-containing analgesia (esketamine + sufentanil + dexamethasone + dexmedetomidine) combined with preoperative and postoperative enteral nutrition support]; CG, control group [standard analgesia (sufentanil + dexamethasone + dexmedetomidine) combined with postoperative only enteral nutrition support]. P < 0.05.
Number of analgesic pump compressions and the dosage of analgesic drugs within 48 h after surgery in both groups
Figure 2 shows that the SG required significantly fewer analgesic pump compressions and a lower total analgesic dosage within 48 h postoperatively compared with the CG (P < 0.05).
*Number of analgesic pump compressions and the dosage of analgesic drugs within 48 h after surgery in both groups. Data were presented as mean ± standard deviation. SG, study group [esketamine-containing analgesia (esketamine + sufentanil + dexamethasone + dexmedetomidine) combined with preoperative and postoperative enteral nutrition support]; CG, control group [standard analgesia (sufentanil + dexamethasone + dexmedetomidine) combined with postoperative only enteral nutrition support]. P < 0.05.
Occurrence of adverse reactions within 48 h after surgery in both groups
Table 1 demonstrates a significantly lower incidence of adverse reactions within 48 h postoperatively in the SG compared with that in the CG (P < 0.05).
Postoperative recovery indicators in both groups
As shown in Figure 3, the times to first exhaust, first defecation, and postoperative hospitalization were all significantly shorter in the SG compared with the CG (P < 0.05).
*Postoperative recovery indicators in both groups. Comparison of the first postoperative exhaust time, first postoperative defecation time, and postoperative hospitalization time between the two groups. Data were presented as mean ± standard deviation. SG, study group [esketamine-containing analgesia (esketamine + sufentanil + dexamethasone + dexmedetomidine) combined with preoperative and postoperative enteral nutrition support]; CG, control group [standard analgesia (sufentanil + dexamethasone + dexmedetomidine) combined with postoperative only enteral nutrition support]. P < 0.05.
Immune indicators in both groups
Figure 4 shows no significant difference in immune indicators (IgG, IgM, IgA) between the two groups before the intervention (P > 0.05). After the intervention, although the levels of these immunoglobulins decreased in both groups, they remained significantly higher in the SG than those in the CG (P < 0.05).
*Comparison of immune indicators in both groups. IgG, immunoglobulin G; IgM, immunoglobulin M; IgA, immunoglobulin A (g/L). Data were presented as mean ± standard deviation. SG, study group [esketamine-containing analgesia (esketamine + sufentanil + dexamethasone + dexmedetomidine) combined with preoperative and postoperative enteral nutrition support]; CG, control group [standard analgesia (sufentanil + dexamethasone + dexmedetomidine) combined with postoperative only enteral nutrition support]. #P < 0.05, compared with before intervention, P < 0.05, compared with CG.
Nutritional status in both groups
Figure 5 shows no significant differences in nutritional indexes (Alb, TRF, PAB) between the two groups before the intervention (P > 0.05). After the intervention, although levels of these markers decreased in both groups, the SG maintained significantly higher levels than the CG (P < 0.05).
*Comparison of nutritional status in both groups. Alb, albumin; TRF, transferrin; PAB, prealbumin (g/L). Data were presented as mean ± standard deviation. SG, study group [esketamine-containing analgesia (esketamine + sufentanil + dexamethasone + dexmedetomidine) combined with preoperative and postoperative enteral nutrition support]; CG, control group [standard analgesia (sufentanil + dexamethasone + dexmedetomidine) combined with postoperative only enteral nutrition support]. #P < 0.05, compared with before intervention, P < 0.05, compared with CG.
Quality of life in both groups
As shown in Figure 6, the SG showed significantly higher scores across all dimensions of the SF-36 compared with the CG (P < 0.05).
*Quality of life in both groups. *P < 0.05. Scores of the eight domains of the 36-Item Short Form Health Survey (SF-36) were shown. Data were presented as mean ± standard deviation. SG, study group [esketamine-containing analgesia (esketamine + sufentanil + dexamethasone + dexmedetomidine) combined with preoperative and postoperative enteral nutrition support]; CG, control group [standard analgesia (sufentanil + dexamethasone + dexmedetomidine) combined with postoperative only enteral nutrition support]. P < 0.05.
Discussion
The incidence of lung cancer increases with age (14). Patients undergoing thoracoscopic radical resection for lung cancer often experience moderate to severe postoperative pain (15). With the growing adoption of enhanced recovery after surgery (ERAS) protocols, multimodal analgesia has been increasingly implemented for these patients (16). Effective analgesia can reduce the incidence of postoperative complications, such as respiratory depression (17). Although opioid-based intravenous analgesia remains the most common clinical approach, excessive opioid use can lead to adverse effects including respiratory depression, nausea, vomiting, and dizziness (18).
As a classic NMDA receptor antagonist, esketamine effectively reduces perioperative pain sensitization and enhances the analgesic effect of opioids, thereby reducing their required dosage (19). At the same time, esketamine can stimulate the central sympathetic nerve, release nerve catecholamines, and avoid hypotension, which is especially suitable for elderly patients with unstable hemodynamics (20). Recent thoracic surgery-specific evidence strengthens our findings. A study by Zhang et al. (21) showed that adding 0.2 mg kg^−^¹ esketamine to intravenous patient-controlled analgesia reduced 48 h sufentanil consumption by 35% after thoracoscopic lung resection. Yan et al. (22) achieved complete intraoperative opioid avoidance with systemic plus epidural esketamine and observed a lower incidence of chronic postsurgical pain at 3 months. In spontaneous ventilation video-assisted thoracic surgery, Fan et al. (23) recorded a 42% remifentanil sparing and better oxygenation, while Zeng et al. (24) demonstrated that a single intraoperative bolus halved the incidence of severe rebound pain after thoracic paravertebral block.
In this study, the SG demonstrated significantly lower VAS scores (at rest and during cough) and higher Ramsay sedation scores at 6, 12, 24, and 48 h postoperatively compared with the CG. The SG also required fewer analgesic pump compressions and a lower total analgesic dosage within 48 h, with a concurrent reduction in adverse reactions. These findings indicate that esketamine may effectively reduce the postoperative pain and agitation of patients, reduce the dosage of opioid analgesics, and reduce the occurrence of respiratory depression, hypotension, and other related adverse reactions caused by opioids, which is consistent with a previous study (25).
Studies have shown that early postoperative enteral nutrition provides essential energy, protein, fat, and carbohydrates, thereby helping to maintain postoperative metabolic balance and promote the recovery of intestinal digestion, absorption, and barrier function. It is therefore the preferred method of nutritional support (26). However, the rapid administration of a large volume of enteral nutrition shortly after surgery may lead to gastrointestinal intolerance, resulting in symptoms such as abdominal distension, pain, diarrhea, and gastric retention (27). Gastrointestinal intolerance compromises the effectiveness of enteral nutrition and increases the risk of treatment failure (28). Therefore, attention should be paid to the problem of postoperative enteral nutrition support intolerance, and practical measures should be taken to improve the compliance of postoperative enteral nutrition.
In our study, the outcomes displayed that IgG, IgM, IgA, Alb, TRF, and PAB levels were higher in the SG compared with the CG, suggesting that preoperative enteral nutrition support may enhance the immune function and nutritional status of patients receiving thoracoscopic radical resection of lung cancer. The underlying mechanisms for these improvements are likely multifactorial. We speculate that (1) the enteral nutrient solution contained various amino acids, proteins, fats, vitamins, organophosphates, trace elements, and other components, which were taken orally in a small dose before the operation and gradually increased. After absorption through the digestive tract, the nutritional status could be directly improved (29). These immune and nutritional benefits are supported by recent intervention studies. In a 2022 phase II trial of non-small cell lung cancer (NSCLC) patients, perioperative immunonutrition elevated serum IgG, IgA, IgM, and CD4+ counts while increasing pre-Alb levels (30). A 2023 meta-analysis pooling 28 randomized controlled trials (RCTs) confirmed significant standardized mean differences for IgG (0.98), IgM (1.15), and prealbumin (0.73) when immunonutrition was administered ≥7 days before surgery (31). More importantly, (2) the preoperative administration of a small dose of enteral nutrient solution might have primed the gastrointestinal tract, enhancing its tolerance to postoperative feeding. This could help maintain gut barrier function, reduce postoperative intolerance, and thereby improve the overall success of nutritional support, which is crucial for modulating immune and metabolic responses after surgery (32). Protection of the gut barrier has been documented by Li and Wang, who observed decreased intestinal permeability markers (DAO, D-lactate) and fewer episodes of bacterial translocation when low-dose EN was commenced 5 days pre-operatively (33). However, these mechanisms remain speculative within the context of our study, and further investigation is warranted to elucidate the precise pathways.
Furthermore, our study found that compared with the CG, the SG showed significantly shorter times to first exhaust, first defecation, and postoperative hospitalization, along with higher scores across all SF-36 dimensions. These results suggest that the combination of preoperative nutritional support and esketamine is associated with accelerated postoperative recovery and improved quality of life in elderly patients undergoing thoracoscopic lung cancer surgery, which is consistent with previous studies (34, 35).
This study has several limitations that must be emphasized when interpreting its findings. Firstly and most importantly, the non-randomized, retrospective design is a fundamental limitation. The allocation of patients to the study and control groups was based on clinical practice rather than randomization, which inherently carries a risk of selection bias and unmeasured confounding. Although baseline characteristics were comparable, this design significantly weakens the strength of causal inference regarding the effects of the combined intervention. Secondly, the single-center nature of the study limits the generalizability of our results. The findings may be influenced by specific institutional protocols, surgical expertise, and patient populations, and thus may not be directly applicable to other settings. Thirdly, the absence of blinding is a notable source of potential bias. The patients and clinicians involved in outcome assessment were aware of the group assignments, which could have influenced the reporting of subjective outcomes such as pain scores (VAS) and quality of life (SF-36). Finally, the follow-up period was relatively short, focused exclusively on the immediate postoperative hospitalization phase. This design does not allow for any conclusions regarding long-term outcomes, including 30-day readmission or complication rates, overall survival, or the sustainability of the observed improvements in immune function and quality of life. Future large-scale, multicenter, prospective, randomized, double-blind trials with long-term follow-up are essential to confirm our findings and establish the long-term benefits of this combined approach.
Conclusion
Our findings suggest that for elderly patients after thoracoscopic radical resection of lung cancer, the combined approach of preoperative nutritional support and esketamine may lead to improved analgesia, enhanced recovery, better preservation of immune and nutritional function, and an improved quality of life, suggesting it may be a beneficial strategy within an enhanced recovery protocol.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The Lancet. Lung cancer: some progress, but still a lot more to do. Lancet. (2019) 394:1880. 10.1016/S 0140-6736(19)32795-331777378 · doi ↗ · pubmed ↗
- 2Brunelli A Charloux A Bolliger CT Rocco G Sculier JP Varela G ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur Respir J. (2009) 34:17–41. 10.1183/09031936.0018430819567600 · doi ↗ · pubmed ↗
- 3Lowczak A Kolasinska-Cwikla A Ćwikła JB Osowiecka K Palucki J Rzepko R Outcomes of patients with clinical stage I–IIIA large-cell neuroendocrine lung cancer treated with resection. J Clin Med. (2020) 9:1370. 10.3390/jcm 905137032392725 PMC 7290504 · doi ↗ · pubmed ↗
- 4Chai T Lin Y Kang M Lin J. Thoracotomy versus video-assisted thoracoscopic resection of lung cancer: a protocol for a systematic review and meta-analysis. Medicine. (2019) 98:e 14646. 10.1097/MD.000000000001464630855453 PMC 6417539 · doi ↗ · pubmed ↗
- 5Hey JC. Lung cancer in elderly patients. Clin Geriatr Med. (2003) 19:139–55. 10.1016/S 0749-0690(02)00067-812735119 · doi ↗ · pubmed ↗
- 6Huyan T Hu X Peng H Zhu Z Li Q Zhang W. Perioperative dexmedetomidine reduces delirium in elderly patients after lung cancer surgery. Psychiatr Danub. (2019) 31:95–101. 10.24869/psyd.2019.9530948695 · doi ↗ · pubmed ↗
- 7Mercadante S Arcuri E Santoni A. Opioid-induced tolerance and hyperalgesia. CNS Drugs. (2019) 33:943–55. 10.1007/s 40263-019-00660-031578704 · doi ↗ · pubmed ↗
- 8Oldham JM. Opioids. J Psychiatr Pract. (2020) 26:1–2. 10.1097/PRA.000000000000044431913964 · doi ↗ · pubmed ↗