Efficacy and safety of PARP inhibitors in advanced or recurrent endometrial cancer: a systematic review and meta-analysis
Huanhuan Zhang, Guangwei Yan, Jinxiang Yan, Xianxu Zeng

TL;DR
This study reviews clinical trials to assess how effective and safe PARP inhibitors are for treating advanced or recurrent endometrial cancer, both alone and in combination with other drugs.
Contribution
The study provides a meta-analysis of PARP inhibitors in endometrial cancer, highlighting the benefits and risks of combination therapies.
Findings
Combining PARP inhibitors with PD-L1/PD-1 inhibitors significantly prolonged progression-free survival.
PARP inhibitor monotherapy showed no significant improvement in survival compared to placebo.
Common side effects included fatigue, nausea, anemia, diarrhea, and alopecia.
Abstract
Several clinical trials have explored the efficacy and safety of Poly (ADP-ribose) polymerase (PARP) inhibitors in endometrial cancer (EC). However, evidence supporting PARP inhibitors alone or in combination with other medications in advanced or recurrent EC remains limited. We utilized Cochrane Library, PubMed, Web of Science, and Embase to identify clinical trials that evaluated the efficacy and safety of PARP inhibitors in advanced and recurrent EC. The outcomes analyzed included progression-free survival (PFS), overall survival (OS), objective response rate (ORR), and adverse events (AEs). We computed hazard ratios (HRs) for PFS and OS, with 95% confidence intervals (CIs) from randomized trials. Subgroup analysis was conducted based on the PARP inhibitor combination therapy strategies (with antiprogrammed death 1 [PD-1]/antiprogrammed death ligand-1 [PD-L1] inhibitors or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
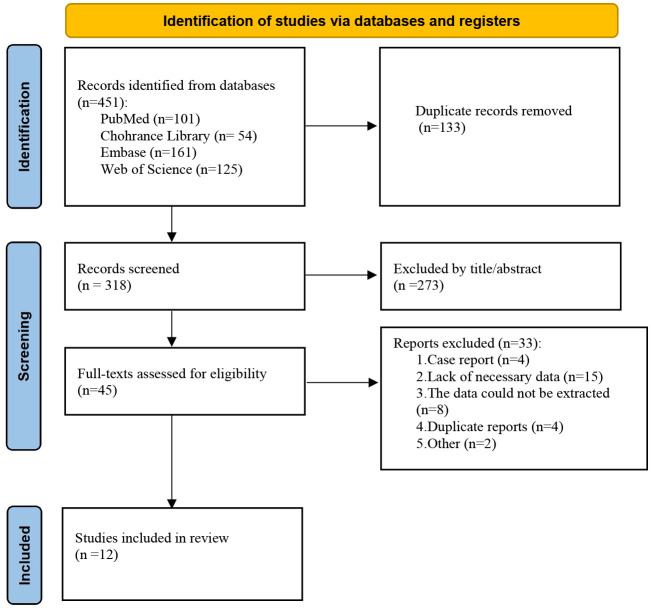 Figure 1
Figure 1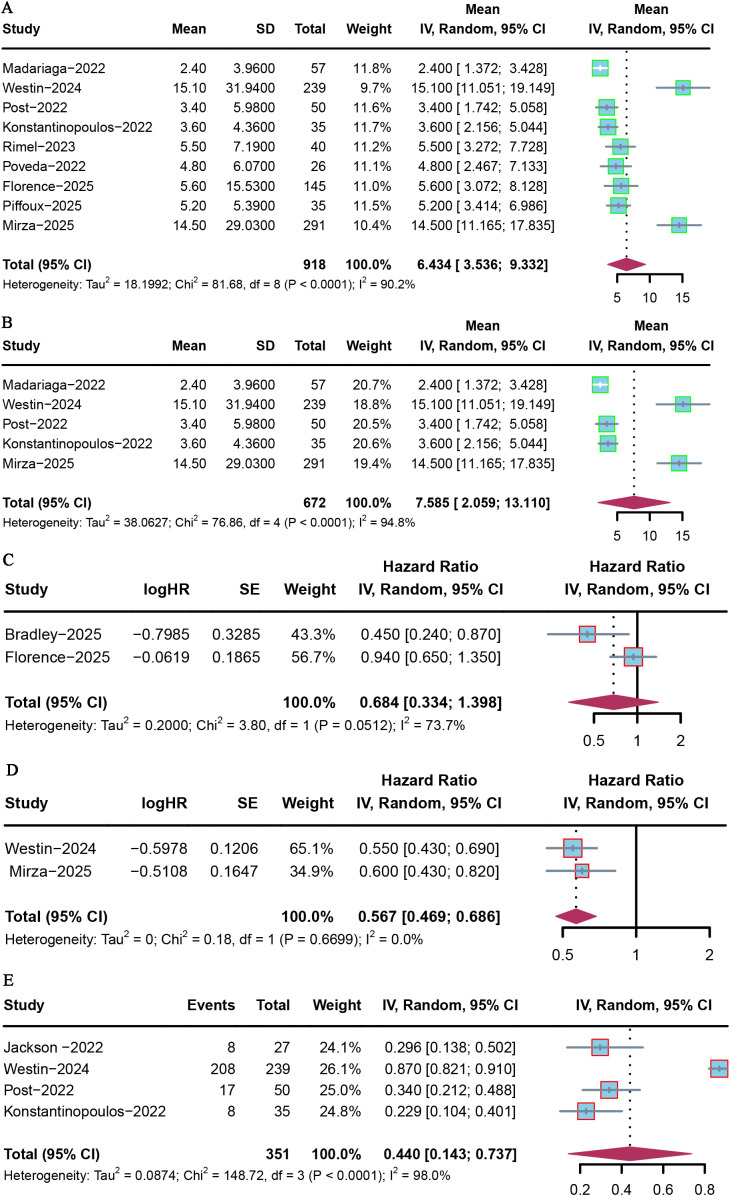 Figure 2
Figure 2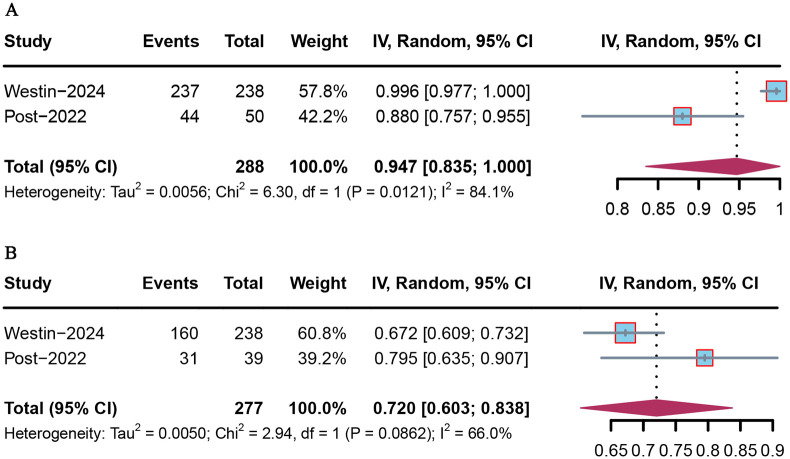 Figure 3
Figure 3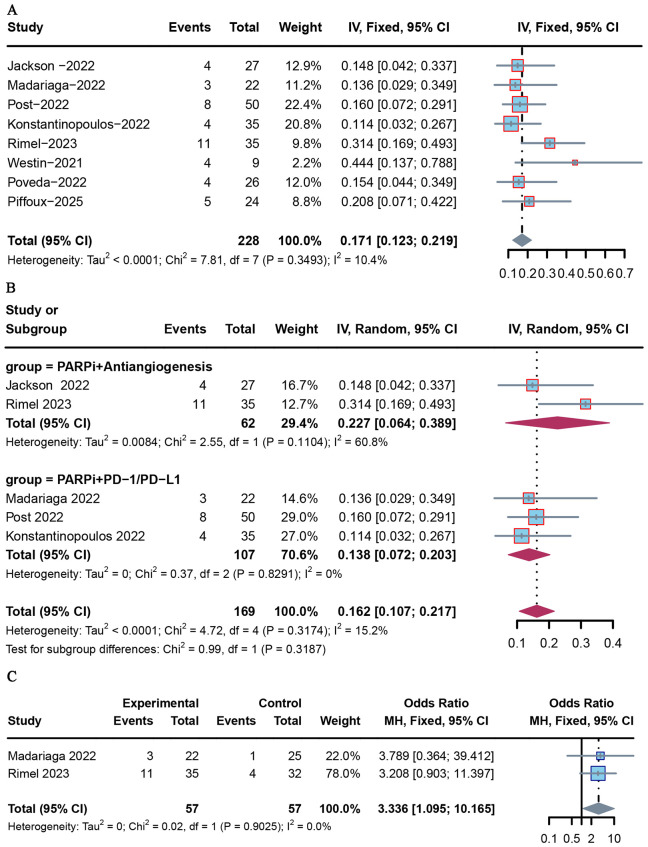 Figure 4
Figure 4| Outcomes and subgroups | Number of studies | Meta-analysis | Heterogeneity | |||||
|---|---|---|---|---|---|---|---|---|
| Pooled estimates (95% CI) | HR (95% CI) |
| Tau2 | Analysis model | ||||
| PFS | ||||||||
| Overall | 9 | 6.434 (3.536–9.332) | – | – | ##### | 18.2 | < 0.0001 | Random-effects |
| PARP with PD-L1/PD-1 inhibitors | 5 | 7.585 (2.059-13.110) | – | – | ##### | 38.062 | < 0.0001 | Random-effects |
| PARP inhibitors vs. placebo | 2 | – | 0.684 (0.334–1.398) | 0.297 | ##### | 0.2 | 0.0512 | Random-effects |
| PARP with PD-L1/PD-1 inhibitors vs. placebo | 2 | – | 0.567(0.469-0.686) | < 0.0001 | 0 | 0 | 0.669 | Fixed-effects |
|
| 4 | 0.440(0.143-0.737) | – | – | ##### | 0.087 | < 0.0001 | Random-effects |
| OS | ||||||||
| Overall | 4 | 11.837 (3.124–20.549) | – | – | ##### | 73.45 | < 0.0001 | Random-effects |
| PARP inhibitors vs. placebo | 2 | – | 0.787 (0.279–2.219) | 0.651 | ##### | 0.443 | 0.034 | Random-effects |
| ORR | ||||||||
| Overall | 8 | 0.171 (0.123–0.219) | – | – | ##### | < 0.0001 | 0.349 | Fixed-effects |
| PARP with PD-L1/PD-1 inhibitors | 3 | 0.138 (0.072–0.203). | – | – | 0.00% | 0.00% | 0.829 | Fixed-effects |
| PARP with antiangiogenesis | 2 | 0.227 (0.064–0.389) | – | – | ##### | 0.008 | 0.11 | Random-effects |
| PARP inhibitors combined therapy vs. monotherapy | 2 | – | 0.300 (0.098–0.913) | 0.034 | 0% | 0 | 0.903 | Fixed-effects |
| AEs | ||||||||
| Any grade | 2 | 0.947 (0.835–1.00) | – | – | ##### | 0.006 | 0.121 | Random-effects |
| AEs of grade ≥ 3 | 2 | 0.720 (0.603–0.838) | – | – | 0.66 | 0.005 | 0.086 | Random-effects |
| Author (year) | Clinical trial | Study design | Sample size | Population | Experimental arm | Control arm ( | Endpoints | ORR | HR (95% CI)-PFS | Median PFS (months, median; 95% CI) | 6-month PFS rate (%; 95% CI) | HR (95% CI)-OS | Median OS (months, median; 95% CI) | Follow-up time (median/months) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Jackson (2022) ( | Phase II | 27 | Recurrent EC | Bevacizumab + rucaparib | – | ORR, PFS6 | 14% (4/27) | – | – | 30 (10–50) | – | – | 25 months | |
| 2 | Madariaga (2022) ( | Phase II | 57 | Recurrent EEC/SE | Niraparib + dostarlimab (22) | Niraparib (25) | ORR, DCR, PFS, OS | 4% (1/25) | – | 2.5 (1.8–3.7) | – | – | 12.5 (6.6–19.3) | – | |
| 3 | Westin (2024) ( | Phase III | 718 | Advanced/metastatic EC | Durvalumab + olaparib ( | Placebo ( | PFS, OS | – | Durvalumab + olaparib: 0.55 (0.43–0.69); durvalumab: 0.71 (0.57–0.89) | Durvalumab + olaparib: 15.1 (12.6–20.7); durvalumab: 10.2 (9.7–14.7); placebo: 9.6 (9.0–9.9) | Durvalumab + olaparib: 87.2 (73.8–94.1); durvalumab: 83.8 (78.4–88.0); placebo: 82.5 (76.9–86.8) | Durvalumab + olaparib: 0.59 (0.42–0.83); durvalumab: 0.77 (0.56–1.07) | Durvalumab + olaparib: NR (NR–NR); durvalumab: NR (NR–NR); placebo: 25.9 (23.9–NR) | Durvalumab + olaparib, durvalumab: 0.71 (0.57–0.89): 15.4 months; placebo: 12.6 months | |
| 4 | Post (2022) ( | Phase II | 50 | Advanced EC | Durvalumab + olaparib | – | PFS6, ORR, OS | 16% (8/50) | – | 3.4 (2.8–6.2) | 34.0 (23.1–50.0) | 8.0 (7.5–14.3) | 17.6 months | ||
| 5 | Konstantinopoulos (2022) ( | Phase II | 35 | Recurrent pMMR EC | Talazoparib + avelumab | – | PFS6, ORR | 11.4% (4/35) | – | 3.6 (2.4–5.4) | 22.9 (10.4–40.1) | – | 12.9 months | ||
| 6 | Rimel (2022) ( | Phase II | 120 | Advanced/metastatic EC | Olaparib ( | Cediranib ( | PFS, ORR, OS | Cediranib: 24.1% (7/29); olaparib: 12.5% (4/32); olaparib + cediran:31.4% (11/35) | Cediranib: 1.45 (one‐sided 95% CI, 2.14); olaparib + cediran: 0.7 (95% CI, 1.05) | Cediranib: 3.8 (3–5.4); olaparib: 2.0 (1.8–4.7); olaparib + cediran: 5.5 (3.7–8.3) | – | Cediranib: 1.01 (one‐sided 95% CI, 1.62); olaparib + cediran: 5.5 (3.7–8.3):0.75 (95% CI, 1.25) | Cediranib: 12.4 (7.5–22.9); olaparib: 13.4 (6.5–19.5); olaparib + cediran: 17.6 (9.7–NR) | 18.3 months | |
| 7 | Westin (2021) ( | Phase Ib | 11 | Recurrent EC | Olaparib + capivasertib | – | ORR | 44% (4/9) | – | – | – | – | – | 7.4 months | |
| 8 | Poveda (2022) ( | Phase II | 26 | Advanced/metastatic EEC | Lurbinectedin + olaparib | – | ORR, PFS, OS | 15.4% (4/26) | – | 4.8 (1.9–6.8) | – | – | 15.9 (7.2–23.3) | – | |
| 9 | Bradley (2025) ( | Phase II | 79 | Advanced/metastatic EC | Rucaparib (39) | Placebo (40) | PFS, OS | – | 0.45 (0.24–0.87) | Rucaparib: 28.1 (12.8–NR); placebo: 8.7 (5.4–16.7) | – | 0.43 (0.18–1.05) | Rucaparib: NR (34.8–NR); placebo: 28.4 (19.0–NR) | 25 months | |
| 10 | Florence (2025) ( | Phase IIb | 145 | Advanced/metastatic EC | Olaparib (96) | Placebo (49) | PFS, OS | – | 0.94 (0.65–1.35) | 5.6 (3.7–8.8) | – | 1.25 (0.80–1.94) | 22.2 (16.0–25.3) | 31.9 months | |
| – | – | – | 4.0 (3.5–7.7) | – | – | 23.8 (19.6–28.6) | |||||||||
| 11 | Piffoux (2025) ( | Phase I/II | 35 | Advanced/metastatic EC | Olaparib + metformin | – | PFS, ORR | 20.80% | – | 5.2 (5.1–8.8) | – | – | – | 5.1 months | |
| 12 | Mirza (2025) ( | Phase III | 291 | Advanced/metastatic EC | Dostar/CP + dostar/nira (192) | PBO/CP + PBO (99) | PFS | – | 0.60 (0.43–0.82) | Dostar/CP + dostar/nira: 14.5 (11.8–17.4); PBO/CP + PBO: 8.3 (7.6–9.8) | – | – | – | 19 months |
| Author/ year | Madariaga ( | Westin ( | Post ( | Konstantinopoulos ( | Rimel ( | Piffoux (31) | Total ( | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Any grade | Grade 3/4 | Any grade | Grade 3/4 | Any grade | Grade 3/4 | Any grade | Grade 3/4 | Any grade | Grade 3/4 | Any grade | Grade 3/4 | Any grade | Grade 3/4 | |
| Any-grade AE | – | – | 237 (99.6%) | 160 (67.2%) | 44 (88%) | 8 (16%) | – | – | – | 31 (79.4%) | – | – | ||
| Fatigue | 11 (50%) | 1 (5) | 129 (54.2%) | 12 (5.0%) | 22 (44%) | 2 (4%) | 16 (45%) | 4 (11%) | 29 (72.5%) | 8 (20.5%) | 19 (61.3%) | 4 (12.9%) | 226 (54.5%) | 31 (7.5%) |
| Nausea | 13 (59%) | 1 (5%) | 130 (54.6%) | – | 19 (38%) | 1 (2%) | 12 (35%) | 0 | 28 (70%) | 2 (5.1%) | 17 (54.8) | 0 (0%) | 219 (52.8%) | 4 (1.0%) |
| Anemia | 9 (41%) | 6 (27%) | 147 (61.8%) | 56 (23.5) | 16 (32%) | 5 (10%) | 25 (72%) | 16 (46%) | – | – | 22 (70.9%) | 5 (16.1%) | 219 (52.8%) | 88 (21.2%) |
| Alopecia | – | – | 121 (50.8%) | – | – | – | – | – | – | – | – | – | 121 (29.2%) | – |
| Diarrhea | 5 (23%) | 0 | 67 (28.2%) | – | 13 (26%) | 0 | 7 (20%) | 0 | 25 (62.5%) | 1 (2.6%) | 10 (32.3%) | 0 (0%) | 127 (30.6%) | 1 (0.2%) |
| Decreased neutrophil count | 4 (18%) | 3 (14%) | 99 (41.6%) | 64 (26.9) | – | – | 12 (34%) | 4 (11%) | – | – | 5 (16.1%) | 5 (16.1) | 120 (28.9%) | 76 (18.3%) |
| Decreased platelet count | 6 (27) | 2 (9%) | 71 (29.8%) | 14 (5.9%) | – | – | 25 (72%) | 10 (29%) | – | – | 9 (29.1%) | 2 (6.5%) | 111 (26.7%) | 28 (6.7%) |
| Vomiting | 8 (36%) | 0 | 61 (25.6%) | – | 8 (16%) | 0 | 14 (35%) | 1 (2.6%) | 6 (19.4%) | 0 (0%) | 97 (23.4%) | 1 (0.2%) | ||
| Anorexia | 5 (23%) | 0 | 55 | – | 12 (24%) | 1 (2%) | 5 (14%) | 0 | 16 (40%) | 6 (15%) | – | – | 93 (22.4%) | 7 (1.7%) |
| Constipation | 5 (23%) | 0 | 78 (32.8%) | – | – | – | – | – | – | – | – | – | 83 (20.0%) | 0 |
| Cough | 7 (32%) | 0 | – | – | – | – | – | – | – | – | – | – | 7 (1.7%) | 0 |
| Palpitations | 7 (32%) | 0 | – | – | – | – | – | – | – | – | – | – | 7 (1.7%) | 0 |
| Neuropathy peripheral | – | – | 60 (25.2%) | – | 2 (4%) | 0 | – | – | – | – | – | – | 62 (14.9%) | 0 |
| Peripheral sensory neuropathy | – | – | 60 (25.2%) | – | 1 (2%) | 0 | – | – | – | – | – | – | 61 (14.7%) | 0 |
| Arthralgia | – | – | 58 (24.4%) | – | – | – | – | – | – | – | – | – | 58 (14.0%) | 0 |
| Decreased white blood cell count | 2 (9%) | 1 (5%) | 48 | 15 (6.3%) | 2 (4%) | 1 | 4 (12%) | 0 | – | – | – | – | 56 (13.5%) | 17 (4.1%) |
| Urinary tract infection | – | – | 48 (20.2%) | – | – | – | – | – | – | – | – | – | 48 (11.6%) | 0 |
| Hypertension | 2 (9%) | 1 (5) | – | – | 2 (4%) | 0 | – | – | 31 (77.5%) | 13 (33.3%) | – | – | 35 (8.4%) | 14 (3.4%) |
| Abdominal pain | 4 (18%) | 0 | – | – | 3 (6%) | 0 | – | – | 10 (33.3%) | 1 (2.6%) | – | – | 17 (4.1%) | 1 (0.2%) |
| Dyspnea | 13 (59%) | 2 (9%) | – | – | – | – | – | – | – | – | – | 13 (3.1%) | 2 (0.4%) | |
| Dizziness | 9 (41%) | 0 | – | – | 2 | 0 | – | – | – | – | 4 (12.9) | 0 | 9 (2.2%) | 0 |
| Creatinine increased | 7 (32%) | 9 (41%) | – | – | – | – | – | – | – | – | – | – | 7 (1.7%) | 9 |
| Myalgia | 5 (23%) | 1 (5%) | – | – | – | – | – | – | – | – | – | – | 5 (1.2%) | 1 (0.2%) |
| Bloating | 5 (23%) | 0 | – | – | – | – | – | – | – | – | – | – | 5 (1.2%) | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPARP inhibition in cancer therapy · Endometrial and Cervical Cancer Treatments · Colorectal and Anal Carcinomas
Introduction
Endometrial cancer (EC) is the most common gynecological malignancy in developed countries, with a majority of cases occurring postmenopause (1). Over the past decade, the prevalence of EC and disease-associated mortality rates has been continuously rising worldwide (1, 2). The prognosis of patients with primary advanced EC is poor, and available therapeutic options are limited. At the moment, no standard therapy has been globally accepted as the standard of care for advanced and recurrent EC after the failure of platinum-based chemotherapy.
Since the proposal of molecular subgroups based on the analysis of the Cancer Genome Atlas (TCGA) in 2013, it has played a crucial role in formulating the most appropriate therapy and identifying prognostic factors (3). More recently, monotherapy with an immune checkpoint inhibitor (ICIs), including antiprogrammed death 1 (PD-1) and antiprogrammed death ligand-1 (PD-L1), has demonstrated a substantial improvement in oncologic outcomes in patients with deficient mismatch repair (MMRd) EC (4, 5). Although several trials highlighted the limited efficacy of anti-PD-1/PD-L1 agents alone, combined therapy of PD-1/PD-L1 inhibitors and antiangiogenic agents is an attractive approach in proficient mismatch repair (pMMR) EC (6, 7).
In 2009, a phase I study presented the first clinical evidence of olaparib, a PARP inhibitor, having antitumor activity in patients associated with breast cancer (BRCA)1/2 mutations (8). In patients without BRCA mutations, the therapeutic value of PARP inhibitors is associated with homologous recombination deficiency (HRD) (9). Defects in homologous recombination repair (HRR) genes, including BRCA1/2, BRIP1, and RAD51C, have the potential to produce HRD (10, 11). A systematic review reported that BRCA1/2 pathogenic variants were identified in 4.3% of EC patients (10). In a large-scale study of molecular profiles of 1,475 EC cases, pathogenic variants in HRR genes were observed in 34.4% of cancers (12). Finally, alterations in the phosphatase and tensin homolog (PTEN) gene occur in up to 78% of EC (13). In preclinical studies, loss of PTEN is associated with HRD, sensitizing tumors to PARP inhibitors (14).
Although several clinical trials have either been completed or are ongoing, evidence supporting the PARP inhibitors, alone or in combination with other drugs, in advanced EC still remains limited. Currently, the majority of relevant studies are phase II clinical trials with small sample sizes. As such, this meta-analysis aimed to synthesize the available data to investigate the effectiveness and safety of PARP inhibitors for the treatment of advanced or recurrent EC.
Materials and methods
Search strategy and selection criteria
This systematic review was conducted and reported in accordance with the PRISMA 2020 guidelines. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 checklist is presented in the Supplementary materials. Electronic databases (PubMed, Embase, Web of Science, and Cochrane databases) were searched from inception up to 25 November 2025. Search terms included (“PARP inhibitor” OR “PARPi” OR “poly ADP-ribose polymerase inhibitor” OR “olaparib” OR “rucaparib” OR “veliparib” OR “niraparib” OR “talazoparib”) AND (“endometrial cancer” OR “endometrial carcinoma” OR “endometrium cancer” OR “endometrial neoplasms” OR “endometrial neoplasms”). In addition, references of related articles were searched to identify other relevant publications.
The inclusion criteria for studies in this meta-analysis were as follows: (1) patients diagnosed with advanced or recurrent EC who underwent treatment with a PARP inhibitor either alone or combined with PD-1/PD-L1 inhibitor or antiangiogenic agents; (2) studies with adequate clinical information, including the name of the medication used, the total number of patients, objective response rate (ORR), progression-free survival (PFS), overall survival (OS), and occurrence of adverse events (AEs); (3) study designs including cohort studies, case–control studies, randomized controlled trials (RCTs), or single-arm trials. For studies reporting on the same populations, we included the most recent results. The principal investigator (HH Z) and the second author (GW Y) independently scrutinized eligibility criteria and extracted study characteristics. This meta-analysis was registered in PROSPERO (registration number: CRD42024556356).
Data extraction and quality assessment
We summarized the characteristics of selected publications, including first author, year of publication, study phase, ClinicalTrials.gov identifier, follow-up time, total number of participants, PFS, OS, ORR, and AEs. For studies involving multiple tumors, only the endometrial cancer subset was included. The quality of the evidence was assessed using the Cochrane risk-of-bias tool (RoB 2) for randomized trials (RCTs) and the risk of bias in nonrandomized studies of interventions (ROBINS-I).
Statistical analysis
The median times and hazard ratios (HRs) for OS and PFS, with their 95% confidence intervals (95% CI), were extracted from the included clinical trials. Pooled estimates of both efficacy and safety outcomes were calculated when ≥ 2 clinical trials reported the results of the same prespecified outcome. Specifically, pooled estimates were calculated using the inverse variance method (metamean for PFS/OS, metaprop with logit transformation for ORR and AEs; metagen for log HRs for PFS/OS). The combined odds ratio (OR) and 95% CI were converted to an incidence rate to assess the ORR of PARP inhibitors. p < 0.05 for the Cochran Q estimates or I^2^ > 50% was considered to indicate high heterogeneity, and the random-effects model was applied; otherwise, the fixed-effects model was used. The effect model and heterogeneity statistics for each analysis are shown in Table 1. Publication bias was not assessed due to the small number of clinical trials (< 10) included (15). Sensitivity analysis was performed to assess the influence of the DUO-E trial and RUBY trial on the meta-analysis results. p < 0.05 was considered to indicate a statistically significant difference. Statistical analysis was performed using the “meta” package in R software.
Results
Study selection and characteristics
The literature search process is shown in Figure 1. Based on the inclusion criteria, 12 clinical trials including a total of 1,594 patients diagnosed with advanced or recurrent EC were included in this meta-analysis (Table 2). (16–26). All studies were published between 2021 and 2025. These studies included one clinical phase Ib trial, nine phase II trials, and two phase III trials. Specifically, five trials investigated the combination of PARP with PD-L1/PD-1 inhibitors, and two trials investigated the combination with an antiangiogenesis agent. Two trials examined both PARP inhibitor monotherapy and combination therapy (17, 21). Data from the combination therapy were used for the analysis.
PRISMA flow diagram illustrating the literature selection process.
The methodological assessment of the included studies is presented in Supplementary Table S1. Overall, a low to moderate risk of bias was observed in most included articles. Only one study was found to present a high risk of bias in the selection of participants (Supplementary Table S1; Supporting information).
Progression-free survival and overall survival
The duration of follow-up time ranged from a median of 7.4 to 31.9 months. PFS was reported in nine included studies. Among these, Madariaga et al. reported the lowest PFS of 2.4 months (95% CI = 1.6–3.7) (17), while Westin et al. reported the highest PFS of 15.1 months (95% CI = 12.6–20.7) (18). The pooled median PFS was 6.43 months (95% CI = 3.54–9.33) (Figure 2A). In the intention-to-treat population, no PFS difference was observed between PARP inhibitor monotherapy and placebo (HR = 0.684 [95% CI = 0.334–1.398], p > 0.05; Figure 2C). However, the combination of PARP with PD-L1/PD-1 inhibitors significantly prolonged PFS versus placebo (HR = 0.567 [95% CI = 0.469–0.686], p < 0.05; Figure 2D).
Forest plot of PFS for PARP inhibitor combination therapy in advanced or recurrent EC. (A) Overall population; (B) PARP inhibitors combined with PD-1/PD-L1 inhibitors; (C) PARP inhibitor monotherapy vs. placebo; (D) PARP combined with PD-L1/PD-1 inhibitors vs. placebo; (E) PFS6.
Based on the subgroup analysis, the pooled median PFS was 7.59 months (95% CI = 2.06–13.11) for advanced or recurrent EC patients who received combined therapy with a PD-1/PD-L1 inhibitor (Figure 2B). In addition, the pooled median PFS at 6 months was 0.44 (95% CI = 0.143–0.737), based on the analysis of four included studies (Figure 2E).
To further elucidate the high heterogeneity, a sensitivity analysis was performed excluding the phase III DUO-E trial and RUBY trial (18). Exclusion of the DUO-E trial significantly decreased the heterogeneity, and the pooled median PFS was 4.10 (95% CI = 3.09–5.10) and 2.972 (95% CI = 2.121–3.824) for the overall population and for patients who received the combined therapy with a PD-1/PD-L1 inhibitor, respectively (Supplementary Figure S1). Although the number of studies was limited, the studies in the funnel plot were symmetrically distributed with respect to the pooled estimate, suggesting no publication bias (Supplementary Figure S2).
OS data were reported in seven included studies; however, median OS was not reached in three studies. Among the included studies, Post et al. reported the lowest OS at 8.0 months (95% CI = 7.5–14.3) (19), while Westin et al. reported the highest OS as not reached (95% CI = not reached–not reached) (18). The pooled median OS was 11.837 months (95% CI = 3.124–20.549) (Figure 3A). In the intention-to-treat population, there was no OS difference between olaparib and placebo (HR = 0.787 [95% CI = 0.279–2.219], p > 0.05; Figure 3B).
Forest plot of OS for PARP inhibitor combination therapy in advanced or recurrent EC. (A) Overall population; (B) PARP inhibitor monotherapy vs. placebo.
Objective response rate
ORR data were reported in eight included studies. The pooled ORR was 0.17 (95% CI = 0.123–0.219) (Figure 4A). Among these studies, Post et al. reported the lowest ORR (8%) (19), while Westin et al. reported the highest ORR (44.0%) (18). Based on subgroup analysis, the pooled ORRs were 0.138 (95% CI = 0.072–0.203) and 0.227 (95% CI = 0.064–0.389) for advanced or recurrent EC patients who received combined therapy with PD-1/PD-L1 inhibitor and antiangiogenesis agent, respectively (Figure 4B). In addition, ORR was notably elevated in the combined therapy group compared with PARP inhibitor monotherapy (OR = 3.34 [95% CI = 1.095–10.165], p = 0.034) (Figure 4C).
Forest plot of ORR for PARP inhibitor combination therapy in advanced or recurrent EC. (A) Overall population; (B) patients receiving combination therapy with PD-1/PD-L1 inhibitor and antiangiogenesis agent; (C) PARP inhibitor monotherapy versus combination therapy.
Adverse effects
Only six included studies provided available AEs data, and the occurrence of AEs of any grade was analyzed in two studies. The overall pooled proportion of AEs was 0.947 (95% CI = 0.835–1.000) (Supplementary Figure S3A). AEs of grade ≥ 3 were analyzed in two studies. The overall pooled proportion of AEs of grade ≥ 3 was 0.72 (95% CI = 0.603–0.838) (Supplementary Figure S3B).
Details of AEs are summarized in Table 3. The most common AEs included fatigue (226, 54.5%), nausea (219, 52.8%), anemia (219, 52.8%), diarrhea (127, 30.6%), and alopecia (121, 29.2%). When considering only AEs of grade ≥ 3, patients had a higher incidence of anemia (88, 21.2%), decreased neutrophil count (76, 18.3%), fatigue (31, 7.5%), decreased platelet count (28, 6.7%), and decreased white blood cell count (17, 4.1%).
Discussion
This is an up-to-date meta-analysis on the efficacy and safety of PARP inhibitors for patients with advanced or recurrent EC. We included 12 studies with a total of 1,594 patients, and the most reliable comparative information comes from the HRs of randomized trials. The main findings from the pooled analyses were as follows: (1) the results showed that the combination of PARP and PD-L1/PD-1 inhibitors could significantly prolong PFS versus placebo; (2) in the intention-to-treat population, there was no PFS/OS difference between PARP inhibitor monotherapy and placebo; (3) the ORR was notably elevated in the combined therapy group compared with PARP inhibitor monotherapy; and (4) the most common AEs included fatigue (226, 54.5%), nausea (219, 52.8%), anemia (219, 52.8%), diarrhea (127, 30.6%), and alopecia (121, 29.2%).
Recently, novel immunotherapeutic strategies have been proposed to enhance clinical efficiency. PARP inhibitors are among the most promising agents and have already demonstrated compelling results in ovarian cancer (28). Furthermore, as it has been reported that the accumulation of DNA damage caused by PARP inhibitors may reverse the immune escape by upregulating PD-L1, combining PD-1/PD-L1 inhibitors with PARP inhibitors is an attractive approach for EC patients (28). Our study suggests that the combination of PARP with PD-L1/PD-1 inhibitors could significantly prolong PFS versus placebo for advanced or recurrent EC patients, and ORR was notably elevated in the combined therapy group compared with PARP inhibitor monotherapy. Studies investigating PD-1/PD-L1 inhibitor monotherapy in MMRd EC revealed a median PFS ranging from 4.4 to 25.7 months, along with an ORR of 26.7% to 57.1% (5, 29, 30,), which were better than those reported in this meta-analysis. The outcomes of our study appear better than those of studies involving PD-1/PD-L1 inhibitors in pMMR EC, which indicated a median PFS of 1.8 to 1.9 months and an ORR of 3.0% to 13.4% (4, 29, 30). Several previous studies have found that the combination of PARP inhibitors, such as olaparib and niraparib, with PD-1/PD-L1 inhibitors might have modest clinical effects (17–19). The addition of the anti-PD-L1 antibody durvalumab with olaparib to platinum-based chemotherapy significantly improved PFS for patients with advanced or recurrent EC compared to durvalumab or chemotherapy alone, demonstrating a potential role for PARP inhibitors (18).
The efficacy of PARP inhibitors was also tested in association with other drugs, such as antiangiogenesis and AKT inhibitors (16, 21, 22). Some studies demonstrate that chronic hypoxia induced by antiangiogenic agents, such as bevacizumab, can lead to HRD within tumors, potentially enhancing sensitivity to PARP inhibitors (16, 31, 32). The combination of antiangiogenic agents with PARP inhibitors has also been assessed in a phase II trial (NCT03660826) (20). In this three-arm randomized trial, PFS was 3.8 months for cediranib alone, 2 months for olaparib, and 5.5 months for olaparib and cediranib. However, the between-arm differences were not statistically significant (20). In this meta-analysis, we included two trials that investigated the combination of antiangiogenic agents with PARP inhibitors. The pooled ORR was found to be 0.138 (95% CI = 0.072–0.203) for advanced or recurrent EC, which is similar to that observed with the combined therapy including a PD-1/PD-L1 inhibitor.
While generally manageable with successful management strategies, AEs occurred more frequently and remain a significant concern with combination immunotherapies. The results of this study indicated that the most commonly reported AEs of any grade included fatigue (226, 54.5%), nausea (219, 52.8%), anemia (219, 52.8%), diarrhea (127, 30.6%), and alopecia (121, 29.2%). Although the frequency of adverse events is typically higher in combination chemotherapies, grade ≥ 3 AEs were reported with low incidence, with the most frequent being anemia (88, 21.2%), decreased neutrophil count (76, 18.3%), fatigue (31, 7.5%), decreased platelet count (28, 6.7%), and decreased white blood cell count (17, 4.1%).
In the phase III DUO-E trial, the overall incidence of treatment-emergent AEs of grade ≥ 3 in the control, durvalumab, and durvalumab + olaparib arms was 56.4%, 54.9%, and 67.2%, respectively (18). Although there was a higher rate of AEs of grade ≥ 3 in the durvalumab + olaparib arm, the safety profiles were generally consistent with the known profiles of the individual components of the regimen (18). However, in the phase II DOMEC trial (19), the combination of durvalumab and olaparib was well tolerated, with no new safety profiles observed, consistent with those in previous studies (19, 29, 30).
Targeted therapies, such as olaparib, which inhibit PARP, induce synthetic lethality in tumor cells harboring HRD. The percentage of BRCA-mutated endometrial cancers is very low; therefore, HRD is an emerging concept in EC and appears to play a role in its pathogenesis. HRD is largely restricted to TP53-mutated ECs, and approximately 20%–40% of p53-abnormal tumors harbor HRD. The UTOLA trial suggests that olaparib may provide the greatest PFS benefit in the population with TP53 mutations (25).
For patients with pMMR disease, the magnitude of PFS benefit is lower, and the efficacy of PD-1 and PD-L1 inhibitors is variable. In the recurrent setting, the combination of pembrolizumab and lenvatinib is a promising therapeutic option for the pMMR/microsatellite-stable (MSS) subset, despite the significant morbidity associated with this pharmacological regimen. Moreover, exploratory subgroup analyses of the DUO-E trial suggest that the addition of maintenance olaparib to the combination of durvalumab plus chemotherapy may improve outcomes in the pMMR and PD-L1–positive patient populations (25). Consequently, assessing PD-L1 expression in recurrent pMMR/MSS cases could help identify patients who might benefit from the combination of PARP with ICIs (33).
There has been strong interest in utilizing a PARP inhibitor alone or in combination with other agents for managing EC. Several ongoing trials are testing the safety and effectiveness of PARP inhibitors in combination with chemotherapy (e.g., NCT04159155, NCT03603184), ICI (e.g., NCT04269200, NCT03016338, NCT03981796), and antiangiogenics (e.g., NCT03660826). Moreover, further biomarker-driven trials aimed at guiding the therapeutic selection and testing targeted agents are warranted.
This research has several limitations. First, owing to restricted data availability, subgroup analyses based on factors such as MMR status, PD-L1 expression, BRCA mutation, and HRD status were not feasible. Second, several clinical trials have not yet reached their final OS endpoints; thus, our OS analyses are based on a limited number of immature datasets and should be interpreted with caution. Updated analyses will be needed once these trials mature. Third, the majority of included trials were nonrandomized, single-arm, and unblinded, and therefore carried high risks of selection bias and performance bias. Further large-scale RCTs are required to confirm these results.
Conclusion
In conclusion, our study provided preliminary evidence that the combination of PARP inhibitors with PD-L1/PD-1 inhibitors exhibits modest activity accompanied by substantial toxicity, particularly in heavily pretreated and predominantly pMMR advanced or recurrent EC. Definitive conclusions regarding survival benefits, however, require further phase III data and biomarker-driven analyses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel RL Miller KD Wagle NS Jemal A . Cancer statistics 2023. CA Cancer J Clin. (2023) 73:17–48. doi: 10.3322/caac.21763, PMID: 36633525 · doi ↗ · pubmed ↗
- 2Makker V Mac Kay H Ray-Coquard I Levine DA Westin SN Aoki D . Endometrial cancer. Nat Rev Dis Primers. (2021) 7:88. doi: 10.1038/s 41572-021-00324-8, PMID: 34887451 PMC 9421940 · doi ↗ · pubmed ↗
- 3Cancer Genome Atlas Research Network Kandoth C Schultz N Cherniack AD Akbani R Liu Y . Integrated genomic characterization of endometrial carcinoma. Nature. (2013) 497:67–73. doi: 10.1038/nature 12113, PMID: 23636398 PMC 3704730 · doi ↗ · pubmed ↗
- 4Antill Y Kok PS Robledo K Yip S Cummins M Smith D . Clinical activity of durvalumab for patients with advanced mismatch repair-deficient and repair-proficient endometrial cancer. A nonrandomized phase 2 clinical trial. J Immunother Cancer. (2021) 9:e 002255. doi: 10.1136/jitc-2020-002255, PMID: 34103352 PMC 8190057 · doi ↗ · pubmed ↗
- 5O’Malley DM Bariani GM Cassier PA Marabelle A Hansen AR De Jesus Acosta A . Pembrolizumab in patients with microsatellite instability-high advanced endometrial cancer: results from the KEYNOTE-158 study. J Clin Oncol. (2022) 40:752–61. doi: 10.1200/JCO.21.01874, PMID: 34990208 PMC 8887941 · doi ↗ · pubmed ↗
- 6Makker V Colombo N Casado Herráez A Santin AD Colomba E Miller DS . Lenvatinib plus pembrolizumab for advanced endometrial cancer. N Engl J Med. (2022) 386:437–48. doi: 10.1056/NEJ Moa 2108330, PMID: 35045221 PMC 11651366 · doi ↗ · pubmed ↗
- 7Makker V Aghajanian C Cohn AL Romeo M Bratos R Brose MS . A phase ib/II study of lenvatinib and pembrolizumab in advanced endometrial carcinoma (Study 111/KEYNOTE-146): long-term efficacy and safety update. J Clin Oncol. (2023) 41:974–9. doi: 10.1200/JCO.22.01021, PMID: 36608305 PMC 9928628 · doi ↗ · pubmed ↗
- 8Fong PC Boss DS Yap TA Tutt A Wu P Mergui-Roelvink M . Inhibition of poly(ADP-ribose) polymerase in tumors from BRCA mutation carriers. N Engl J Med. (2009) 361:123–34. doi: 10.1056/NEJ Moa 0900212, PMID: 19553641 · doi ↗ · pubmed ↗