Efficacy of psychosensory interventions for the management of pediatric pain, fear, and distress during emergency care: a systematic review and meta-analysis of randomized clinical trials
Mariela Bustamante Fernández, Line Caes, José Iván Rossel, Genesis Díaz Díaz, Gabriela Ruiz Valenzuela, Scarlett Caroca Madariaga, Nicole Klein Vallecillo, Sofía Hidalgo Vilche, Valeska Tapia Espinoza, Mariana González Zamarin, Katherine Strasser

TL;DR
This study reviews how psychological and sensory techniques can help reduce pain and fear in children during emergency medical procedures.
Contribution
The study provides a systematic review and meta-analysis of randomized trials on psychosensory interventions in pediatric emergency care.
Findings
Psychosensory interventions significantly reduced self-reported and observed pain and fear in children.
Pre-procedural informational videos and somato-sensory distraction were the most effective strategies.
High heterogeneity in results suggests variability in intervention effectiveness across studies.
Abstract
The experience of invasive medical procedures (IMP) in pediatric emergency departments (PEDs) is often highly stressful for children and adolescents and potentially leads to short- and long-term biopsychosocial consequences. To address these challenges, psychological and sensory strategies have been developed to mitigate negative outcomes and enhance children's adaptive coping PEDs. To evaluate the efficacy of psychological and sensory interventions on pediatric pain, fear, and distress during PEDs. A systematic review and meta-analysis were conducted following the PRISMA 2020 Statement (PROSPERO registration: CRD42023403583). Searches were performed in PubMed, PsycInfo, CINAHL, SCOPUS, and Web of Science for studies published between January 2004 and September 2024. Randomized controlled trials involving children aged 2–18 years undergoing IMPs in PEDs. The qualitative synthesis and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
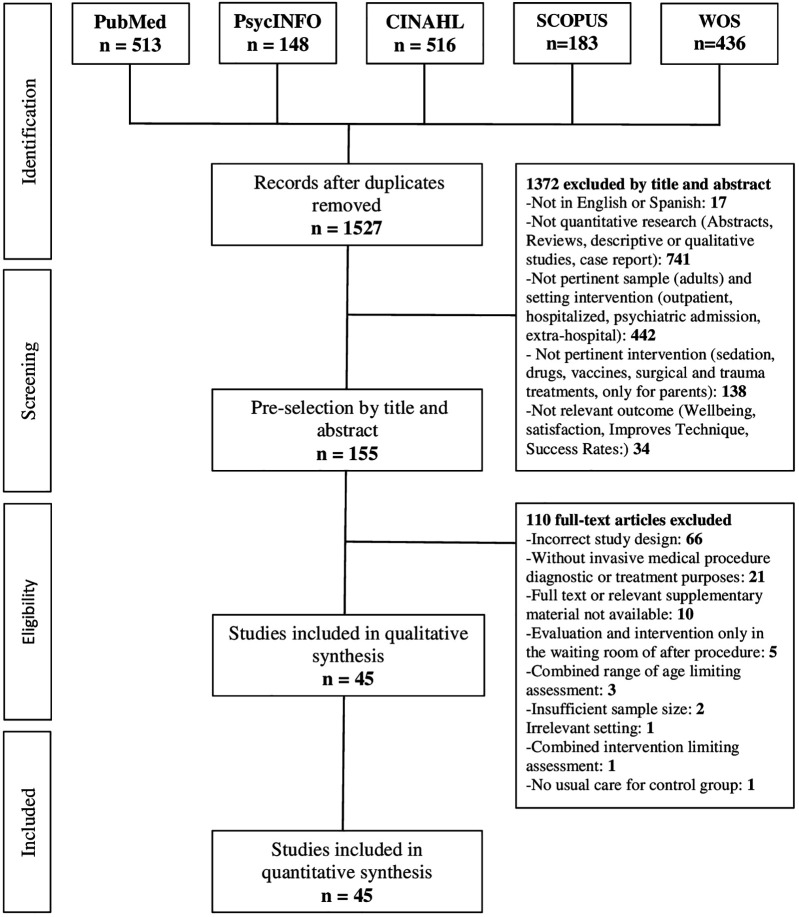 Figure 1
Figure 1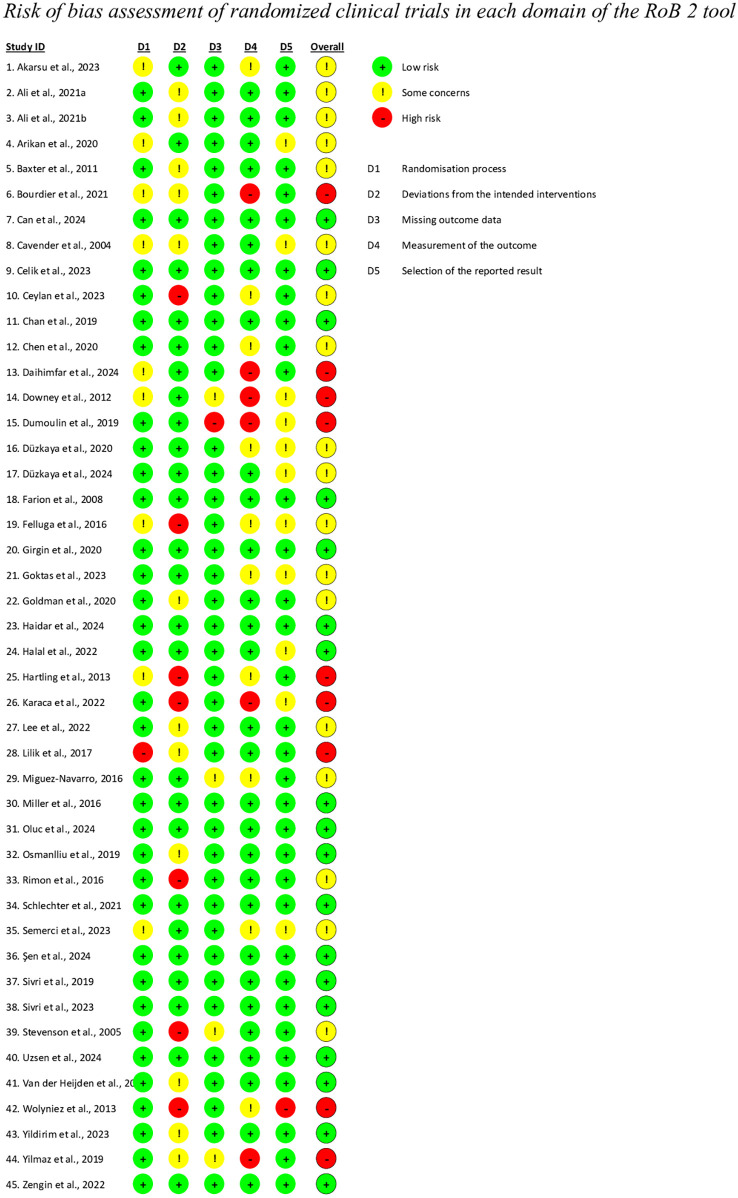 Figure 2
Figure 2| Author | Sample & Country | Objective | Main Intervention | Specific intervention | Timing | Control | Outcomes and Measured | Results |
|---|---|---|---|---|---|---|---|---|
| Akarsu, Semerci, and Kılınç, 2023 ( | 159 (5 to 12 years) | Compare the effects of watching cartoons with VR and tablet on pain, fear, and anxiety during venipuncture | Screen-Based and Immersive Reality | Video with VR Glasses (Group 1). Cartoon on Portable Device (Group 2) | Before and During | Usual procedure. Standard parental support. | Pain (WB-FACES) and Fear (CFS). Self-Reported and Observer | VR and Cartoon were effective in reducing self-reported pain ( |
| Ali et al., 2021a ( | 86 (6 to 11 years) M = 9/SD = 2.22 Boys: 60.5% Girls: 48.8%. Canada | Evaluate the effectiveness of a humanoid robot to reduce stress and pain during intravenous cannulation | Social Interaction | Robot Coach | Before, During, and After | Usual procedure. Standard parental support. | Self-Reported Pain (FPS-R), Behavioral Distress (OSBD-R) | Robot intervention showed a significant difference compared control in distress ( |
| Ali et al., 2021b ( | 86 (6 to 11 years) M = 7/SD = 2.96 Boys: 52.9% Girls: 47.1%. Canada | Compare the effectiveness of using an iPad vs. standard care on pain and distress during intravenous cannulation | Screen-Based | Cartoon on Portable Device (Group 1). | Before and during | Usual procedure. Standard parental support. The nurse used usual calming verbalization | Self-Reported Pain (FPS-R), Behavioral Distress (OSBD-R), Biological Marker: HR. | No significant differences were found in pain (Control/iPad: |
| Arikan and Esenay, 2020 ( | 216 (6 to 12 years) | Examine the effects of active and passive distraction on pain, fear, and anxiety during blood sampling | Toy-Based Distractions | Interaction with Rotating Toy (Group 1) and Musical Bracelet (Group 2) | During | Usual procedure. Standard parental accompaniment | Self-Reported Pain (WB-FACES/VAS), and Fear (CFS). | Both the active and passive distraction groups significantly reduced pain for VAS (Active/Passive/Control: |
| Baxter et al., 2011 ( | 81 (4 to 18 years) M = 10.01/SD = 0.95 | Compare a reusable cold and vibration device with standard care to alleviate pain from pediatric venous access | Somato-Sensory | Buzzy or Vibration (Group 1). | During | Usual procedure. Standard parental accompaniment | Pain self-reported and observed (FPS-R), Behavioral Distress (OSBD-R). | Significant differences between Buzzy and control for self-reported pain ( |
| Bourdier et al., 2021 ( | 607 (1,5 to 6 years) M = 3.7/SD = 1.12 | Evaluate differences in pain-related behavior during cannulation between the buzzy device and standard care | Somato-Sensory | Buzzy or Vibration (Group 1). | During | Usual procedure. Standard parental accompaniment. EMLA patch | Behavioral Distress (CHEOPS). | Control group had lower distress scores than those in the Buzzy group (Control/Buzzy: |
| Can et al., 2024 ( | 160 (4 to 10 years) | Evaluate the effect of Veinlite PEDI2 (VID) and VR on emotional behavior, pain, fear, and anxiety | Unisensory Distractions | VID (Group 1), Video with VR Glasses (Group 2), and Video VR Glasses + VID (Group 3) | Before, during, and after | Usual procedure. Standard parental accompaniment | Self-reported Pain (WB-FACES/CAS) and Fear (CFS). | Significant differences were found for WB-FACES pain (Control/VID/VR/VID + VR: |
| Cavender et al., 2004 ( | 43 (4 to 11 years) M = 7.89/SD = 1.74 | Determine the effectiveness of parental involvement using positioning and distraction to reduce pain, fear, and distress during venipuncture | Social Interaction | Parental Positioning and Distraction (Group 1). | Before, during, and after | Usual procedure. Standard parental accompaniment. | Pain (WB-FACES) and Fear (GFS) self-reported Behavioral Distress (PBCL). | The intervention group did not show significant differences compared the control in pain ( |
| Celik et al., 2023 ( | 96 (7 to 15 years) M = 10.67/SD = 2.86 | Determine the effect of cold spray and ice applied during venipuncture on the level of fear and pain in children | Somato-Sensory | Cold Spray (Group 1) and Ice Gel (Group 2) | Before and during | Usual procedure. Standard parental accompaniment | Pain (VAS) and Fear (CFS) Self-reported and observed. | Cold Spray significantly reduced both pain and fear, both self-reported and observed, compared to Cuidado Usual (Pain: |
| Ceylan and Erkut, 2023 ( | 80 (3 to 6 years) | Determine the effect of distraction with a finger puppet during venous blood sampling on children’s pain and emotional manifestation | Social Interaction | Finger Puppet (Group 1). | Before and during | Usual procedure. Standard parental accompaniment | Behavioral Distress (CEMS) | Distress measures were statistically lower in the experimental group (Puppet/Control: |
| Chan et al., 2019 ( | 252 (4 to 11 years) | Evaluate the efficacy and safety of VR distraction for needle pain in the emergency department and outpatient settings | Immersive Reality | Video with VR Glasses (Group 1). | Before and during | Usual procedure. Standard parental accompaniment. age-appropriate distractions | Self-reported Pain (FPS-R) and Fear (VAT). | VR significantly reduced both pain (VR/Control: |
| Chen et al., 2020 ( | 136 (7 to 12 years) | Examine the effects of VR on pain and fear in school-aged children during intravenous injection | Immersive Reality | Video with VR Glasses (Group 1). | During | Usual procedure. Standard parental accompaniment | Pain (WB-FACES), Fear (CFS), both self-reported and observed. | VR intervention significantly reduced for fear observed VR/Control: |
| Daihimfar et al., 2024 ( | 180 (3 to 6 years) M = 4.36/SD = 0.66 | Compare the effects of acupressure and music therapy on venipuncture pain intensity in children | Unisensory Distractions | Music Therapy (Group 1) and Acupressure | Before and during | Usual procedure. Standard parental accompaniment | Self-reported Pain (Oucher Scale). | The lowest mean pain score was in the music therapy group, and the highest in the control group (Music/Acupressure/Control: |
| Downey et al., 2012 ( | 100 (3 to 18 years) | Determine if watching cartoons in an acute care setting reduces pain perception in children | Screen-Based | Cartoons on Tablet or Portable DVD Player (Group 1). | During | Usual procedure. Standard parental accompaniment | Self-reported Pain (FPS-R). | Pain score differences during the procedure were minimal (Cartoons: |
| Dumoulin et al., 2019 ( | 177 (8 to 17 years) | Compare the efficacy of VR during a medical procedure with two other conditions: watching television and CLS | Immersive Reality | Video Game with VR (Group 1) and Cartoons on Tablet or Portable DVD Player (Group 2) | During | Usual procedure. Standard parental accompaniment. The CLS program | Self-reported Pain and Fear (VAS). | VR group was effective in reducing pain intensity (Cartoon: |
| Düzkaya et al., 2020 ( | 477 (6 to 12 years) | Compare the effects of watching a cartoon and an informational video on children’s pain and fear levels | Screen-Based | Cartoons on Tablet or Portable DVD Player (Group 1) and Informational Video (Group 2) | Before and during | Usual procedure. Standard parental accompaniment | Pain (WB-FACES), Fear (CFS), both self-reported and observed, Biological Markers: SpO2, HR, BP. | Informational video and cartoon groups had lower pain ( |
| Düzkaya et al., 2024 ( | 177 (6 to 12 years) | Determine the effects of ShotBlocker and the Helfer Skin Puncture technique on children’s pain and fear during intramuscular injection | Somato-Sensory | ShotBlocker (Group 1) and Helfer Skin Puncture (Group 2) | During | Usual procedure. Standard parental accompaniment | Pain (WB-FACES) Fear (CFS), both self-reported and observed. | Shockblocker had lowest scores for observed fear and pain ( |
| Farion et al., 2008 ( | 80 (6 to 12 years) M = 9.4/SD = 2.04 | Determine whether a new product, Pain Ease, would reduce pain during intravenous cannulation in children | Somato-Sensory | Cold Spray | Before | Standard parental accompaniment. Placebo aerosol. CLS distraction | Self-reported and Observed Pain (VAS). Caregivers, Nurses, and CLS. | Cold Spray showed lower pain compared to usual care, both in observed pain ( |
| Felluga et al., 2016 ( | 40 (4 to 11 years) M = 9.0/SD = 2.56 | Evaluate if the presence of medical clowns can reduce children’s anxiety and pain during painful procedures | Social Interaction | Medical Clowns (Group 1). | Before and during | Usual procedure. Standard parental accompaniment. Nurse distraction | Self-reported Pain (NRS/WB-FACES), Fear (CAPS). | No significant differences were found in pain between the control group ( |
| Girgin et al., 2020 ( | 90 (6 to 12 years) M = 9.3/SD = 1.5 | Compare the effects of ShotBlocker and Buzzy methods on pain, fear, and parental satisfaction during intramuscular injection | Somato-Sensory | Buzzy or Vibration (Group 1) and ShotBlocker | Before and during (Group 1), During (Group 2) | Usual procedure. Standard parental accompaniment | Pain (WB-FACES), Fear (CFS), both self-reported and observed. | Buzzy and ShotBlocker significantly reduced pain and fear. For observed and self-reported pain (Buzzy/ShotBlocker/Control: |
| Goktas and Avci, 2023 ( | 144 (7 to 12 years) | Determine the effects of visual and/or auditory distraction techniques during invasive procedures on pain, anxiety, and medical fear | Toy-Based Distractions Unisensory Distractions | Kaleidoscope (Group 1), Listening to Music (Group 2), and Video with VR Glasses (Group 3) | Before, during, and after | Usual procedure. Standard parental accompaniment | Pain (WB-FACES), Fear (CFS), self-reported. | Pain levels were significantly lower in the intervention groups (Kaleidoscope/Music/VR/Control: |
| Goldman and Behboudi, 2020 ( | 70 (6 to 16 years) M = 9.23/SD = 4.26 | Explore the role of VR in reducing pain and anxiety during intravenous catheterization, compared to standard treatment | Immersive Reality | Video with VR Glasses (Group 1) | Before, during, and after | Usual procedure. Standard parental accompaniment | Self-reported Pain (FPS-R) and Fear (VSAS) | VR group reported statistically significant lower pain scores compared to the control group ( |
| Haidar et al., 2024 ( | 300 (2 to 14 years) | Evaluate the effect of the Buzzy device on pain and anxiety compared to EMLA cream during intravenous cannulation or venipuncture | Somato-Sensory | Buzzy or Vibration (Group 1) | Before and during | Usual procedure. Standard parental accompaniment. Topical EMLA | Self-reported Pain (FPS-R), Behavioral Distress (FLACC). | Mean self-reported pain scores were lower in the EMLA control group than Buzzy ( |
| Halal et al., 2022 ( | 120 (3 to 6 years) M = 4.39/SD = 0.97 | Study the effect of the Buzzy device and whistling during blood sample collection on children’s pain and fear | Somato-Sensory | Buzzy or Vibration (Group 1) and Whistling (Group 2) | Before and during | Usual procedure. Standard parental accompaniment | Pain (WB-Faces), Fear (CMFS), both self-reported. | Pain showed statistically significant differences (Buzzy/Whistling/Control: |
| Hartling et al., 2013 ( | 42 (3 to 11 years) M = 5.92/SD = 3.29 | Compare music with standard care for managing pain and stress | Unisensory Distractions | Listening to Music (Group 1) | Before, during, and after | Usual procedure. Standard parental accompaniment | Self-reported Pain (FPS-R), Behavioral Distress (OSBD-R). Biological Marker: HR. | No significant difference was observed for pain (Control/Music: |
| Karaca and Guner, 2022 ( | 60 (4 to 6 years) | Analyze the effect of a musical and moving toy distraction method on fear and anxiety | Toy-Based Distractions | Musical and Dancing Toy (Group 1) | Before and during | Usual procedure. Standard parental accompaniment | Self-reported and Observed Fear (CFS). Biological Marker: SpO2, HR. | There were no statistically significant differences in self-reported (Musical toy/Control: |
| Lee et al., 2022 ( | 88 (6 months to 4 years) M = 1.92/SD = 1.70. Boys: 60.2% Girls: 39.8%. Canada | Determine whether a VR environment reduces distress among children during IV catheter placement compared to standard care | Screen-Based | Ceiling Virtual Reality Display (Group 1) | Before and during | Usual procedure. Standard parental accompaniment | Behavioral Distress (FLACC), Observed Pain (VAS) and Fear (VAS). | There were no statistically significant differences for distress levels (Control/VR screen: |
| Lilik et al., 2017 ( | 57 (3 to 6 years) | Evaluate the effectiveness of cartoon-patterned clothing and bubbles for alleviating pain and anxiety during venipuncture | Unisensory Distractions | Cartoon-patterned Clothes (Group 1) and Blowing Bubbles (Group 2) | During | Usual procedure. Standard parental accompaniment | Behavioral Distress (FLACC), Fear Self-Reported (CFS). | Significant differences were observed in self-reported fear and an approach to significance for distress levels. Mean scores for fear were Control/Blowing Bubbles/Simple Visual: |
| Miguez-Navarro, 2016 ( | 140 (3 to 11 years) | Investigate the efficacy of video distraction to reduce anxiety and pain in children undergoing venipuncture | Screen-Based | Cartoons on Tablet or Portable DVD (Group 1) | Before and during | Usual procedure. Parental presence was not allowed in the study group | Self-reported Pain (WB-FACES/NRS), Behavioral Distress (GDS) Biological Marker: HR. | Significantly lower levels of distress in the video distraction group (Video/Control: |
| Miller et al., 2016 ( | 98 (3 to 12 years) M = 6.73/SD = 2.71 | Examine which of the interventions most effectively reduces pain and distress in children during IV cannulation | Screen-Based | PSP-VG (Group 1), Ditto-D (Group 2), Ditto-P (Group 3), Ditto-C (Group 4) | Before, during, and after | Usual procedure. Standard parental accompaniment | Self-reported Pain (WB-FACES) and Observer-reported Pain (VAS), Behavioral Distress (FLACC). | Significant reductions in pain and distress only for observed measures. Self-reported pain were: Control/PSP/Ditto-D/Ditto-PP/Ditto-C: |
| Oluc et al., 2024 ( | 111 (6 to 12 years) | Evaluate the effects of two distraction methods on reducing pain and fear during phlebotomy | Active Command | Blowing Bubbles (Group 1) and Stress Balls (Group 2) | Before and during | Usual procedure. Standard parental accompaniment | Fear (CFS), Pain (WB-FACES), both self-reported and observed. | Significant differences were found in self-reported fear (Bubbles/Stress Balls/Control: |
| Osmanlliu et al., 2019 ( | 63 (7 to 17 years) M = 11.7/SD = 2.95 | Study the feasibility and acceptability of VR distraction for patient comfort during intravenous procedures | Immersive Reality | VR Video Game (Group 1) | Before and during | Usual procedure. Standard parental accompaniment | Self-reported Pain (NRS), and Fear (CFS), Behavioral Distress (PBCL). | No significant differences were found in pain scores (VR/Control: |
| Rimon et al., 2016 ( | 53 (2 to 15 years) M = 6.19/SD = 3.09 | Investigate whether clown medical interventions reduce distress and have an effect on cortisol during venipuncture | Social Interaction | Medical Clowns (Group 1) | Before, during, and after | Usual procedure. Standard parental accompaniment | Self-reported Pain (VAS). Biological Markers: Plasma Cortisol | The intervention with clowns significantly reduced pain scores (Clowns: |
| Schlechter et al., 2021 ( | 115 (4 to 17 years) | Evaluate the efficacy of VR distraction to increase the success of the first intravenous attempt | Immersive Reality | VR Video Game (Group 1) | Before and during | Usual procedure. Standard parental accompaniment. and distraction | Pain (FPS-R), Fear (LTAS) both self-reported and observed (Caregivers) | There were no significant differences for self-reported/observer pain (VR: |
| Semerci et al., 2023 ( | 161 (5 to 12 years) | Evaluate the efficacy of Buzzy and Cold Spray in reducing pain, anxiety, and fear during venipuncture | Somato-Sensory | Buzzy (Group 1) and Cold Spray | Before and during | Usual procedure. Standard parental accompaniment | Pain (WB-FACES), Fear (CFS), both self-reported and observed (Caregivers and health workers) | Cold Spray and Buzzy significantly reduced both observed and self-reported pain and fear ( |
| Şen et al., 2024 ( | 102 (7 to 12 years) | Evaluate the effect of VR glasses during IV catheter insertion on children’s emotional responses | Immersive Reality | Video with VR Glasses (Group 1) | During | Usual procedure. Standard parental accompaniment | Behavioral Distress (CEMS). | The VR group scored significantly lower than the control group (VR: |
| Sivri et al., 2019 ( | 150 (7 to 12 years) | Investigate the effect of Buzzy and ShotBlocker on reducing pain from intramuscular penicillin injections in children | Somato-Sensory | Buzzy or Vibration (Group 1) and ShotBlocker | Before and during | Usual procedure. Standard parental accompaniment | Pain self-reported (VAS/FPS-R). | Pain scores were significantly lower in Buzzy and ShotBlocker for both VAS/FPS-R (Control: |
| Sivri et al., 2023 ( | 242 (9 to 12 years) | Compare the effectiveness of Buzzy, ShotBlocker, and Distraction Cards in reducing pain and anxiety during venous blood sampling in children | Somato-Sensory | Buzzy or Vibration (Group 1), ShotBlocker (Group 2), and Distraction Cards (Group 3) | Before and during | Usual procedure. Standard parental accompaniment | Pain self-reported (VAS/FPS-R). | Pain was significantly higher in the control group, for VAS and FPS-R (Control: |
| Stevenson et al., 2005 ( | 149 (2 to 16 years) | Analyze the effect of CLS intervention during peripheral venous angiocatheter insertion on children’s suffering | Social Interaction | CLS (Group 1) | Before and during | Usual procedure. Standard parental accompaniment | Behavioral Distress (OSBD-R). | There was a significant reduction in distress in the CLS group ( |
| Uzsen et al., 2024 ( | 120 (5 to 10 years) | Evaluate the effects of Buzzy and Acupressure methods on children’s pain, fear, and anxiety levels during intramuscular injection | Somato-Sensory | Buzzy or Vibration (Group 1) and Acupressure | Before and during | Usual procedure. Standard parental accompaniment | Fear (CFS), Pain (WB-FACES), both self-reported and observed. | Buzzy and Acupressure significantly reduced pain and fear in both observed and self-reported measures. For pain, Control ( |
| Van der Heijden et al., 2019 ( | 191 (3 to 13 years) | Determine the effectiveness of music and cartoons in reducing pain and stress during emergency procedures | Screen-Based | Cartoons on Tablet or Portable DVD (Group 1) and Listening to Music (Group 2) | During | Usual procedure. Standard parental accompaniment | Self-reported Pain (FPS-R), Observed Pain (AHTPS), Behavioral Distress (OSBD-R). Health worker and Research Observer. HR. | Observed pain showed significant differences (Control/Cartoons/Music: |
| Wolyniez et al., 2013 ( | 47 (3 to 16 years) M = 7.45/SD = 4.0 | Evaluate the effect of therapeutic clowns on stress and anxiety levels during emergency procedures | Social Interaction | Medical Clowns (Group 1) | Before and during | Usual procedure. Standard parental accompaniment | Self-reported Pain (FPS-R; VAS). | There were no significant differences in pain for FPS-R/VAS (Control: |
| Yildirim et al., 2023 ( | 150 (4 to 10 years) | Determine whether using VR glasses or Buzzy during IV insertion improves first attempt success and reduces pain, fear, and anxiety levels | Immersive Reality | Video with VR Glasses (Group 1) and Buzzy (Group 2) | During and after | Usual procedure. Standard parental accompaniment | Self-reported Pain (WB-FACES; CAS), and Fear (CFS), Behavioral Distress (CEAS). Biological Markers: BP, RR, HR. | No significant differences were found in self-reported pain with WB or CAS (Control/VR/Buzzy: |
| Yilmaz et al., 2019 ( | 160 (5 to 10 years) | Compare the effectiveness of Buzzy, ShotBlocker, and Bubble Blowing in alleviating pain and fear during intramuscular injection | Somato-Sensory | Buzzy (Group 1), ShotBlocker (Group 2), and Bubble Blowing (Group 3) | Before and during | Usual procedure. Standard parental accompaniment | Pain (Oucher Scale), Fear (CFS), both self-reported and observed Caregiver and research observer. | Significant differences in both observed and self-reported ( |
| Zengin et al., 2022 ( | 224 (7 to 10 years) | Evaluate the effectiveness of ShotBlocker and Palm Stimulator in reducing pain associated with intramuscular injection | Somato-Sensory | ShotBlocker (Group 1) and Palm Stimulator (Group 2) | Before and during | Usual procedure. Standard parental accompaniment | Fear (CFS), Pain (VAS; FPS-R), both self-reported and observed-reported. Caregiver and research observer. |
| Intervention | Self-Reported Pain | Self-Reported Fear | Observed Pain | Observed Fear | Observed Distress | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Z | p | SMD + IC | Z | p | SMD + IC | Z | p | SMD + IC | Z | p | SMD + IC | Z | p | SMD + IC | |
|
|
|
|
|
|
|
|
|
|
|
|
|
| N. E | N. E | N. E |
| Blowing Soap Bubbles | 6.87 | <0.01 | −1.06 [−1.37, −0.76] | 9.41 | <0.01 | −1.57 [−1.90, −1.24] | 1.49 | 0.14 | −1.05 [−2.44, 0.34] | 4.41 | <0.01 | −1.73 [−2.50, −0.96] | 2.69 | <0.01 | −0.92 [−1.59, −0.25] |
| Palm Stimulator | 6.84 | <0.01 | −1.00 [−1.29, −0.71] | 0.10 | 0.92 | −0.02 [−0.40, 0.36] | 5.90 | <0.01 | −1.26 [−1.68, −0.84] | 0.25 | 0.80 | −0.05 [−0.43, 0.33] | N. E | N. E | N. E |
| Stress Ball | 4.56 | <0.01 | −1.15 [−1.64, −0.66] | 4.22 | <0.01 | −1.05 [−1.54, −0.56] | 5.83 | <0.01 | −1.56 [−2.08, −1.03] | 6.22 | <0.01 | −1.70 [−2.24, −1.17] | N. E | N. E | N. E |
| Whistling Breathing | 1.99 | 0.05 | −0.45 [−0.89, −0.01] | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E |
|
| |||||||||||||||
| Video Game with VR |
|
|
|
|
|
| N. E | N. E | N. E | N. E | N. E | N. E | 3.02 | < |
|
|
|
| < |
| 2.69 | <0.01 |
| N. E | N. E | N. E | N. E | N. E | N. E | 3.51 | < |
|
| Video VR Glasses | 3.89 | <0.01 | −0.91 [−1.36, −0.45] | 2.49 | 0.01 | −1.39 [−2.48, −0.29] | 1.42 | 0.16 | −1.38 [−3.29, 0.53] | 1.25 | 0.21 | −2.42 [−6.21, 1.37] | 4.66 | <0.01 | −0.84 [−1.19, −0.49] |
| Video VR Glasses + VID | 3.31 | <0.01 | −0.86 [−1.36, −0.35] | 2.17 | 0.03 | −0.49 [−0.94, −0.05] | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E |
|
|
|
|
|
|
|
|
| <0.01 |
|
| < |
|
|
|
|
|
|
|
|
| N. E | N. E | N. E |
| < |
| N. E | N. E | N. E |
| < |
|
| Ditto C | 0.94 | 0.34 | −0.30 [−0.94, 0.33] | N. E | N. E | N. E | 3.87 | <0.01 | −1.40 [−2.11, −0.69] | N. E | N. E | N. E | 1.32 | 0.19 | −0.43 [−1.06, 0.21] |
| Ditto-D | 1.29 | 0.20 | −0.41 [−1.04, 0.21] | N. E | N. E | N. E | 2.07 | 0.04 | −0.67 [−1.31, −0.04] | N. E | N. E | N. E | 2.16 | 0.03 | −0.71 [−1.35, −0.06] |
| Ditto-P | 0.06 | 0.95 | −0.02 [−0.65, 0.61] | N. E | N. E | N. E | 2.46 | 0.01 | −0.83 [−1.48, −0.17] | N. E | N. E | N. E | 1.43 | 0.15 | −0.46 [−1.10, 0.17] |
|
|
| < |
|
| < |
|
| < |
|
| < |
| N. E | N. E | N. E |
|
| 1.73 | 0.08 | −0.56 [−1.19, 0.08] | N. E | N. E | N. E | 1.98 | 0.05 | −0.64 [−1.28, −0.01] | N. E | N. E | N. E | 2.76 | <0.01 | −0.92 [−1.58, −0.27] |
|
| N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | 1.08 | 0.28 | −0.23 [−0.65, 0.19] |
|
|
| < |
| N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E |
| Distraction Cards | 5.40 | <0.01 | −0.72 [−0.98, −0.46] | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E |
| Listening to Music | 2.05 | 0.04 | −1.61 [−3.14, −0.07] | 6.47 | <0.01 | −1.83 [−2.39, −1.28] | N. E | N. E | N. E | N. E | N. E | N. E | 0.31 | 0.76 |
|
|
|
|
|
| N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E |
| Cartoon-Clothes | 2.19 | 0.03 | −0.74 [−1.40, −0.08] | 2.59 | 0.01 | −0.88 [−1.55, −0.21] | N. E | N. E | N. E | N. E | N. E | N. E | 2.19 | 0.03 |
|
| Vein Imaging Device | 0.00 | 1.00 | 0.00 [−0.31, 0.31] | 0.77 | 0.44 | −0.17 [−0.61, 0.27] | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E |
|
| |||||||||||||||
| Child Life Specialists | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | 0.72 | 0.47 | −0.12 [−0.46, 0.21] |
| Finger Puppets | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | 7.38 | <0.01 | −2.06 [−2.60, −1.51] |
| Medical Clowns | 1.16 | 0.25 | −0.61 [−1.63, 0.42] | 2.82 | <0.01 |
| N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N.E |
| Parental Distraction | 0.81 | 0.42 | −0.25 [−0.85, 0.35] | 1.02 | 0.31 | −0.32 [−0.92, 0.29] | N. E | N. E | N. E | N. E | N. E | N. E | 1.51 | 0.13 | −0.25 [−0.85, 0.35] |
| Robot Coach | 2.92 | 0.003 | −0.67 [−1.12, −0.22] | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | 1.65 | 0.10 | −0.37 [−0.81, 0.07] |
|
| |||||||||||||||
| Buzzy or Vibration | 4.68 | <0.01 | −1.14[−1.62, −0.66] | 5.01 | <0.01 | −2.30 [−3.20, −1.40] | 4.97 | <0.01 | −2.15 [−2.99, −1.30] | 4.90 | <0.01 | −2.69 [−3.77, −1.61] | 1.46 | 0.14 | −0.57 [−1.34, 0.20] |
| Cold Spray | 2.54 | 0.01 | −2.35 [−4.17, −0.53] | 13.29 | <0.01 | −3.11 [−3.57, −2.65] | 2.42 | 0.02 | −2.01 [−3.64, −0.38] | 6.55 | <0.01 | −2.66 [−3.46, −1.87] | N. E | N. E | N. E |
| Ice Gel | 1.61 | 0.11 | −0.41 [−0.90, 0.09] | 1.99 | 0.05 | −0.50 [−1.00, −0.01] | 1.86 | 0.06 | −0.47 [−0.97, 0.02] | 1.80 | 0.07 | −0.46 [−0.95, 0.04] | N. E | N. E | N. E |
| Shotblocker | 4.15 | <0.01 | −0.62 [−0.92, −0.33] | 2.32 | 0.02 | −1.17 [−2.16, −0.18] | 2.64 | <0.01 | −0.91 [−1.58, −0.23] | 2.40 | 0.02 | −1.18 [−2.14, −0.21] | N. E | N. E | N. E |
| Tactile Manual | 1.73 | 0.08 | −1.21 [−2.58, 0.16] | 1.34 | 0.18 | −0.97 [−2.38, 0.45] | 1.68 | 0.09 | −0.48 [−1.04, 0.08] | 1.29 | 0.20 | −0.88 [−2.21, 0.46] | N. E | N. E | N. E |
|
|
| < |
|
| < |
|
| < |
|
|
|
| N. E | N. E | N. E |
| Musical Bracelet | 4.63 | <0.01 | −2.04 [−2.60, −1.48] | 8.24 | <0.01 | −1.58 [−1.95, −1.20] | 11.91 | <0.01 | −2.82 [−3.29, −2.36] | 10.48 | <0.01 | −2.24 [−2.66, −1.82] | N. E | N. E | N. E |
| Kaleidoscope | 6.33 | <0.01 | −1.78 [−2.33, −1.23] | 6.21 | <0.01 | −1.73 [−2.28, −1.18] | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E | N. E |
| Rotating Tactile | 13.31 | <0.01 | −1.90 [−2.18, −1.62] | 10.31 | <0.01 | −2.18 [−2.60, −1.77] | 13.60 | <0.01 | −3.89 [−4.45, −3.33] | 12.79 | <0.01 | −3.31 [−3.81, −2.80] | N. E | N. E | N. E |
| Musical and Dancing | N. E | N. E | N. E | 0.37 | 0.71 | 0.10 [−0.41, 0.60] | N. E | N. E | N. E | 0.46 | 0.65 | −0.12 [−0.62, 0.39] | N. E | N. E | N. E |
| Intervention | Biological Marker | Z-Value | SMD + IC | |
|---|---|---|---|---|
| Somatosensory: Buzzy or Vibration | Respiratory Frequency | 0,15 | 0,88 | 0.03 [−0.36, 0.42] |
| Diastolic Blood Pressure | −0,72 | 0,47 | −0.15 [−0.54, 0.25] | |
| Systolic Blood Pressure | 0,28 | 0,78 | 0.06 [−0.34, 0.45] | |
| Heart Rate | −0,46 | 0,65 | −0.09 [−0.49, 0.30] | |
| Screen-Based: Cartoons | Heart Rate | 0.73 | 0.47 | 0.16 [−0.27, 0.58] |
| Social Interaction: Robot Coach | Heart Rate | 0.18 | 0.86 | 0.04 [−0.38, 0.46] |
| Simple Cognitive: Listening to Music | Heart Rate | −0,27 | 0,79 | −0.08 [−0.69, 0.52] |
| Social Interaction: Medical Clowns | Cortisol | −0,46 | 0,64 | −0.13 [−0.67, 0.41] |
| Toy Interaction: Musical and Dancing | Heart Rate | 1,57 | 0,12 | 0.41 [−0.10, 0.92] |
| Oxygen Saturation (SpO2) | −0,79 | 0,43 | −0.20 [−0.71, 0.30] | |
| Immersive Reality: Video with VR Glasses | Respiratory Frequency | −1,16 | 0,24 | −0.23 [−0.63, 0.16] |
| Diastolic Blood Pressure | 0,73 | 0,46 | 0.15 [−0.25, 0.54] | |
| Systolic Blood Pressure | −0,38 | 0,7 | −0.08 [−0.47, 0.32] | |
| Heart Rate | −0,61 | 0,54 | −0.12 [−0.51, 0.27] |
| Intervention | Biological Marker | Z Value | P Value | SMD + IC |
|---|---|---|---|---|
| Somatosensory: Buzzy or Vibration | Respiratory Frequency | −0,93 | 0,35 | −0.19 [−0.58, 0.21] |
| Heart Rate | −1,04 | 0,3 | −0.21 [−0.60, 0.19] | |
| Screen-Based: Cartoons | Heart Rate | −9,21 | <0.00001 | −1.11 [−1.35, −0.87] |
| Oxygen Saturation (SpO2) | 0,34 | 0,74 | 0.04 [−0.18, 0.26] | |
| Systolic Blood Pressure | −6,56 | <0.00001 | −0.76 [−0.99, −0.54] | |
| Diastolic Blood Pressure | −5,3 | <0.00001 | −0.61 [−0.83, −0.38] | |
| Heart Rate | 0,27 | 0,79 | 0.05 [−0.32, 0.43] | |
| Simple Cognitive: Listening to Music | Heart Rate | −0,67 | 0,5 | −0.12 [−0.48, 0.24] |
| Toy Interaction: Musical and Dancing | Heart Rate | 2,91 | 0,004 | 0.78 [0.25, 1.31] |
| Oxygen Saturation (SpO2) | −1,88 | 0,06 | −0.49 [−1.01, 0.02] | |
| Screen-Based: Informational Video | Heart Rate | −8,35 | <0.00001 | −0.99 [−1.23, −0.76] |
| Oxygen Saturation (SpO2) | 0,54 | 0,59 | 0.06 [−0.16, 0.28] | |
| Systolic Blood Pressure | −7,17 | <0.00001 | −0.84 [−1.07, −0.61] | |
| Diastolic Blood Pressure | −5,66 | <0.00001 | −0.65 [−0.88, −0.43] | |
| Immersive Reality: Video VR Glasses | Respiratory Frequency | −1,16 | 0,25 | −0.23 [−0.63, 0.16] |
| Heart Rate | 6,76 | <0.00001 | 1.55 [1.10, 2.00] |
| Intervencion | Sample | Measure Self-report | Observed Behavior | Biological markers | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Before | During | After | Before | During | After | Before | During | After | ||
|
| ||||||||||
| Palm Stimulator | School Age ( | Fear: CFS | Pain: VAS, FPS-R | Fear: CFS | Pain: FPS-R | |||||
| Blowing Soap Bubbles | Preschool ( | Pain: WB-FACES ( | Pain: Oucher ( | Pain: WB-FACES. Fear: CFS ( | Pain: WB-FACES ( | Pain: Oucher ( | Pain: WB-FACES. Fear: CFS ( | |||
| Shotblocker | School Age ( | Pain: WB-FACES ( | Pain: Oucher. Fear: CFS ( | Pain: WB-FACES ( | Pain: WB-FACES ( | Pain: WB-FACES, Oucher ( | Pain: WB-FACES. Fear: CFS ( | |||
| Stress Ball | School Age ( | Pain: WB-FACES. Fear: CFS | Pain: WB-FACES. Fear: CFS | Pain: WB-FACES. Fear: CFS | Pain: WB-FACES. Fear: CFS | |||||
| Whistling Breathing | Preschool & School Age ( | Pain WB-FACES | Pain WB-FACES | Fear CMFS | ||||||
|
| ||||||||||
| Video Game with Virtual Reality | Preschool ( | Pain: VAS ( | Pain: VNRS. Fear: CFS ( | Pain: VAS ( | Pain: FPS-R. Fear: LTAS ( | Distress PBCL ( | Pain: FPS-R. Fear: LTAS ( | |||
| Video with Virtual Reality Glasses | Preschool ( | Pain: FPS-R ( | Pain: FPS-R ( | Pain: WB-FACES ( | Fear: CFS ( | Pain: WB-FACES ( | Distress CEMS ( | BP, HR, RR ( | BP, HR, RR ( | BP, HR, RR ( |
| Video with Virtual Reality Glasses + VID | Preschool & School Age ( | Pain: WB-FACES, CAS. Fear: CFS | Distress CEMS | Distress CEMS | ||||||
|
| ||||||||||
| Ditto D-PP-C | Preschool & School Age ( | Pain WB-FACES | Pain WB-FACES | Pain WB-FACES | Pain: VAS. Distress: FLACC | Pain: VAS. Distress: FLACC | Pain: VAS. Distress: FLACC | |||
| Informational Video | School Age ( | Pain: WB-FACES. Fear: CFS | Pain: WB-FACES. Fear: CFS | Pain: WB-FACES. Fear: CFS | Pain WB-FACES, Fear CFS | SpO2, BP, HR | SpO2, BP, HR | |||
| PSP Video Games | Preschool & School Age ( | Pain WB-FACES | Pain WB-FACES | Pain WB-FACES | Pain: VAS. Distress: FLACC | Pain: VAS. Distress: FLACC | Pain: VAS. Distress: FLACC | |||
| VR Ceiling Screen | Infant/Preschool ( | Distress FLACC, Pain and Fear VAS | ||||||||
| Cartoons | Preschool ( | Pain: FPS-R ( | Pain: WB-FACES ( | Pain: FPS-R ( | Pain WB-FACES ( | Pain: WB-FACES ( | Pain: WB-FACES, Fear: CFS ( | SpO2, BP ( | HR ( | SpO2, BP ( |
|
| ||||||||||
| Distraction Cards | School Age ( | Pain: VAS, FPS-R | Pain: VAS, FPS-R | |||||||
| Listening to Music | Preschool ( | Pain: FPS-R ( | Pain: FPS-R ( | Pain: FPS-R ( | Distress: OSBD-R ( | Pain: AHTPS ( | Distress: OSBD-R ( | HR ( | HR ( | HR ( |
|
| ||||||||||
| Vein Imaging Device | Preschool, School Age &Teenager ( | Fear CFS | Pain: WB-FACES, CAS | Distress CEMS | Distress CEMS | |||||
| Cartoon-Clothes | Preschool & School Age ( | Fear CFS | Distress FLACC | |||||||
|
| ||||||||||
| Child Life Specialists | Infant/Preschool, School Age & Teenager ( | Distress OSBD-R | ||||||||
| Finger Puppets | Preschool & School Age ( | Distress CEMS | Distress CEMS | |||||||
| Medical Clowns | Infant/Preschool ( | Pain: WB-FACES. Fear: CAPS ( | Pain: WB-FACES ( | Pain: NRS ( | Pain: NRS ( | Plasma Cortisol ( | ||||
| Parental Positioning and Distraction | Preschool & School Age ( | Pain WB-FACES, Fear GFS | Fear: GFS. Distress: PBCL | Distress: PBCL | Fear: GFS. Distres:s PBCL | |||||
| Robot Coach | School Age ( | Pain FPS-R | Pain FPS-R | Distress: OSBD-R | Distress: OSBD-R | Distress: OSBD-R | HR | |||
|
| ||||||||||
| Buzzy or Vibration | Preschool ( | Pain: CAPS ( | Pain: FPS-R ( | Pain: WB-FACES ( | Pain: CAPS ( | Pain: FPS-R ( | Pain: WB-FACES ( | BP, HR, RR ( | BP, HR, RR ( | BP, HR, RR ( |
| Cold Spray | School Age ( | Pain: VAS. Fear: CFS ( | Pain: VAS ( | Pain: VAS. Fear: CFS ( | Pain: VAS ( | |||||
| Ice Gel | School Age & Teenager ( | Pain: VAS. Fear: CFS | Pain: VAS. Fear: CFS | Pain: VAS. Fear: CFS | Pain: VAS. Fear: CFS | |||||
| Manual Tactil | Preschool ( | Pain: WB-FACES ( | Pain: WB-FACES ( | Pain: WB-FACES. Fear: CFS ( | Pain: WB-FACES Fear: CFS ( | Pain: VAS ( | Pain: WB-FACES. Fear: CFS ( | |||
|
| ||||||||||
| Kaleidoscope | School Age ( | Pain: WB-FACES. Fear: CAM-S, CMFS | Pain: WB-FACES. Fear: CAM-S, CMFS | |||||||
| Musical and Dancing | Preschool & School Age ( | Fear CFS | Fear CFS | Fear CFS | Fear CFS | Fear CFS | Fear CFS | SpO2, HR | SpO2, HR | SpO2, HR |
| Musical Bracelet | School Age ( | Pain: WB-FACES, VAS. Fear CFS | Pain: WB-FACES, VAS. Fear CFS | Pain: WB-FACES. Fear: CFS | Pain: WB-FACES. Fear: CFS | |||||
| Rotating Tactile | School Age ( | Pain: WB-FACES, VAS. Fear CFS | Pain: WB-FACES, VAS. Fear CFS | Pain: WB-FACES. Fear: CFS | Pain: WB-FACES. Fear: CFS | |||||
| Type of intervention | Main mechanism | Clinical implications in PEDs |
|---|---|---|
| Somatosensory | Provide tactile and kinesthetic stimulation that modulates pain signals through sensory inhibition. | Strong and consistent reduction of pain and fear, particularly with Cold Spray and Buzzy/Vibration. Highly feasible, low-cost and quick to apply during IMPs |
| Screen-based | Direct audiovisual attention and modulate cognitive–emotional appraisal of threat. | Informational videos before an IMP are the most effective overall. It is useful when preparation time is available. Cartoons during procedures further support distraction. |
| Active command | Encourage rhythmic motor activity and breathing to support self-regulation and effective coping. | Simple, low-cost, and effective for reducing pain and fear when children actively participate during IMPs. Practical as a complementary strategy. |
| Toy interaction | Facilitate playful tactile or visual engagement that activates sensory feedback. | Effective for pain and fear. Useful when toys can be manipulated by the child. Best suited for brief IMPs, fostering positive engagement and distraction. |
| Immersive reality | Provide immersive multisensory distraction through visual and proprioceptive engagement. | Helpful for behavioral distress but effects on pain and fear are inconsistent. Limited by cost, setup time, and sensory tolerance. More suitable for older children and adolescents. |
| Social interaction | Engages emotional and social co-regulation to reduce perceived threat and enhance security cues. | Finger puppet play and robot interaction reduced distress, while parental and clown distraction yielded mixed results, likely influenced by caregiver stress and interaction quality. |
| Unisensory distractions | Use single-channel sensory input to focus attention (visual or auditory) | Music and card viewing showed moderate effects on fear and behavioral distress. Useful as low-cost complementary tools rather than standalone interventions. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Pain Management Techniques · Infant Development and Preterm Care · Music Therapy and Health
Introduction
Facing invasive medical procedures (IMPs) in a pediatric emergency department (PED) can be a stressful and potentially traumatic experience for children and adolescents (1–3), as it involves greater stressors compared to other healthcare contexts (4, 5). The structure and functioning of a PED are characterized by a crowded and fast-paced environment, unpredictability, and sensory overstimulation across admission, diagnosis, and treatment (6–11). This process is also frequently compounded by stressors related to the acute illness that prompted the visit, caregiver stress levels, and the procedural pain experience itself (12–18). Furthermore, IMPs in PEDs often involve high levels of anticipatory fear and procedural pain (19), which may increase behavioural distress, and in effect, child verbal and physical resistance, leading to higher stress for caregivers and healthcare personnel (19–21). High behavioral distress may also imply prolonged procedures and lower efficiency required in PEDs (22, 23).
Pain experiences, fear, and behavioral distress in PEDs not only impact the immediate experience of the pediatric patient but can also have long-term psychological and somatosensory consequences. Psychologically, there is a significant link between negative pre-hospital and hospital experiences and the development of negative pain memories, anxiety, depression, avoidance behaviors, unnecessary visits, and poor adherence to health advice (24–27). From a somatosensory perspective, neuroscience studies suggest that children may be at higher risk of developing central sensitization (28–30), leading to increased pain sensitivity, lowered pain thresholds, chronic pain, and lasting changes in pain pathways (28, 31–35). Therefore, it is essential to identify interventions that are both effective and efficient in PEDs to improve patient experiences and reduce immediate and long-term complications (36).
Some psychological and sensory interventions have proven effective in reducing pain, fear, and behavioral distress in outpatient IMPs (37). Sensory interventions involve the use of specific sensory stimuli (tactile, auditory, visual, proprioceptive, vestibular) to enhance sensory regulation and adaptive response to painful stimuli (38, 39). Psychological interventions integrate cognitive, emotional, behavioral, and social elements in the modulation of pain (40–42). Psychosensory interventions, in this context, refer to strategies that integrate both sensory stimulation and psychological regulation processes to influence pain perception and emotional responses. The theoretical and empirical foundations of how psychosensory approaches support a biopsychosocial modulation of pain are promising for advancing understanding of the mechanisms underlying their effectiveness (43, 44). Despite the growing use and evaluation of psychosensory approaches in PEDs, a comprehensive overview of their comparative effectiveness remains limited, which is crucial for appropriate evidence-based implementations within this complex setting. Hence, this systematic review and meta-analysis aims to: (1) analyze and summarize the current state-of-the-art evidence (acquired through randomized controlled trials [RCTs]) on the effectiveness of psychological and sensory interventions in managing pain, fear, and distress in children undergoing IMPs in PEDs; and (2) analyze the methodological rigor and quality of the RCTs included in the review.
Materials and methods
Procedure
The study was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA, 2020) Statement to ensure transparency and thoroughness at all stages of the process (45). Searches were conducted over the last two decades (January 2004–September 2024), ensuring methodological and contextual relevance to current PEDs.
Literature search
A systematic review of RCTs evaluating the effectiveness of psychological and/or sensory strategies to manage pediatric pain, fear, and behavioral distress was conducted, according to the pre-registered protocol on PROSPERO (CRD42023403583). The search terms focused on these primary outcomes, using combinations of descriptors such as “Children OR Adolescent,” “Psychological OR Sensory Intervention,” “Pain OR Fear OR Distress,” and “Emergency Department,” connected with the Boolean operator AND (see Supplementary Material 1). Boolean phrases were adapted to the thesauri of PubMed, CINAHL, PsycInfo, Scopus, and Web of Science databases. Gray literature was not included. However, backward and forward snowballing were performed on the reference lists and citations of the included studies to identify any eligible RCTs not captured in the primary database search.
These outcomes were prioritized because they represent the core emotional and behavioral manifestations of procedural stress in children, which are directly observable or self-reported and clinically relevant for evaluating the effectiveness of psychosensory interventions. Physiological or biological indicators (e.g., heart rate, respiratory rate, blood pressure, oxygen saturation, cortisol) were retained as complementary secondary outcomes when reported alongside emotional or behavioral measures, as they provide additional information about autonomic activation associated with procedural stress. However, these indicators were not included as specific search terms, as they were outside the scope of the main research question.
Inclusion and exclusion criteria
Inclusion criteria were: (1) Studies published from 2004 onwards; (2) studies published in English or Spanish; (3) RCTs; (4) studies with at least one control group with usual care; (5) children aged 2–18 years; (6) studies evaluating a psychological, sensory, or mixed psychosensory intervention implemented within PED care; (7) PED as the setting intervention; (8) sample undergoing at least one IMPs for diagnosis or treatment purposes (e.g., intravenous line, blood sample, or injections); (9) studies evaluating pain, fear, or behavioral distress as outcomes assessed through self-report or observer-report.
Studies were excluded if: (1) children had a severe chronic diagnosis that could interfere with outcomes (e.g., cancer, cystic fibrosis); (2) studies were caregiver-focused only; (3) hospitalization or outpatient settings; (4) interventions applied only on the waiting room or post-discharge; (5) PED care without IMPs; (6) sample size below 30 children, and (7) studies focusing exclusively on physiological or biochemical parameters.
Selection process
The article selection process is presented in the PRISMA flowchart (see Figure 1). Two reviewers (MB and VT) independently selected the articles meeting the eligibility criteria by first reviewing all identified titles and abstracts, and subsequently all full texts selected after the abstract selection. Discrepancies between reviewers were resolved by consensus.
PRISMA flow diagram.
Data extraction and synthesis
Data extraction was performed independently by two reviewers (MB and GD) using a predefined extraction form, which included: study design, sample size, type of IMPs, participant demographic information (age, gender), details of interventions (type, duration, frequency, and timing), outcomes measured (self-reported, observed pain, fear, behavioral distress as well as biological markers), and statistical results (mean differences, standard deviations [SD], p-values, and confidence intervals [CI]) (see Table 1).
Risk of bias
The risk of bias was assessed using the Cochrane Collaboration's Tool (46). This tool classifies studies according to the risk of bias in six domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, and incomplete outcome data. Each study was categorized as having high, moderate, or low risk in each domain, allowing for a nuanced and accurate assessment of the methodological quality and internal validity of the trials included in the analysis. The risk of bias for each included studies was assessed by two independent reviewers (MB and IR), with conflicts resolved by a third reviewer (LC).
Meta-analysis
A bibliometric analysis of the selected RCTs was performed to gain an in-depth overview of the study characteristics and obsolescence across all the evidence. Obsolescence was calculated by means of the Burton-Kebler (Calculates the median age of cited articles to determine the “half-life” of the literature) and Prince index (Measures the percentage of cited articles that are less than a specified 5 years).
Meta-analysis was conducted to calculate pooled effect sizes of psychosensory interventions on self-reported or observed pain, fear, and behavioral distress. Review Manager (RevMan) Web version endorsed by the Cochrane Collaboration was used, to compute the effect sizes (Z-value and standardized mean difference [SMD]) and design of the forest plots. Effect sizes are reported along with a 95% CI and presented both quantitatively and graphically using forest plots. In these forest plots, each trial is visually represented as a horizontal diamond shape, where the center indicates the effect size, and the end points represent the CI limits.
Random-effects models (inverse-variance method) were selected a priori, given the anticipated clinical and methodological diversity among studies. Heterogeneity was assessed using the Chi^2^ and I^2^ statistics. The Chi^2^ statistic is used to determine if the variation among studies is significant. A low Chi^2^ and high p-value indicate no significant heterogeneity, suggesting consistency across studies. A high Chi^2^ and low p-value indicate significant heterogeneity, suggesting variations greater than expected by chance. On the other hand, the I^2^ statistic measures is used to determine the proportion of total variation due to heterogeneity. I^2^ providing a percentage that indicates the degree of inconsistency in the results, and I^2^ value of 25% indicates low heterogeneity, 50% moderate, and 75% high heterogeneity.
Subgroup analyses were pre-registered in PROSPERO to explore potential differences by (a) procedure type, (b) age range, and (c) adult intervention (type and if was performed by parental or professional). Quantitative subgroup analysis was feasible only by intervention modality, as mostly included studies involved venipuncture or intravenous procedures, and only one study specified exclusive parental implementation. No meta-regression was conducted, given the limited number of studies per subgroup and the diversity of designs.
Accordingly, effect sizes were calculated for seven intervention subtypes, identified and analyzed based on the type of stimulus involved in each psychosensory strategy: (1) Somato-Sensory includes interventions providing direct tactile or kinesthetic stimulation, such as vibratory (Buzzy) or cold devices (Cold Stray, Ice gel) and tactile stimulators (e.g., shotblocker). (2) Immersive Reality, which uses Virtual reality (VR) devices to engage children in simulated experiences, either through passive observation or active interaction. (3) Screen-based, uses audio-visual distractions screens, such as cartoons video and video games. (4) Toy interaction use toys to capture the child's attention during the procedure, with or without handling. (5) Social interaction includes dynamic activities with others (e.g., medical clowns, robots, caregivers or child life specialists (CLS). (6) Active command, involve simple commands to cope with the situation and require the child's active participation, such as squeezing a stress ball, whistling, or blowing soap bubbles. (7) Unisensory distractions involve simple cognitive or visual interventions, like viewing cards, vein imaging device (VID) or listening to music, without combining multiple sensory stimuli.
Sensitivity analyses were not performed, as the primary objective of this review was to estimate the overall effectiveness of psychosensory interventions across heterogeneous designs. Given the diversity of interventions and outcome measures, excluding studies based on methodological quality or sample size would have substantially reduced statistical power.
Results
Article selection
A total of 1,796 articles were identified by the searches. After removing 269 duplicates, 1,527 titles and abstracts were screened, revealing 155 abstracts meeting the inclusion criteria for full-text screening. After full-text screening, 45 articles were selected for final inclusion, one of which was identified through backward snowballing after full-text screening. The main reasons for exclusion were: (1) irrelevant sample, as some studies included adults or focused on age groups not related to the review, such as neonates; (2) not pertinent and setting intervention with studies not applied in PED; (3) unrelated intervention, with some studies addressing pharmacological approaches instead of psychological or sensory interventions; (4) inappropriate type of procedure, excluding studies that did not focus on IMPs; (5) non-experimental or quasi-experimental study design; and (6) absence of relevant outcomes, where studies did not measure outcomes such as pain, fear, or distress during the procedure (see Figure 1).
The total sample size across the 45 articles was N = 6,480 children (3,087 females and 3,393 males). The mean age of participants was 7.34 with a of SD 3.26. The mean age of articles was 3.76 years, with a SD of 4.57, 95% CI [3.24, 5.91]. The most recent article was 4 months old, with the oldest being 20 years old. The obsolescence of the RCTs, considering a Burton-Kebler index and Prince index, showed a median of 2 years, with 84.44% of the RCTs being less than 5 years old. The 45 studies were conducted in 13 countries, mainly in Turkey (n = 19; 42.2%), Canada (n = 9; 20.0%), and the United States (n = 4; 8.9%). The remaining studies came from 10 other countries across Europe, Asia, and the Middle East (see Table 1).
The following sections present the outcomes for pain, fear, and distress, as reported by either children or observers, across all the interventions as well as grouped by these intervention categories. Results are presented in order of effectiveness of the intervention category. Due the limited findings for biomarkers, the results for biomarkers could not be organized by intervention category, hence these findings are organized according to the assessed biomarker instead.
Pain
Thirty-seven studies evaluated the effectiveness in reducing pain, demonstrating significant reductions in both self-reported and observer-reported pain. For self-reported pain, the overall effect test yielded a Z value of 7.66 (p < 0.01), with a total SMD of −0.94 (95% CI: −1.19, −0.70). Subgroup analysis revealed substantial heterogeneity, evidenced by Chi^2^454.17 (df = 17, p < 0.01) and an I^2^ of 96.3%. For observer-reported pain the overall effect yielded a Z value of 6.27 (p < 0.01) with an SMD of −1.52 (95% CI: −2.05, −0.99). The substantial heterogeneity was evidenced by Chi^2^264.40 (df = 11, p < 0.01), reflecting an I^2^ 95.8%. Below is a summary for the effectiveness of the intervention category, ordered by the efficacy of the interventions (SMD, Z and p-values are in Table 2).
Somato-Sensory (N = 15 studies): Buzzy or vibration, cold spray, and Shotblocker significantly reduced pain both types of reports (47–61). Manual Tactile significantly reduced observer-reported pain (57), while it only approached significance for self-reported pain (57, 61). Ice gel approached significance only for observer-reported pain (48), while it did not reach statistical significance for self-reported pain (48).
Screen-Based (N = 9 studies): Informational videos were effective in reducing self-reported and observer-reported pain (62). For observer-reported pain, Ditto device in its 3 versions, [Distraction (D), Preparation (PP), and both Combined (C)], ceiling-mounted VR (63, 64), and cartoons screens showed a significant effect (65–70).
Toy-Interaction (N = 2 studies): Rotating tactile, musical bracelet, and kaleidoscope were effective in reducing pain for both self-reported and observer-reported measures (71, 72).
Unisensory-Distractions (N = 5 studies): For self-reported pain, viewing cards and listening to music were effective in reducing pain (61, 70, 72, 73), while VID did not reach statistical significance (74).
Immersive Reality (N = 10 studies): VR glasses showed significant results for self-reported pain but did not reach significance for observer-reported pain (58, 65, 72, 74–77). VR video games were not significant in reducing self-reported pain but approached significance in observer-reported pain (68, 78, 79).
Active-Command (N = 4 studies): Squeezing a stress ball and the palm stimulator were significantly effective in reducing self-reported and observer-reported pain (60, 80). Blowing soap bubbles was effective in reducing self-reported pain but did not reach significance in observer-reported pain (58, 79). Whistling approached significance for self-reported pain (53).
Social-Interaction (N = 5 studies): Robot were significantly effective in reducing self-reported pain (81), while neither parental distraction (82) nor medical clowns (83–85) reached statistical significance in the same measure.
Fear
Twenty-six studies evaluated the impact of interventions on their effectiveness of reducing fear. The analysis revealed a significant reduction in self-reported fear, with an overall effect test of Z = 6.18 (p < 0.01) and a total SMD of −1.30 (95% CI: −1.71, −0.89). Subgroup analysis indicated substantial variability, as reflected in the Chi^2^ = 392.44 (df = 14, p < 0.01) and an I^2^ 96%. Similarly, for observer-reported fear (evaluated in thirteen studies) a significant effect was demonstrated, with an overall effect of Z = 5.28 (p < 0.01) and an SMD of −1.77 (95% CI: −2.43, −0.16). The subgroup differences highlighted significant heterogeneity, with Chi^2^ = 166.02 (df = 9, p < 0.01) and an I^2^ 94.6%.
Somato-Sensory (N = 9 studies): Cold Spray, Buzzy, and Shotblocker were significantly effective in reducing both self-reported and observer-reported fear (48, 51, 53, 54, 58, 59). Ice Gel approached significance for both types of reports (48), while Manual Tactile did not reach significance in either of them (49, 57, 60).
Toy-Interaction (N = 3 studies): Rotating tactile, musical bracelet, and viewing a kaleidoscope were significantly effective in reducing both self-reported and observer-reported fear (71, 72). In contrast, musical and dancing toys (MDT) did not reach significance for either type of report (86).
Unisensory-Distractions (N = 3 studies): Listening to music was effective in reducing self-reported fear (72). Cartoon-patterned clothes demonstrated significant results for reducing self-reported fear (87), while the VID did not reach significance for either type of report (74).
Immersive-Reality (N = 10 studies): VR headset videos significantly reduced self-reported fear, but did not reach significance in observer-reported fear (58, 65, 72, 74–77). VR video games (68, 78, 79) showed no significant reduction in self-reported fear.
Active-Command (N = 5 studies): Blowing soap bubbles and squeezing a stress ball significantly reduced both self-reported and observer-reported fear (59, 80, 87). However, whistling was only effective in reducing self-reported fear (53), and Palm Stimulator was not significant in any measurement (60).
Screen-Based (N = 4 studies): Informational videos and cartoons were significantly effective in reducing both self-reported fear and observer-reported (62, 65, 68) and ceiling-mounted VR screens for observer-reported (63).
Distress
The studies (N = 17) evaluated the effectiveness in reducing observer-reported distress in children during IMPs in PEDs and included combined results from parental, healthcare staff, and researcher perceptions. The pooled effects analysis showed a significant effect for observer-reported distress reduction (Z = 4.38, −0.57 [−0.83, −0.32] p < 0.01). The differences between subgroups were also significant (Chi^2^ = 59.84, df = 13, p < 0.01; I^2^ = 78.3%), suggesting variability in the efficacy of the different categories of intervention.
Active-Command (N = 1 study): Blowing soap bubbles significantly reduced distress level (87).
Immersive Reality (N = 5 studies): VR video games and VR goggles were effective in reducing distress (58, 74, 75, 78, 88).
Screen-Based (N = 4 studies): The Ditto device (64) (D-PP-C) and video games (64) showed a significant effect in reducing distress, while cartoons and ceiling-mounted VR screens did not reach significance (63, 64, 69, 70).
Social Interaction (N = 4 studies): Finger puppet significantly reduced observer-reported distress (89). Robot, caregivers and CLS support did not reach significance (81, 82, 90).
Unisensory-Distractions (N = 4 studies): Cartoon-patterned clothes (colorful animated characters), demonstrated modest but significant results (87). Listening to music was not effective in reducing distress (70, 73), and VID showed a trend toward significance (74).
Somato-Sensory (N = 4 studies): Buzzy were not significant in reducing distress (47, 52, 58, 91).
Biological markers
Only seven studies evaluated biological markers during the procedure (58, 66, 69, 73, 78, 81, 86), while five studies assessed them post-procedure (58, 62, 69, 70, 86).
For Heart Rate (HR), informational videos significantly reduced post-procedural HR (62), while VR glasses and MDT significantly increased heart rate post-procedure (86). Buzzy showed no significant effect on post-procedural HR (58). During the procedure, no significant changes were observed for HR in most of the evaluated interventions (58, 62, 66, 70, 73, 81, 86). Only one study reported a significant reduction of HR (cartoon intervention, p < 0.01) (69) but without the mean and SD per group.
For post-procedural blood pressure, informational videos and cartoons significantly reduced both systolic and diastolic pressure (62). During the procedure, no significant effects were observed for any interventions (58). For SpO2 (Oxygen Saturation), MDT approached significance post-procedure (86), but not during the procedure. Video with VR glasses showed no significant effects during/post-procedure (58). No intervention impacted plasma cortisol levels during the procedure (84) or respiratory frequency during/post-procedure (58).
Risk of bias assessment
The risk of bias was assessed using the RoB-2 tool for RCTs, through which 40% of studies were classified as low risk, 40% as having some concerns, and 20% as high risk (see Figure 2). The risk levels with respect to the five domains were as follows: (1) the randomization process showed low risk in 77.8% of studies, some concerns in 20%, and high risk in 2.2%; (2) for deviations from intended interventions, 57.8% were at low risk, 26.7% some concerns, and 15.6% were high risk; (3) regarding missing outcome data, 88.9% were low risk, 8.9% some concerns, and 2.2% were high risk; (4) in the measurement of the outcome domain, 64.4% were rated as low risk, 22.2% as some concerns, and 13.3% as high risk; (5) for the selection of the reported result, 73.3% were at low risk, 24.4% some concerns, and 2.2% were high risk.
Risk of bias assessment of randomized clinical trials in each domain of the RoB-2 tool.
Deviations from the intended intervention were the domain with the highest level of bias across the studies. This high level of bias was primarily due to the lack of or inability to blind participants and/or intervention providers to the assigned study group. Only a few studies attempted to minimize this bias by blinding outcome assessors (50, 73, 90) and/or by blinding data analysis (80). Additionally, a second major source of bias in this domain stemmed from the high variability in implementing social component interventions across both groups. For the experimental group, this was observed when clowns, CLS, and/or caregivers employed flexible distraction strategies, and for the control group, when usual distraction methods were left to the discretion of healthcare personnel and caregivers. The interactive and adaptive nature of non-standardized social interventions increased the risk of deviations from the intended protocol, as the child's response, caregiver involvement, and intervention provider's style could differ significantly from case to case, impacting intervention consistency. Although some studies attempted to reduce variability in implementation by assigning the same provider, this approach increased the risk of bias in outcomes due to the lack of blinding, highlighting the methodological challenge of balancing standardization and control in studies with psychological interventions.
Discussion
Main findings and comparative effectiveness
This systematic review and meta-analysis compiled and analyzed the evidence available about interventions aimed at reducing pain, fear, and distress in children undergoing IMPs in PEDs, as assessed using self- or observer report or biomarkers. The interventions were grouped according to the type of stimulus, including somato-sensory, screen and immersive reality, social interaction, active command and unisensory distractions. The meta-analysis revealed the potential of psychological and sensory interventions to reduce pain, fear, and distress during the procedure, as well as induce some significant reductions in post-procedure biological markers. However, not all interventions demonstrated the same effectiveness across all outcomes.
Based on the size SMD, somato-sensory (Buzzy or Vibration, Cold Spray), tactile toys (Musical Bracelet Toy, Rotating Tactile Toy), and screen-based interventions (Informational Video, Cartoons) were the most effective interventions and exhibited concordance between child-reported and observer-reported outcomes for both pain and fear. Informational videos were the most effective interventions for both self-reported and observer-reported pain and fear outcomes, followed by rotating tactile toys in second place, and somato-sensory interventions, such as buzzy and cold spray, in third place. Active Command strategies were effective in pain and fear the more active the child's participation was. Regarding social interventions, finger puppet stood out as the most effective intervention for reducing observed distress, while interaction with a robot was only significant for self-reported pain. However, parental distraction, interaction with clowns, and CLS support did not show any significant results across all outcomes. VR-based interventions showed large discrepancies between child-reported and observer-reported outcomes for pain and fear. Interventions like VR video games and the Ceiling-Mounted VR Screen were not significant for self-reported outcomes but were significant for observer-reported pain and fear. In contrast, VR Glasses significantly reduced self-reported, but not observer-reported fear.
The large effect sizes observed in some analyses, and the discrepancies between observer- and self-reported outcomes, should be interpreted in light of methodological and contextual factors specific to PEDs settings. Observer ratings are particularly sensitive to visible behavioral changes, which can yield substantial standardized differences even with modest clinical improvements. In contrast, children's self-reports were often obtained after partial emotional regulation, resulting in smaller SMDs. Moreover, the high emotional reactivity typical of PEDs contexts may amplify observable changes in distress behavior, producing apparently larger intervention effects. These contextual influences indicate that large SMDs likely reflect not only the clinical efficacy of psychosensory interventions but also setting-specific perceptual and methodological factors.
Mechanisms of psychosensory modulation
The findings of somato-sensory interventions in reducing pain and fear are align with previous research in primarily outpatient settings (92–95). Their effectiveness can be explained by the somatosensory activation of cutaneous nerve fibers that inhibit pain signals sent to the brain, Aβ fibers, which transmit sensations of touch, pressure, and vibration (Buzzy), and Aδ and C fibers, responsible for detecting stimuli related to pain and temperature (Cold Spray) (96, 97), facilitate an ascending modulation of pain (98). Concerning the difference in effect size between the two strategies on pain reduction (cold spray being more effective than Buzzy), recent evidence suggests that Cold Spray shows greater efficacy, as its inhibitory effect is more intense, rapid, and direct, whereas Buzzy modulates nociceptive signals without fully blocking them (99–102). Additionally, the combination of vibration with cold may cause both stimuli to compete for sensory attention, with the vibratory stimulus tending to dominate, diminishing the cold stimulus's effect and, thus, its efficacy in pain modulation (54, 103). On the other hand, the similar efficacy regarding fear levels can be understood from the conditioned inhibition perspective, where either intense acts as a safety signal, conditioning the child to associate the procedure with a less painful and threatening experience (104–106). However, our results also suggest informational videos and certain toys can be equally or more effective than somato-sensory, in the context of PEDs, which contrasts with outpatient settings where Buzzy consistently shows greater efficacy than other visual or auditory strategies (94). Specifically, the use of informational videos was the intervention with the greatest effect size in the meta-analysis. One key explanatory variable could be the influence of environmental stressors. A visit to an ED involves higher cognitive and emotional demands than outpatient care. These environmental stressors may act as amplifiers of fear experiences, increasing the relevance of a focus on modulating the cognitive and emotional pathways of pain (107). According to the cognitive and emotional pain modulation framework, pre-procedural education may act through cognitive restructuring of the experience, where information about what will happen (what, how, where, with whom) may help modulate the perception of threat and anticipatory emotional response (108–111). Taking into consideration that informational videos also show a child model successfully undergoing an IMP, their effectiveness can also be explained through vicarious learning processes, where a positive model can counteract fear acquired through negative experiences or previous negative models (112, 113).
Regarding the use of toys, three of them (Rotating Toy, Musical Bracelet, Kaleidoscope) were consistent with previous evidence in reducing pain and fear in outpatient settings (114–116). The fourth toy, MDT, did not reach statistical significance. This could be because, unlike the other three effective toys, which the child could touch or interact with during the procedure, the MDT could only be passively observed. From the perspective of pain neuroscience, tactile stimulus manipulation enhances the activation of descending pain modulation mechanisms through sensory and motor feedback (117–119), which may explain the differences in their effectiveness despite all being play objects.
Similarly, the effectiveness of active command or instruction strategies, where the child follows a guided action continuously during the procedure (e.g., squeezing a stress ball, blowing bubbles, palm stimulator and whistling), can be explained by both ascending and descending pain modulation. On the one hand, at the descending level the voluntary and repetitive nature of the action influences the activation of cognitive and emotional pain modulation areas. The types of actions themselves activate both sensory and autonomic systems. On the other hand, at the ascending level, similar to Buzzy and Cold Spray, the pressure of the stress ball and palm stimulator stimulates nerve fibers in the skin that can inhibit pain signals (120). Controlled breathing and bubble blowing activate sympathetic and parasympathetic systems, as a way of optimizing the modulation of psychophysiological pain responses (121–123).
The findings on the effectiveness of VR are consistent with mixed efficacy findings in predominantly outpatient settings (124–127). To gain a better insight into the heterogeneity observed in the effectiveness for VR interventions within meta-analysis, we consider four key variables that could explain the variation. Firstly, the age of the sample. During early to middle childhood, the proprioceptive and vestibular systems are still developing. Hence, VR interventions, which require high processing of both systems, increase the likelihood of discomfort with the device (128, 129), leading to variable efficacy of the experience on reducing pain, fear or distress. Particularly, studies involving infants and preschoolers showed more discomfort and a tendency to remove the device (78, 79). As half of the VR studies in the meta-analysis included early childhood participants, this could explain the lower efficacy outcomes across our meta-analysis. Secondly, environmental and illness-related stressors can impact the effectiveness of VR interventions. It has been documented that higher stress levels increase susceptibility to adverse VR effects (disorientation, dizziness, and nausea) (130). Both the stress of the ED environment and illness-related stress can limit participants' tolerance for VR, which varies widely among individuals, contributing to heterogeneous results across studies. Thirdly, the VR format and content varied widely amongst the included interventions. Among the 12 interventions using VR strategies, there were four presentation formats and 11 different content types. The level of cognitive and sensory load involved in each is key to its efficacy. The use of VR video games is considered the format with the highest cognitive demand due to the need for active interaction and real-time decision-making, which can affect children's ability to process and report their pain experience, leading to discrepancies in self-reported results (131–135). Lastly, the discrepancies between observed and self-perceived outcomes could have further added to the variation in effectiveness. Neuroscientific studies affirm that VR primarily influences visual and motor circuits, reducing behavioral pain expression, but to a lesser extent, it affects the anterior cingulate cortex and insula, which integrate the subjective dimension of pain (136). In high-cognitive-demand VR interventions, this could explain why observers perceive a behavioral change while participants may not experience a reduction in subjective pain. Conversely, low-cognitive-demand VR interventions may result in less behavioral pain expression but facilitate better subjective self-perception.
Social and developmental factors
The effectiveness of social interventions in managing pain and distress in children during medical procedures appeared to be largely dependent on the child's age and the type of interaction. Finger puppet interaction in preschoolers was significant in reducing observed distress, likely due to the playful and dynamic nature of the interaction, which uses both visual and tactile stimulation, facilitating the modulation of cognitive and emotional pain pathways (95). In older children (6–12 years), the efficacy of interaction with robots on self-perceived pain could be associated with stimulating cognitive and emotional neural circuits, favoring downward pain regulation, which has also been evidenced in previous literature (137–140). On the other hand, parental distraction and CLS support, which did not show any significant impact across any of the outcomes, were applied to a broader sample (ages 2–16). Age differences may be important, considering that during early childhood, children are more dependent on parental co-regulation, while individual intervention strategies become more effective from school age onwards. Furthermore, evidence suggests that social pain modulation requires active and quality strategies (141, 142). In the ED context, not all caregivers may be effective in providing distraction after brief training, and parental stress levels may reduce the quality of their intervention (143–145). Importantly, none of the studies observed the parental or CLS's behaviors during the intervention, which would allow checking how well they were adhering to intervention training instructions rather than engaging in more habitual behaviors. Regarding the above, both verbal, nonverbal, and paraverbal elements of adult behavior have been suggested as influential variables to consider in the process of child co-regulation (146). Lastly, the exclusive effectiveness of clown therapy on self-reported fear levels could suggest that it primarily acts on cognitive or emotional pain pathways, rather than on nociceptive pain pathways (86, 147).
Physiological and biological markers
The impact of the intervention on biomarkers of stress levels were mixed and largely dependent on the specific biomarker assessed and the timing of assessment, with the most impact observed post-intervention for heart rate and blood pressure. Informational videos were highly effective in reducing post-procedural heart rate and systolic and diastolic blood pressure (62), which is consistent with literature highlighting the sustained calming effects of cognitive preparation provided by informational videos (148, 149). This reduction in heart rate supports the notion that these videos promote parasympathetic recovery by helping children feel more prepared and less anxious about the procedure. This finding is consistent with previous studies were cognitive distraction through videos or educational content effectively lowered anxiety and, consequently, physiological stress markers such as blood pressure (150). Conversely, VR glasses significantly increased heart rate post-procedure (58). These mixed findings align with previous discussions on how VR can potentially induce sensory overload, which activates the sympathetic nervous system and raises heart rate (151, 152). Interestingly, the MDT also significantly increased heart rate post-procedure (86), which could be explained by the toy's engaging and dynamic nature, which provides distraction while potentially also increasing arousal in children, leading to sympathetic activation. Other interventions such as Buzzy or vibration, listening to music, and VR during the procedure showed no significant changes in heart rate or blood pressure, suggesting that their effects might be insufficient to counteract the autonomic responses to stress during the procedure itself (58, 73).
Lastly, limited evidence was available for SpO₂, respiratory rate, and plasma cortisol, showing inconclusive results for oxygen saturation and no significant alterations in plasma cortisol or respiratory rate. This highlights the need for more investigations on these biomarkers. The absence of significant effects on respiratory frequency (58) aligns with previous studies, where interventions such as distraction or sensory modulation failed to significantly affect respiratory frequency, possibly due to the short duration of the procedure or the mild intensity of the intervention (73, 150). Similarly, the lack of impact on cortisol levels could reflect the complexity of stress hormone modulation during medical interventions. On one hand, cortisol, a marker of hypothalamic–pituitary–adrenal (HPA) axis activation, may require more robust or prolonged interventions to produce significant changes, particularly in acute contexts such as medical procedures (144, 153). On the other hand, since the only study assessing cortisol levels used plasma samples, a method that may be less sensitive to subtle or transient stress responses compared with salivary or capillary cortisol, the absence of significant findings may also be due to methodological measurement factors.
Clinical implications for PEDs
This systematic review and meta-analysis provide guiding results for the implementation of psychological and sensory interventions in PEDs. The main clinical implications, mechanisms of action, and recommended applications for each intervention type are summarized in Table 4. Protocols for effectively managing pain, fear, and distress in pediatric emergencies should consider the use of: (a) preparatory strategies (such as informational videos) to facilitate an initial modulation of the cognitive evaluation of the upcoming experience; (b) somato-sensory devices during venipuncture to activate the ascending pain modulation pathways; and (c) complementary distraction strategies, whether through the stimulation of cognitive and/or emotional processes that promote descending pain modulation. When selecting descending pain modulation interventions, it is recommended to consider the child's cognitive and sensory processing capacity, as well as the cognitive load involved in the intervention.
In particular, the use of VR may overwhelm the vestibular and proprioceptive systems in infants and preschoolers. In these cases, simpler distraction strategies, such as screens, robots, or manipulable toys, are recommended. Further, at the preschooler age, sensory, emotional, and cognitive processes are dependent on adult behavior, highlighting the importance of involving caregivers with co-regulation strategies (154). Unfortunately, there is limited evidence regarding which specific co-regulation behaviors are effective in PED. For school-aged children, considering their still-developing systems, it is essential to make specific adjustments based on the level of interaction and type of VR content to ensure more effective pain and fear modulation (124, 127). In adolescents, there are less risk considerations related to their already developed sensory, vestibular, and proprioceptive systems (155). It is also important to allow adolescents to actively participate in choosing the intervention, as this promotes autonomy and a sense of control over their pain experience (156).
Methodological limitations and future research
Despite the robustness of the findings, this meta-analysis is not without limitations. First, the high levels of heterogeneity observed indicate significant variability in study designs, intervention implementation, and outcome measures. This variability limits the generalizability of the findings and underscores the need for more standardized methodologies for both intervention design and outcome assessment in future research. Secondly, only articles published in English or Spanish were included, which could reduce the generalizability of the findings. Thirdly, the effectiveness of interventions on pain, fear, and distress outcomes was assessed exclusively during the invasive medical procedure, which may limit the interpretation of effects across different procedural phases. Interventions that did not yield significant results during the procedure might show efficacy in pre-procedural preparation or in facilitating post-procedural stress recovery. Fourth, most of the included studies do not include individual variables (previous pain experiences, central sensitivity, catastrophizing, attentional bias to pain, etc.) which could impact children's stress and the effectiveness of the interventions (28, 31–35, 157). Should all be considered cross the board to adopt a personalized approach that adjusts the intervention based on the patient's needs (158, 159).
Fifth, it is noteworthy that most interventions included in this review were implemented by healthcare professionals, with only one study (82) directly focusing on parental behaviors as the main component of the intervention. Conversely, only one study (69) explicitly excluded caregiver presence from the intervention group, considering that such presence could act as a non-pharmacological method to reduce children's anxiety and, therefore, represent a potential source of bias. This distinction underscores the importance of differentiating between active caregiver variables (behaviors) and passive variables (presence or absence). In this context, caregiver presence or absence emerges as a relevant yet scarcely explored factor, whose independent contribution to children's stress modulation warrants further investigation. Given that the inclusion criteria of this review prioritized active psychological and sensory interventions, future research should aim to disentangle the individual and combined effects of active caregiver behaviors and passive presence to better understand their respective roles in children's adaptive responses during IMPs.
Sixth, achieving blinding in psycho-sensorial interventions presents inherent challenges. The active involvement of children, caregivers, and healthcare professionals is integral to most interventions, making it practically impossible to fully blind the intervention's nature (160). Participants are consciously aware of both the activities performed and the intended objectives, which may introduce demand biases and skew outcomes positively. Social interventions, in particular, present added variability in delivery due to their interactive and adaptive nature. Given the difficulty of ensuring full blinding and standardizing application in psychological interventions, alternative methods are crucial for enhancing methodological rigor. Emphasizing blinding of outcome evaluators (50, 73, 90) and data analysts (80) may offer a feasible approach. Partial blinding strategies could also be used, where participants, although aware they are receiving an intervention, are not informed of the exact study objectives and hypotheses. Additionally, they may be kept unaware of whether they are in a specific “experimental” or “control” group when more than one intervention group or a control condition with minimally effective psychological or sensory strategies is included. For social interventions, consistent training of providers, structured response protocols for varying interaction scenarios, and fidelity assessments during intervention delivery can improve consistency and minimize potential deviations.
Seventh, although some studies reported physiological or biological, these were treated as secondary complementary outcomes to the main emotional or behavioral measures. This approach aligns with the review's focus on children's pain, fear, and distress as the core responses to procedural stress. While limited in scope, this inclusion allowed for an initial approximation of the physiological dimension of procedural stress and its potential modulation by psychosensory interventions. However, the available data were highly heterogeneous across studies, making it necessary to interpret these results with caution. Future research could benefit from integrating standardized physiological and biochemical measures to provide a more comprehensive psychophysiological understanding of stress regulation in pediatric IMPs.
Finally, given the high heterogeneity observed (I^2^ > 90%), results should be interpreted with caution. A random-effects model was applied a priori to address variability in intervention formats and study designs. Although subgroup analyses were pre-planned, only the classification by psychosensory subtype was feasible due to insufficient stratified data. In addition, no sensitivity or meta-regression analyses were conducted, which limits the assessment of result stability and potential moderators. This decision aimed to preserve statistical power given the small number of studies per category. Moreover, the geographical concentration of studies—primarily conducted in Turkey, Canada, and the United States—may have contributed modestly to between-study variability and limits the generalizability of findings to other healthcare contexts. Future meta-analyses with larger, more geographically diverse, and methodologically homogeneous datasets should include sensitivity and meta-regression analyses to explore sources of heterogeneity and confirm the robustness of these findings.
Concluding remarks
In summary, this systematic review and meta-analysis suggest that a broad range of psychological and sensory interventions may reduce pain, fear, and distress during procedures in PED, as well as in some post-procedural biological markers. Pre-procedural preparation and procedural distraction appear to be key strategies for modulating these responses, addressing the sensory, cognitive, and emotional components of pediatric procedural pain. However, given the high heterogeneity among studies and the absence of meta-regression or sensitivity analyses, these findings should be interpreted with caution. Despite these limitations, the current evidence provides a preliminary useful foundation for developing clinical protocols aimed at optimizing the experience of children and adolescents in PED settings and minimizing long-term consequences, both psychological and somatosensory.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Price J Kassam-Adams N Alderfer MA Christofferson J Kazak AE. Systematic review: a reevaluation and update of the integrative (trajectory) model of pediatric medical traumatic stress. J Pediatr Psychol. (2016) 41:86–97. 10.1093/jpepsy/jsv 07426319585 · doi ↗ · pubmed ↗
- 2Cozzi G Cognigni M Busatto R Grigoletto V Giangreco M Conte M Adolescents’ pain and distress during peripheral intravenous cannulation in a paediatric emergency setting. Eur J Pediatr. (2022) 181:125–31. 10.1007/s 00431-021-04169-x 34218317 PMC 8760195 · doi ↗ · pubmed ↗
- 3Hitchcock C Goodall B Wright IM Boyle A Johnston D Dunning D The early course and treatment of posttraumatic stress disorder in very young children: diagnostic prevalence and predictors in hospital-attending children and a randomized controlled proof-of-concept trial of trauma-focused cognitive therapy for 3- to 8-year-olds. J Child Psychol Psychiatry. (2022) 63:58–67. 10.1111/jcpp.1346034128219 · doi ↗ · pubmed ↗
- 4Wingler D Liston D Joseph A Wang Y Feng H Martin L. Perioperative anxiety in pediatric surgery: induction room vs. operating room. Paediatr Anaesth. (2021) 31:465–73. 10.1111/pan.1409833278852 · doi ↗ · pubmed ↗
- 5Marcev I Lannon-Boran C Hyland P Mc Hugh Power J. The factors associated with paediatric medical post-traumatic stress: a systematic review. J Health Psychol. (2025) 30(11):2860–2880. 10.1177/1359105324127221439344541 PMC 12433540 · doi ↗ · pubmed ↗
- 6Ratnapalan S Cieslak P Mizzi T Mc Evoy J Mounstephen W. Physicians’ perceptions of background noise in a pediatric emergency department. Pediatr Emerg Care. (2011) 27:826–33. 10.1097/PEC.0b 013e 31822 c 135721878828 · doi ↗ · pubmed ↗
- 7Joseph MM Mahajan P Snow SK Ku BC Saidinejad M Optimizing pediatric patient safety in the emergency care setting. Pediatrics. (2022) 150:e 2022058158. 10.1542/peds.2022-05967336189487 · doi ↗ · pubmed ↗
- 8Haas R Brundisini F Barbara A Darvesh N Ritchie L Mac Dougall D Emergency department overcrowding: an environmental scan of contributing factors and a summary of systematic review evidence on interventions. Can J Health Technol. (2023) 3(11). 10.51731/cjht.2023.78638320062 · doi ↗ · pubmed ↗