KIT Mutant/Core binding factor-negative acute myeloid leukemia might be a complex subgroup with dismal prognosis: a single-center retrospective analysis
Rui Jiang, Zhibo Zhang, Yizi Liu, Wenqiang Qu, Zhao Zeng, Linlin Wang, Qian Wang, Jia Yin, Suning Chen

TL;DR
This study finds that KIT mutant/CBF-negative AML is a complex and high-risk leukemia subgroup with poor survival outcomes.
Contribution
The study characterizes the clinical and molecular features of KIT mutant/CBF-negative AML, highlighting its poor prognosis.
Findings
KIT mutant/CBF-negative AML patients had a median event-free survival of 15.3 months and overall survival of 24.1 months.
KIT exon 17 mutations were associated with worse survival outcomes.
Allogeneic hematopoietic stem cell transplantation improved survival in these patients.
Abstract
KIT mutations are well-established as poor prognostic markers in core binding factor AML (CBF AML). However, data on KIT mutation in CBF-negative (CBF-neg) AML remains scarce. This retrospective study aimed to characterize the clinical features and outcomes of patients with KIT mutant (KIT mut)/CBF-neg AML. We conducted a retrospective study in our single center and identified non-M3 de novo AML with KIT mutations by next-generation sequencing (NGS) from January 2018 to June 2024. Core binding factor (CBF) AML or patients with underlying systemic mastocytosis were excluded. The clinical data of KIT mut/CBF-neg AML was collected and analyzed. 45 patients were enrolled in the cohort, including 3 patients with secondary AML. The median variant allele frequency (VAF) of KIT mutation was 41.2% and the most frequent comuations were CEBPA (27/45, 60%), WT1 (12/45, 26.7%) and NRAS (11/45,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
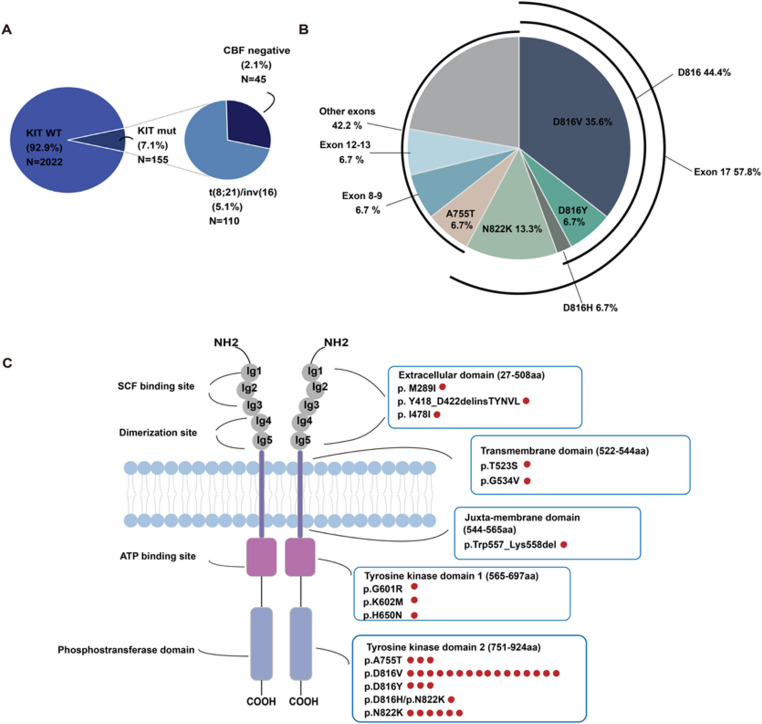 Figure 1
Figure 1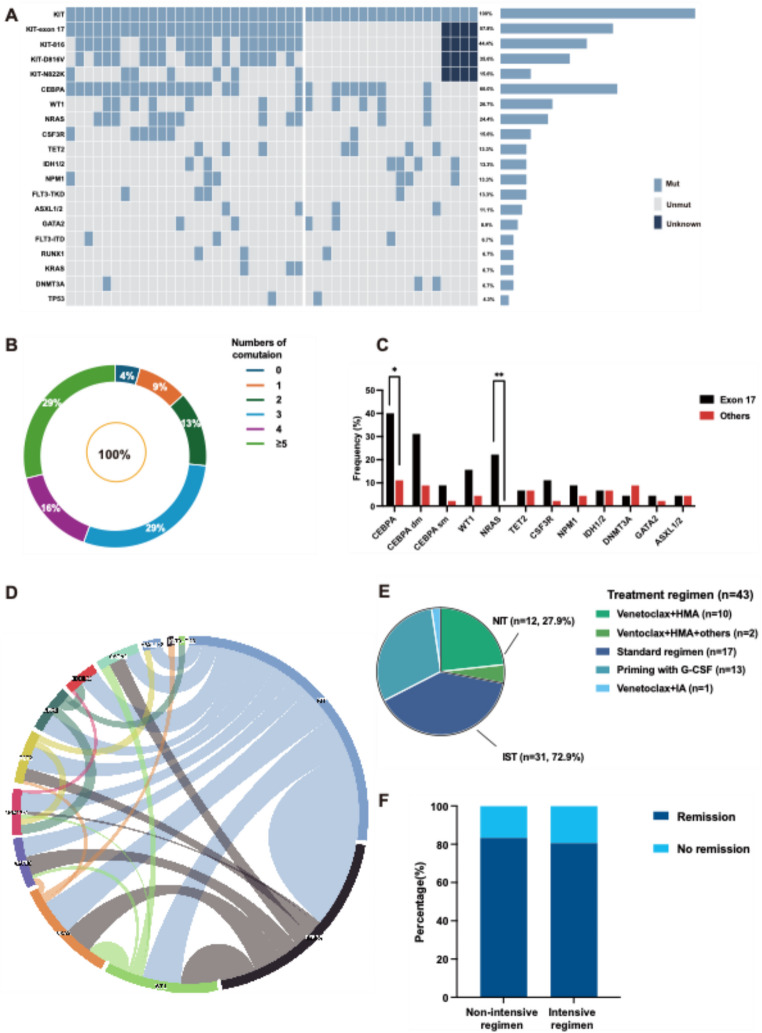 Figure 2
Figure 2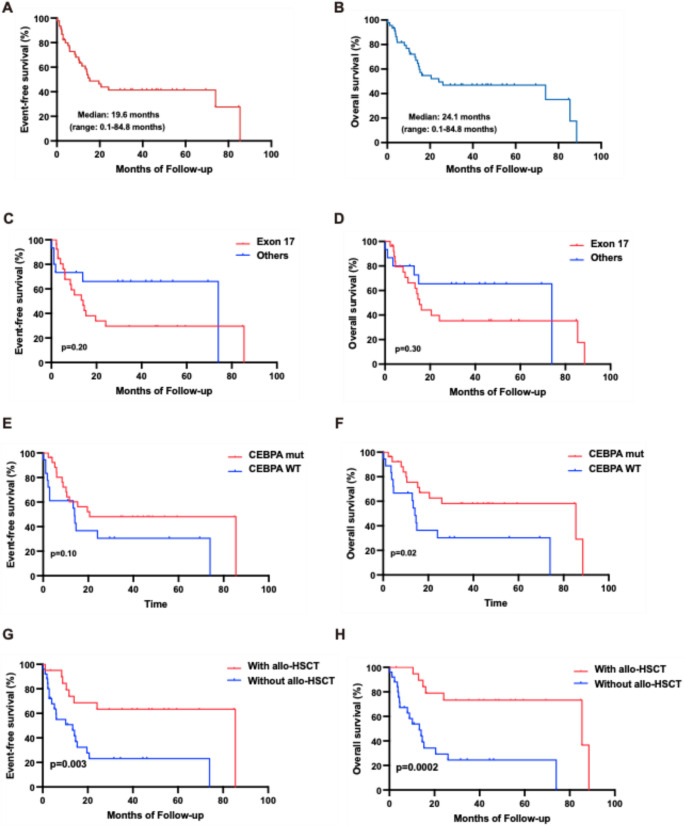 Figure 3
Figure 3- —https://doi.org/10.13039/501100012166National Key Research and Development Program of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Mast cells and histamine · Myeloproliferative Neoplasms: Diagnosis and Treatment
Introduction
KIT, also known as stem cell factor (SCF) receptor, is one of prominent member in the family of Type III tyrosine kinase receptor [1]. The KIT gene is a proto-oncogene located at the 11 locus of long arm of chromosome 4 [2], and the gene product physiologically is involved in cellular proliferation and survival, cell differentiation, chemotaxis and activation of gene transcription, by participating in several signaling pathways, including PI3K pathway, JAK/STAT pathway, Src pathway and MAPK pathway [1–6].
KIT dysfunction, induced by gain-of function mutations, plays an important role in tumorigenesis and progression. It has been reported KIT mutation occurred in several solid cancers, including thymic cancer, breast cancer and gastrointestinal stromal tumor (GIST) [1, 7]. In myeloid neoplasms (MNs), KIT mutation is primarily correlated with systemic mastocytosis (SM), with 90% patients harboring activating mutation and KIT D816V occurred most frequently [8]. Aside from SM, acute myeloid leukemia (AML) was the most common MNs with KIT mutation, which was detected in 4%−6% de novo AML [9, 10], most frequently occurred in core binding factor AML (CBF AML).
Previous study has primarily focused on the prognosis of KIT mutation in CBF AML. It has been well established that KIT mutation was one of poor prognostic factors in CBF AML treated by intensive chemotherapy. Moreover, KIT exon 17 mutations were associated with unsatisfactory survival outcome in patients with RUNX1::RUNXT1 AML receiving hypomethylating agents (HMA) [11]. However, less attention has been given to CBF-negative (CBF-neg) AML, resulting in a lack of understanding regarding the distribution and prognosis of KIT mutation in the specific population. Consequently, we performed a retrospective study on patients with KIT mutant (KIT mut)/CBF-neg AML and investigated the clinical characteristics, treatment procedures and survival to provide preliminary clues into the individual treatment strategy of the subgroup.
Materials and methods
Patients
A total of 45 newly-diagnosed, non-M3 AML patients who presented KIT mutation via next-generation sequencing (NGS), without fusion gene RUNX1::RUNXT1 or CBFB::MYH11 detected by conventional cytogenetic analysis or RT-PCR between January 2018 and June 2024 in our single center were retrospectively analyzed. As KIT activating mutation or KIT D816V is one of diagnostic criteria in SM based on the 5th edition of the World Health Organization classification of MNs [12], patients with evidence of underlying SM were excluded (see Supplemental Fig. 1). This study was approved by the responsible ethics committees and performed in accordance with the Declaration of Helsinki. Informed consent was obtained from all patients involved in the study.
Treatment procedures and measurable residual disease (MRD) assessment
Forty-three patients received at least one cycle of induction therapy and were included for response assessment. Induction therapy was classified into two groups: non-intensive therapy (NIT) and intensive therapy (IST). NIT included venetoclax + HMA (decitabine or azacytidine) ± others (homoharringtonine or all-trans-retinoic acid). IST included standard regimen [IA (idarubicin, cytarabine) and DA (daunorubicin, cytarabine) ± venetoclax and priming regimen, including IAG [idarubicin, doxorubicin, cytarabine, human granulocyte colony stimulating factor (G-CSF)], HAAG (homoharringtonine, doxorubicin, cytarabine, G-CSF) and ECAG (aclarubicin, doxorubicin, cytarabine and G-CSF). Response assessment was conducted according to the 2022 recommendation of the European LeukemiaNet (ELN 2022) [13]. MRD assessment was performed by multiparameter flowcytometry or quantitative PCR (qPCR). MRD negativity was defined as < 0.1% CD45-expressing cells. NPM1 > 0.2% variant allele frequency (VAF) detected by qPCR was considered MRD positive [14]. Twenty patients underwent allogeneic hematopoietic stem cell transplantation (allo-HSCT).
Survival definition and statistical analysis
Event-free survival (EFS) was calculated from the date of diagnosis as AML to the date of treatment failure, relapse or death induced by any cause, whichever happened first, and relapse-free survival (RFS) was calculated from the date of remission to the date of relapse or death, whichever happened first. Overall survival (OS) was defined as the duration between the date of diagnosis and the date of death.
Categorical variables were summarized using numbers (proportion) and compared with Chi-square test and Fisher’s exact test. Continuous variables were summarized using median (range) and compared with Mann-Whitney test. Survival curves were constructed with Kaplan-Meier method and survival analysis between different subgroups was conducted by Log-rank test. Predictors for EFS and OS was performed by univariate Cox hazard analysis and multivariable analysis selected variables with p value of < 0.1 in univariate analysis and clinical significance. The proportional hazards assumption was assessed using Schoenfeld residuals and log-minus-log plots, and no significant violation was observed. P value of < 0.05 was considered statistically significant. IBM SPSS 26.0 and Graphpad Prism 9 were used for statistical analysis.
Results
Incidence, type and location of KIT mutation in KIT mutant/CBF-neg AML
From January 2018 to June 2024, we reviewed 2, 177 patients diagnosed as AML and detected 155 patients (7.1%) with KIT mutation by NGS, including 110 (5.1%) patients with fusion gene RUNX1::RUNXT1 or CBFB::MYH11 and 45 patients (2.1%) without such fusion gene (Fig. 1A). By further analysis of the 45 KIT mut/CBF-neg patients, the most common mutation was at exon 17 (26/45, 57.8%). KIT D816V was most frequently seen with an incidence of 35.6% (16/45), followed by KIT N822K with a percentage of 13.3% (7/45) (Fig. 1B). Furthermore, we noted D816H was in coexistence with N822K in one patient (Fig. 1C).Fig. 1. Characteristics of KIT mutation in 45 KIT mut/CBF-neg AML (A) Distribution and frequency of KIT mutation in de-novo AML. (B) Pie chart showing type and frequency of KIT mutation in the 45 patients. (C) Schematic representation of KIT domains depicting type and number of mutations of the cohort
Clinical characteristics
The median age at diagnosis of 45 patients with KIT mut/CBF-neg was 46 years old (range: 17–74 years old), including 3 patients with secondary AML, among which one patient was diagnosed as therapy-related AML and two patients progressed from MDS and MPN, respectively. Twenty-six patients (26/45, 57.8%) exhibited normal karyotype, six patients (6/45, 13.3%) exhibited myelodysplasia-related cytogenetic abnormalities, and 2 patients (2/45, 4.4%) presented KMT2A rearrangement. Fourty-three patients were available for analysis of ELN 2022 risk stratification at diagnosis: 46.5%, 30.2% and 23.3% in favorable, intermediate, and adverse, respectively. The detailed clinical characteristics of the cohort was listed in Table 1.
Table 1. Clinical characteristics of 45 KIT mutant/core binding factor (CBF)-negative (CBF neg) AML patientsVariablesAll patients (n = 45)Sex, n (%)Male30 (66.7)Female15 (33.3)AML type, n (%)De novo42 (93.3)Secondary3 (6.7)Age (years), median (range)46 (17–74)CBC at diagnosis, median (range)WBC, ×10^9^/L41.7 (2.8–239.5.8.5)Hb, g/L89 (48–134)PLT, ×10^9^/L30 (3–1466)BM blast (%), median (range)65 (13–92)KMT2A rearrangement, n (%)2 (4.4%)AML with MRC, n (%)13 (28.9%)ELN 2022 risk stratification (n = 43), n (%)Favorable20 (46.5)Intermediate/Adverse23 (53.5)KIT mutational site, n (%)KIT−81620 (44.4)KIT-D816V16 (35.6)KIT-N822K7 (15.6)Comutations, n (%) CEBPA 27 (60) NPM1 6 (13.3)FLT3-ITD3 (6.7)FLT3-TKD3 (6.7)IDH1/26 (13.3) TP53 2 (4.4)ANC absolute neutrophil count, *BM *bone marrow, *CBC *complete blood count, *Hb *hemoglobin, *MRC *myelodysplasia-related changes, *PLT * platelet, WBC white blood cell count
Comutations
The mutational profile of 45 patients with KIT mut/CBF-neg was depicted in Fig. 2A. The median variant allele frequency (VAF) of KIT mutation was 41.2% (range: 1%−64.5%) and the median number of comutations except KIT mutation was three (range: 0–7). The most common mutated genes were CEBPA (27/45, 60%), WT1 (12/45, 26.7%), NRAS (11/45, 24.4%), TET2 (7/45, 15.6%), CSF3R (6/45, 13.3%), NPM1 (6/45, 13.3%), IDH1/2 (6/45,13.3%), DNMT3A (6/45, 13.3%) and GATA2 (5/45, 11.1%) (Fig. 2A). Compared with CBF AML, CEBPA, WT1, NPM1 and IDH1/2 cooccurred more frequently in KIT mut/CBF-neg AML with statistically significance (see Supplemental Fig. 2**)**. Furthermore, among patients with CEBPA comutations, 74.1% (20/27) harbored CEBPA^dm^. Twenty-five patients were available for further analysis of mutational sites, including seventeen patients (44.4%, 17/25) with bZIP in-frame (bZIP-inf) mutations (see Supplemental Fig. 2). Only 4.4% (2/45) patients showed single KIT mutation, including one patient solely with KIT D816V and the other with deletion/insertion of extracellular domain. Most patients (39/45, 86.7%) exhibited more than two comutations except KIT, among which 28.8% (13/45) possessed more than 5 comutations (Fig. 2B).
Fig. 2. Co-mutation analysis, treatment disposition and response assessment of the cohort (A) Mutational landscape of 45 KIT mut/CBF-neg AML. Each column represents one patient, and each line represents one gene. (B) Proportions of the number of comutations of the cohort. (C) Comparison of the frequencies of comutations between patients with KIT exon 17 mutation (n = 26) and with others (n = 15). Comparisons were made by Chi-square test and Fisher’s exact test and considered statistically significant at p values less than 0.05. (D) Circos program of the co-occurrence and frequency of mutational genes. (E) Distributions of induction therapy with various treatment procedures. (F) Bar chart showing the rate of remission of induced with non-intensive therapy (NIT) (n = 12) and intensive therapy (IST) (n = 31). * p < 0.05; ** p < 0.001
Comparison of baseline clinical features between patients with KIT exon-17 mutation and with others
Considering exon 17 was the major mutant site in AML as reported before [15, 16], we further divided 41 patients, available for analysis of KIT mutation site, into two groups: patients with exon 17 (n = 25) and others (n = 16) and made comparison between the subgroups (Table 2). The proportion of male was significantly higher in patients with exon 17 (76.9% vs. 40.0%, P = 0.04). Meanwhile, patients with KIT exon 17 showed a significantly lower median VAF (29.1% vs. 48.3%, P = 0.0005). Additionally, the frequency of several somatic mutations was relatively higher in the subgroup of patients with exon 17, including CEBPA, WT1, NRAS, CSF3R and NPM1 (Fig. 2C and D), among which the incidence of CEBPA and NRAS was significantly higher in patients with exon 17 (CEBPA: 40.0% vs. 11.1%, p = 0.025; NRAS: 22.2% vs. 0.0%, p = 0.006) (Fig. 2C).
Table 2. Clinical characteristics between patients with KIT-exon 17 and othersVariablesExon 17 (n = 26)Others (n = 15) p Male, n (%)20 (76.9)6 (40.0) 0.04 Age (years), median (range)57 (17–74)47 (18–65)0.38CBC at diagnosis, median (range)WBC, ×10^9^/L51.5 (3.2–239.5.2.5)6.7 (0.3–48.7) < 0.001 Hb, g/L92 (34–129)83 (57–119)0.72PLT, ×10^9^/L29 (8–1466)52 (8–175)0.19BM blast (%), median (range)65 (15–88)51 (13–92)0.49KIT VAF (%), median (range)29.1 (2.1–64.5)48.3 (4.1–63.8) 0.0005 ELN 2022 risk stratification, n (%)0.30Favorable8 (30.8)3 (20.0)Intermediate10 (38.5)6 (40.0)Adverse4 (15.4)6 (40.0)Gene mutation, n (%) CEBPA 18 (69.2)5 (33.3) 0.02
NRAS 10 (38.5)0 (0.0) 0.0067
NPM1 4 (15.4)2 (13.33)> 0.99Induction regimen, n (%) 0.03 NIT4 (15.4)7 (46.7)IST21 (80.8)7 (46.7)Allo-HSCT, n (%)9 (34.6)8 (50)0.35*Allo-HSCT *allogeneic hematopoietic stem cell transplantation, *IST *intensive therapy, *NIT *non-intensive therapy (NIT), *VAF *variant allele frequency
Treatment disposition and response rate
Two patients refused to receive induction therapy and were excluded for response assessment. Forty-three patients received at least one cycle of induction therapy and available for response assessment: 27.9% (12/43) patients received NIT, including ten patients receiving venetoclax and HMA, and the others (31/43, 72.1%) received IST. The proportion of various induction regimen was depicted in Fig. 2E. Comparisons of baseline clinical features, response and MRD assessment between patients with different treatment disposition were listed in Supplemental Table 1. The rate of complete remission (CR) after induction therapy was comparable between patients with NIT and with IST (83.3%, 10/12 vs. 80.6%, 25/31) (Fig. 2F). Thirty-four patients were available for MRD analysis after one cycle of induction therapy. 47.1% (16/34) patients achieved MRD negativity, including ten patients with NIT after one cycle. Twenty patients (44.4%) patients underwent subsequent allo-HSCT, including 5 patients who failed to maintain remission and collapsed after a median time of 10.6 months (range: 5.1–18 months) since allo-HSCT.
Survival and prognostic analysis
The last follow-up was completed by December 2025. With a median follow-up of 48 months, the median EFS and OS of the cohort were 15.3 months (range: 0.1–85.4 months) (Fig. 3A) and 24.1 months (range: 0.1–88.5 months) (Fig. 3B). Patients with KIT mutation at exon 17 showed an inferior EFS (median: 14.1 vs. 74 months) (Fig. 3C) and OS (median: 15.3 vs. 74 months) (Fig. 3D) in comparison with other sites. Moreover, patients with KIT exon-17 mutation harbored a significantly poor RFS (median: 12.2 vs. 72.2 months; P = 0.03) (see supplemental Fig. 4). Meanwhile, patients with CEBPA mutation appeared to have an advantage of EFS (median: 20.6 vs. 13.9 months; P = 0.10) over those with wildtype [17] (Fig. 3E), while a significantly superior OS was seen in the subgroup of patients with CEBPA comutation (median: 85.4 vs. 14.1 months; P = 0.02) (Fig. 3F). Furthermore, patients with CEBPA bZIP in-frame mutations (bZIP-inf) showed superiority of EFS and OS over patients with CEBPA WT [17]. However, no obvious difference of survival was seen between patients with CEBPA bZIP-inf and with other mutational sites (see supplemental Fig. 5). There was no significant difference of OS and EFS between patients with NPM1 mutation and NPM1 WT despite a superior EFS in patients with NPM1 mutation (see supplemental Fig. 5). According to ELN2022 risk stratification, patients with favorable risk harbored an advantage of EFS and OS over patients with intermediate or adverse (median EFS: 85.4 months vs. 13.9 months, P = 0.11; median OS: 85.4 vs. 14.6 months, P = 0.03) (see supplemental Fig. 5). Allo-HSCT significantly improved EFS (median: 85.4 vs. 13.9 months; P = 0.003) (Fig. 3G) and OS (median: 85.4 vs. 14.6; p = 0.0002) (Fig. 3H) in the cohort.
Fig. 3. Survival analysis of the cohort (A-B) Kaplan-Meier curves of event-free survival (EFS) and overall survival (OS) of 45 KIT mut/CBF-neg AML. (C-D) Kaplan-Meier curves of EFS and OS of patients with KIT exon 17 mutation and with others. (E-F) Kaplan-Meier curves of EFS and OS of patients with CEBPA mutation and WT. (G-H) Kaplan-Meier curves of EFS and OS of patients with allogeneic hematopoietic stem cell transplantation (allo-HSCT) and without
We further performed univariate and multivariate cox regression analysis to better clarify the cohort (Tables 3 and 4), and identified TP53 mutation at diagnosis was an independent risk factor (EFS: hazard ratio [HR], 11.15 [95% CI: 2.12–58.72], P = 0.004; OS: HR, 8.75 [95% CI: 1.41–54.45], P = 0.02) while allo-HSCT was an independent protective factor (EFS: HR, 0.34 [95% CI: 0.13–0.87], P = 0.025; OS: HR, 0.18 [95% CI: 0.05–0.71], P = 0.014). Moreover, NPM1 mutation was an independent risk factor for EFS (HR: 4.19 [95% CI: 1.47–11.96], P = 0.007) while intermediate or adverse risk stratified by ELN 2022 was an an independent risk factor for OS (HR: 4.23 [95% CI: 1.05–17.17], P = 0.043). We identified CEBPA mutation as a significant protective factor (HR: 0.39 [95% CI: 0.17–0.89], P = 0.026) and NPM1 mutation as a significant risk factor (HR: 3.30 [95% CI: 1.08 ~ 10.06], P = 0.04) for OS in univariate analysis, but not significant in multivariate analysis.
Table 3. Univariate and multivariate Cox regression analysis of event-free survival (EFS)VariablesUnivariateMultivariateHazard ratio(95% CI) p Hazard ratio(95% CI) p Male1.34 (0.56–3.22)0.51Age1.01 (0.98–1.03)0.60WBC1.00 (0.99–1.00.99.00)0.26Secondary AML1.05 (0.25–4.45)0.95Intermediate/adverse risk^^1.92 (0.84–4.35)0.12KIT* exon 17 mut1.83 (0.72–4.68)0.21CEBPA mut0.53 (0.25–1.20)0.13CEBPA bZIP-inf mut0.84 (0.37–1.91)0.68NPM1mut 4.1 (1.47–11.42)
0.007
4.19 (1.47–11.96)
0.007 TP53 mut 12.27 (2.46–61.30)
0.002
11.15 (2.12–58.72)
0.004 Allo-HSCT 0.29 (0.12–0.70)
0.006
0.34 (0.13–0.87)
0.025 bZIP-inf: bZIP in-frame mutations; ^*^: stratified by ELN 2022
Table 4. Univariate and multivariate Cox regression analysis of overall survival (OS)VariablesUnivariateMultivariateHazard ratio(95% CI) p Hazard ratio(95% CI) p Male1.05 (0.43–2.57)0.92Age1.01 (0.98–1.04)0.40WBC1.00 (0.99–1.00.99.00)0.65Secondary AML1.32 (0.31–5.65)0.71Intermediate/adverse risk^*^ 2.50 (1.02–6.09)
0.04
4.24 (1.05–17.17)
0.04 KIT exon 17 mut1.65 (0.64–4.27)0.31CEBPA mut 0.39 (0.17–0.89)
0.03 1.43 (0.42–4.89)0.57CEBPA bZIP-inf mut0.65 (0.27–1.59)0.35NPM1mut 3.30 (1.08 ~ 10.06)
0.04 2.05 (0.54 ~ 7.73)0.29TP53 mut 23.77 (3.91–144.42.91.42)
< 0.001
8.75 (1.41–54.45)
0.02 Allo-HSCT 0.18 (0.07–0.50)
0.001
0.18 (0.05–0.71)
0.014 ^*^: stratified by ELN 2022
Discussion
Here we reported the distribution of KIT mutation in CBF-neg AML and clarified the clinical characteristics and prognosis of the subgroup. Our results indicated that KIT mut/CBF-neg AML might possess a dismal survival, regardless comutation and allo-HSCT might benefit the underestimated populations.
It has been an important issue concerning the prognosis of KIT mutation in AML, especially in CBF-AML, including AML with RUNX1::RUNXT1 and CBFB::MYH11. The incidence of KIT mutation was approximately 4%−6% in AML [9, 10], which frequently occurred in 10%−40% CBF-AML, with a poor survival in the subgroup of patients with RUNX1::RUNXT1 based on multiple retrospective and perspective clinical studies [11, 15, 18–22]. However, there was few research on KIT mutation in CBF-neg AML. A retrospective study preliminarily presented the distribution of KIT mutation in myeloid neoplasms, including 56% patients with CBF-neg AML and 45% with CBF-AML [16]. A real-word study showed that in comparison with CBF-AML, CBF-neg AML showed a superior survival with a 3-year OS of 77.3% and a 3-year DFS of 73.6%. However, the study failed to focus on the subgroup of KIT mut/CBF-neg AML, meanwhile, KIT mutation showed no prognostic significance in the study [23]. Whereas based on two AML independent databases, a retrospective study identified 17 KIT mut/CBF-neg AML with a poor median OS of 26.4 months. Recently, another study identified 16 patients of the subgroup and pointed out the subgroup showed extremely poor survival with a median OS of 9 months and a median RFS of 3.2 months, regardless comutations [24]. Consistent with the previous studies, our study indicated that KIT mut/CBF-neg AML was a specific subgroup and showed a poor prognosis with a median EFS of 15.3 months and a median OS of 24.1 months, despite most patients categorized into favorable-risk and intermediate-risk subgroup based on ELN2022.
In this study, we first depicted the clinical features and the mutational landscape of KIT mut/CBF-neg patients in AML. Three secondary AML was included and by further analysis, secondary AML was not significantly associated with EFS and OS in our univariate analysis. Several studies reported that the incidence of CEBPA mutation was relatively low in adult patients with CBF AML, approximately 1% [21, 23]. Unlike that in CBF AML, CEBPA mutation seemed to be more frequent in CBF-neg AML, with an incidence of 36.4% according to a retrospective study [23]. In line with that, our study discovered that over 50% of the subgroup presented CEBPA mutation. By further analysis, it was unexpected that patients with CEBPA appeared to attain a superior survival in the subgroup and CEBPA mutation had a significantly positive impact on OS, which was not mentioned in the previous study. Moreover, the incidence of NPM1 mutation was relatively lower in our cohort than that reported before, which was detected in 38% patients [24]. In our cohort, NPM1 showed a significantly negative impact on EFS and OS in univariate cox regression, which was inconsistent with Log-rank test, a possible explanation maybe a small sample size of NPM1 mutation in the rare group. However, the rarity of this co-mutation pattern means its implications remain to be fully elucidated. We noticed TP53 mutational status at diagnosis was negatively associated with EFS and OS although two patients in our cohort harbored TP53 mutation, one of which underwent a course of venetoclax plus decitabine as induction, achieved CR with undetectable MRD, received allo-HSCT after consolidation with intermediate dose cytarabine and maintained CR after a follow-up of 40.8 months while the other one received a course of venetoclax plus decitabine as induction, achieved CR but relapsed after 4.8 months and collapsed.
Aside from description of clinical characteristics, we preliminarily probed into the efficiency of induction therapy in the rare subgroup. We noticed a comparable remission rate between patients with NIT and IST however a relatively higher rate of MRD elimination in patients with NIT. Notably, one patient who received venetoclax in combination with IA as induction therapy remained remission after a follow-up of 34.5 months. A systemic review reported that there was a statistically significant superiority of survival in those who achieved MRD negativity. Moreover, in those who achieved morphological remission, MRD negativity was positively associated with disease-free survival (DFS) and OS [25]. Accordingly, our retrospective study provided preliminary evidence that venetoclax-based regimen might be an appropriate choice for the rare subgroup due to the achievement of a fast MRD elimination, which might make for future survival benefit.
Nonetheless, there might be some limitations in our study. First, the sample size of our cohort was small which might result in the instability of cox regression analysis and overestimated the influence of variables, for example NPM1 and TP53, a rare comutation pattern needed further study. Second, due to retrospective study, the choice of induction regimen and whether to perform allo-HSCT were dependent on physician and the economic condition of the patient. Moreover, a small sample size of NIT subgroup, we failed to perform propensity score–matched analysis and our findings should be considered exploratory. We performed the comparison of clinical features between patients with NIT and IST, and there was no evident imbalance between the two subgroups, except NPM1 mutation and KIT mutational site. It has been elucidated that NPM1 mutation was associated with favorable response rate and survival while KIT mutation was associated poorer survival in several real-word study of venetoclax plus HMA [26, 27]. Accordingly, a higher MRD elimination rate in NIT might be attributable to the higher incidence of NPM1 mutation. Due to the limited sample size in NIT subgroup, we might overstate the clinical effect and survival benefit of NIT, which might be ascribed to the imbalance in the rate of patients with KIT exon 17 mutation between NIT and IST and might partly explain the contradiction on the role of venetoclax-based regimen in KIT mut AML between our study and the previous study [28]. Moreover, our study failed to answer whether venetoclax-based regimen could induce a sustainable survival benefit in KIT mut/CBF-neg AML, which needs prospective study with large sample size and long-term follow-up.
In conclusion, our results indicated that KIT mut/CBF-neg AML was a complex subgroup, which might be overlooked in our clinical practice, presented various molecular biological features and harbored a dismal prognosis. Our findings raised a presumption that induction with venetoclax + HMA might be appropriate for those patients, which might induce an early MRD elimination and remission, subsequently bridging to allo-HSCT and attain a sustainable remission. Our research is limited due to small sample size base on a retrospective study from our single center. There is a great need in future to investigate the characteristics and treatment strategies of KIT mut/CBF-neg AML and develop new markers for monitoring MRD by conducting a large prospective study.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file 1 (DOCX 10.5 MB)
Supplementary file 2 (DOCX 28.0 KB)