Pregnancy in women with spinal muscular atrophy (SMA): maternal and neonatal outcomes with multi-speciality management
David Cohen, Melanie Nana, Nicholas Hart, Lindsay Arrandale, Con Kelleher, Catherine Nelson-Piercy

TL;DR
This study examines pregnancy outcomes in women with spinal muscular atrophy, showing that with specialized care, healthy births are possible.
Contribution
The paper presents the first reported successful pregnancy in a woman with SMA type-1 and emphasizes the importance of multi-specialty care.
Findings
Eight pregnancies in six women with SMA resulted in healthy live births, with six pre-term and two term deliveries.
Four women experienced respiratory function deterioration during pregnancy but mostly recovered postpartum.
Multi-specialty care improved outcomes, allowing some women to have successful second pregnancies.
Abstract
Spinal muscular atrophy (SMA) is a rare inherited disorder that results in skeletal muscle wasting and weakness with a varying degree of severity. Pregnancy is associated with several changes in respiratory muscle function and respiratory physiology, which can compromise breathing leading to complications during pregnancy and delivery. Pregnant women with SMA are therefore considered to be a high-risk obstetric group. Due to the rare nature of the condition, it is infrequently encountered in pregnancy and this highlights the clinical importance of reporting this current case series. We report, in this retrospective case series, the outcomes of eight pregnancies in six women living with SMA, including, to our knowledge, the first reported successful pregnancy in a woman with SMA type-1, managed in our tertiary multi-professional and multi-speciality centre. All pregnancies, over an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
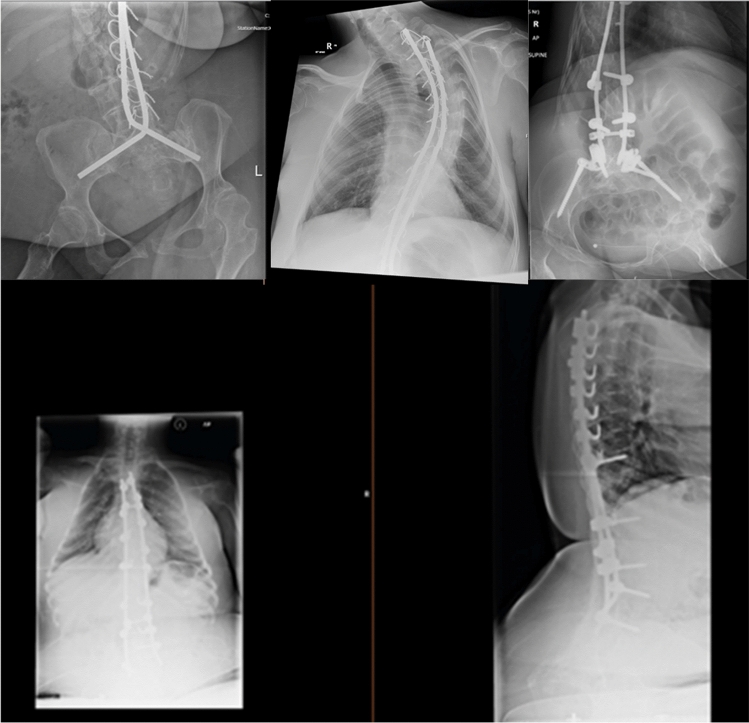 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurogenetic and Muscular Disorders Research · Cardiovascular Issues in Pregnancy · Nerve Injury and Rehabilitation
Introduction
Spinal muscular atrophy (SMA) is a rare genetic disorder with an incidence of 1 in 10,000 live births [1]. The condition leads to progressive loss of motor neurons in the ventral horns of the spinal cord, resulting in skeletal muscle wasting and weakness, particularly impacting locomotor and respiratory muscles. Although there are four types, type 1 SMA rarely progresses beyond childhood, whereas types 2, 3 and 4 are less severe and more slowly progressive [2]. Furthermore, with targeted nutritional support and respiratory support, for example non-invasive ventilation (NIV) to manage chronic respiratory failure, combined with advances in gene therapy and novel drugs, such as antisense oligonucleotide inhibitors, the life expectancy of individuals with SMA is increasing, with women reaching childbearing age [3, 4]. We report the management, maternal and neonatal outcomes of six women across eight pregnancies from our multi-professional, multi-specialty maternity unit.
Methods
A retrospective review of maternal and neonatal outcomes for all women living with SMA who received obstetric care at St Thomas’ Hospital in London between 2007–2025 was performed. Patients were identified from an anonymised database of women who received care under the obstetric medicine team. The multi-speciality team consists of an experienced obstetrician, obstetric medicine physician, obstetric anaesthetist and respiratory and critical care physician. All women identified were contacted and written informed consent was obtained for inclusion in this case series.
Maternal demographics, SMA type, functional status, maternal and neonatal outcomes, mode of delivery, gestation at delivery, anaesthetic details and neonatal outcomes were collected from hospital records. Where outcomes were not reported, patients were contacted via telephone. Primary outcomes of interest were maternal and neonatal morbidity and mortality as well as maternal respiratory deterioration. Secondary outcomes included pregnancy complications, mode of delivery, anaesthesia-related issues and neonatal health metrics.
Continuous variables were expressed as a mean ± standard deviation (SD) or median [interquartile range (IQR)], depending on normality of distribution of the data.
Results
Demographics and disease characteristics
Eight pregnancies in six women living with SMA were identified. Median maternal age at delivery was 29 ± 7 years. Six pregnancies were spontaneous, two were achieved with in vitro fertilisation (IVF)—both in the same woman, due to unexplained infertility. Demographics, including SMA type, are summarised in Table 1. Four out of the six women in our study have SMA type-2, one has SMA type-3, and one has SMA type-1. All women were wheelchair dependent prior to conception. Three women used home NIV pre-pregnancy. The woman with SMA type-1 who had not had a spinal fusion but had severe kyphoscoliosis and several fixed flexion deformities required modifications to her wheelchair to allow for growth of her pregnant abdomen. Table 1. Patient demographicsPatient IDPregnancyAge at delivery (years)SMA typeConceptionPPC11272SpontaneousNo22232SpontaneousYes33363SpontaneousYes44302SpontaneousYes35333SpontaneousYes56272IVFYes67241SpontaneousNo58342IVFYesSMA spinal muscular atrophy, PPC pre-pregnancy counselling (Pregnancies listed in chronological order)
Maternal and pregnancy outcomes
Four of the women received pre-pregnancy counselling (PPC) involving discussion around the impact of SMA on maternal health during pregnancy. Of the two who did not, one had an unplanned pregnancy, the second only had genetic counselling regarding the risk of any offspring inheriting SMA. The three women who used home NIV pre-pregnancy experienced a decline in their respiratory status as pregnancy progressed, as expected, requiring an increase in duration of NIV and/or change in NIV settings (inspiratory positive airways pressure and back up rate up-titrated). All were weaned back to pre-pregnancy settings of NIV within one month of delivery. Median gestational age at birth was 35 weeks and five days [IQR 6-7 days]. All were delivered by elective caesarean section under general anaesthetic after assessment by the multi-speciality team. Three women required awake fibreoptic intubation. Tables 2 and 3 summarise the maternal outcomes. Table 2. Maternal outcomes (Antenatal and Delivery)PregnancyRespiratory support pre-pregnancyAntenatal complications/admissionsHours of NIV support in antenatal periodMode of DeliveryAnaesthesia at deliveryPreterm labour/obstetric complication (PET, GDM, PPH)Delivery complications1NonePre-existing hypothyroidismNoneELCSGAGDM—diet controlledNo—received prophylactic antibiotics to prevent chest infection2Night NIV 10–12 h per night, cough assist as requiredpostpartum LRTINight NIV 10-12h per night, 3–4 h in the afternoon from 19 weeksELCSAwake fibreoptic intubation GANoNo3Noneinfluenzaovernight NIV from 33 weeks until deliveryELCSGANoBowel injury leading to 4 week ITU admission, developed respiratory distress. Poor post-op surgical wound healing—VAC dressing for 4 months4NoneLRTI at 35 weeks—admitted for 1 night—no NIV requiredNoneELCSAwake fibreoptic intubation GANoNo5NoneH1N1 infections × 2, ITU admission for pneumoniaNIV while inpatient with respiratory infectionELCSGANoNo6Night NIV + cough assist—low adherence 1 st trimester chest infection—no admissionFrom 19 weeks NIV at night and as required during the day. Weekly cough-assist use in last trimester of pregnancyELCSAwake fibreoptic intubation GANoNo7NIV 17 h per dayIncrease of NIV use to 24 h per day at 18 weeksELCSGANoNo8Night NIV + cough assist—low adherence2nd trimester—gastroenteritis complicated by catheter-associated UTIUsed once at 23 weeks used overnight for two weeksELCSAwake fibreoptic intubation GANoNoNIV non-invasive ventilation, PRN as required, GA general anaesthetic, LRTI lower respiratory tract infection, UTI urinary tract infection, C/S caesarean section, ELCS elective lower segment caesarean section, PET preeclampsia toxaemia, GDM gestational diabetes mellitus, PPH postpartum haemorrhageTable 3Maternal outcomes (Postnatal and Mortality)PregnancyRespiratory support post-pregnancyProgress since deliveryLong-term follow-upMortality1NoneStable—working full-timeStable. Commenced Risdiplam 14 years post partum (for last 4 years)No2Night NIV 10–11 h, cough assist PRNNow has SPC due to urinary retention secondary to RisdiplamCommenced Risdiplam 5 years post-delivery due to increased weaknessNo3Extubated to NIV for 48 h, cough-assist device—CPAP trial, but did not use postnatallyC/S wound infection, sepsis with postnatal collection, laparotomy and bowel injury, 2 postnatal chest infections, perforated appendix 4 months postnatalReturned to pre-pregnancy stateNo4NIV immediately after C/S but stopped 4 h post-op. cough assist device daily for 2 weeks postnatalGradual postnatal increase in weakness. 1 year PN—returned to work, but was struggling with fatigue. Commenced NIV 7–8 h at night for 6 months. Next 6 months only when ill. Sleep study improved at 2-year postnatal review, stopped regular NIVStableNo5NoneDecided for second pregnancy 3 years laterRisdiplam for last 2 years,No6Continuous NIV for first 48 h postpartum, then back to intermittent use as requiredDecided for second pregnancy 7 years laterReturned to pre-pregnancy stateNo7Decrease of NIV use to 20–21 h per day. Weaned back to pre-pregnancy level 1 month postnatalNo changes in NIV use postpartum. NIV setting increased but usage time stayed the sameStableNo8Continuous NIV for 6 hUTI requiring admission 2 months postnatallyReturned to pre-pregnancy stateNoNIV non-invasive ventilation, CPAP continuous positive airway pressure, C/S caesarean section, UTI urinary tract infection, SPC suprapubic catheter
Neonatal outcomes
Six of the eight babies were born pre-term. Mean birth weight was 2540 g ± 658 g. Four required admission to the neonatal intensive care unit (NICU), three with respiratory distress, and one was admitted with necrotising enterocolitis. All NICU admissions were of babies born pre-term. There were two neonatal readmissions. No babies died and we have confirmed all are still alive and thriving at the time of writing. There were no reported congenital abnormalities. Table 4 summarises the neonatal outcomes. Table 4. Neonatal outcomesPregnancyAntenatal steroidsBirth weight (grams)Gestational age (weeks + days)Apgar score (1/5/10 min)Congenital anomaliesRespiratory distress syndromeNeonatal intensive care unit (NICU) admissionNeonatal readmission?Neonatal mortality1No340138 + 4Not availableNoneRequired inflation breaths immediately after birth—recovered spontaneouslyNoNoNo2Yes294036 + 44,6,10NonenoYes—2 daysNoNo3Yes323237 + 12, 4NonenoNoNo4Yes258036 + 2Not availableNoneNoneNOApnoeas day 10 secondary to reflux—resolved with antacidNo5Yes258035 + 02, 4NoneYesThree week admission—with RDSNoNo6219035 + 06, 6NoneNonoNoNo7No147430 + 04,5NoneYesAdmitted for three months with NEC1 week post discharge developed bronchiolitisNo8Yes192034 + 44,5NoneYes (TTN) 2 × sets of inflation breaths, 1 × ventilation breaths givenYes—5 daysNoNoNICU* neonatal intensive care unit, NEC necrotising enterocolitis, BW birth weight, RDS respiratory distress syndrome, TTN transient tachypnoea of the neonate
Discussion
For women living with SMA, embarking on a pregnancy may expose them to a significant risk of deterioration in their health [5], and presents unique challenges to medical teams managing them. Caring for these women is complex, and should be led by a highly skilled multi-speciality team with experience of pregnancy in women with SMA.
SMA type
This current series provides detailed insight into the management of pregnancy in women with SMA. Whilst age at delivery in our series is similar to previous reports [3, 4, 6] at 28 years, our population differs from previous reports in terms of SMA type. Specifically, to our knowledge, this series includes the first reported case of a successful pregnancy in a woman with SMA type-1. Furthermore, SMA type-2 is more prevalent, whereas in previous series, SMA type 3 was more prevalent [2]. It needs to be acknowledged that previously women with the more severe phenotype of type-1 and type-2 may have been counselled against pregnancy. As nutritional and respiratory support care has advanced, more of these higher risk women have been successfully supported through pregnancy.
Pre-pregnancy counselling
To date, PPC has not been described in the literature for women with SMA. Here we have reported that all but two of our patients received PPC. Of the two that did not, one had an unplanned pregnancy and one only had pre-pregnancy genetic counselling. PPC is well evidenced to be beneficial for women of child-bearing age with other chronic diseases [7, 8], and leads to better maternal and fetal outcomes. PPC should be offered to all women living with SMA as it allows for shared decision making regarding reproductive choices and highly personalised care and advice supporting each woman to prepare for the challenges of pregnancy.
Monitoring respiratory function
Respiratory muscle function, depending on disease severity, can be preserved but one must be aware that women living with SMA can have chronic respiratory failure, requiring nocturnal NIV to support inspiratory muscle function, and cough assist device to support expiratory muscle function and secretion management [2, 9, 10]. In addition, the restrictive ventilatory defect imposed by respiratory muscle weakness will worsen as pregnancy progresses. The diaphragm becomes increasingly splinted as a consequence of the increasing intra-abdominal pressure of the gravid uterus. Indeed, half of the pregnancies in our case series required an increase in respiratory support mid second trimester until after the baby was delivered. Interestingly, this is in contrast to the observations in the Bencivenga et al. series [11], where they reported no change in respiratory function throughout pregnancy. This highlights the much higher risk patients in our series.
In pregnant people with such severe neuromuscular disease, monitoring and surveillance of daytime symptom burden and overnight respiratory status is essential. In line with the low incidence of such pregnant patients, there are no validated respiratory or sleep questionnaires. Standard simple physiological monitoring with spirometry has limited clinical value as often these patients have a significantly reduced vital capacity (VC) due to respiratory muscle weakness and the associated restrictive ventilatory defect, for example VC of less than 1L. This, in essence, means that tracking VC lacks both sensitivity or specificity to have clinical value.
During the 1st and 2nd trimester, we undertook monthly reviews, assessing respiratory and sleep symptoms (e.g. positional breathlessness, breathlessness on hoist transfer, sleep quality, early morning headaches and daytime fatigue) with dual channel overnight oximetry studies to evaluate upper airways obstruction as well as hypoventilation accompanied by daytime spot transcutaneous carbon dioxide and oxygen assessment. During the third trimester, more frequent multi-professional clinical reviews, assessing respiratory and sleep symptoms, took place. These included daytime spot transcutaneous carbon dioxide, as an elevated carbon dioxide level is a warning signal that would necessitate an increase in either the pressure support and/or back up rate in the ventilator. We aimed to maintain carbon dioxide levels within the normal range, or even low normal range, throughout pregnancy. This clinical approach is required to maintain lung volumes, ventilation and gas exchange as pregnancy progresses and intra-abdominal pressure rises and offset the impaired respiratory muscle and diaphragm function.
Mode of maternal delivery
All women in the current series underwent elective lower segment caesarean section (ELCS) and this should be planned for. This is similar to the findings by Bencivenga et al. [11]. Women with SMA often have significant contractures and positioning them on an operating theatre table is more difficult. We use a combination of gel pads and bean bags to safely support the limbs and the usual lateral supports to ensure a safe left lateral position. In some cases, access to the lower abdomen for a transverse suprapubic incision is complicated and the usual surgical stance to perform the surgery needs to be reconsidered. The surgery itself needs to be gentle with sharp dissection abdominal entry, without the typical stretching of the abdominal wall incision routinely practiced by many obstetricians, to avoid extension of the incision due to tissue fragility. Future contraceptive issues, including tubal ligation, will have been discussed preoperatively, as well as menstrual issues that could be addressed by insertion of a progestogen-releasing intrauterine system at the time of surgery.
Closure of the rectus sheath with a suitable suture is important. The rectus sheath is usually thin and fragile and use of a non-absorbable nylon suture or long term absorbable PDS (Polydioxanone) suture is required. There is usually very little fat, but a 2-layer fat closure with 2/0 monocryl (poliglecaprone 25) is preferred. Skin closure is with subcuticular monocryl and with dermabond (2-Octyl cyanoacrylate) skin adhesive for additional support, which also acts as a dressing. Standard antibiotic prophylaxis is used to prevent infection as are routine uterotonics to prevent uterine atony and post-partum bleeding.
Mode of anaesthesia
Regional anaesthesia, in the form of intrathecal local anaesthetic and opioid injected in the lumbar region below the termination of the spinal cord, is the preferred mode of anaesthesia for caesarean section in the obstetric population.
This technique may be difficult in the presence of scoliosis, if bony landmarks are distorted, and in the presence of lumbar metal rod fixation, where needle access to the lumbar neuraxium may not be possible.
SMA types 1 and 2 lead to scoliosis due to the inability of weak spinal muscles to support growing spinal bones. In our case series all patients had severe scoliosis and five had required extensive spinal metal rod fixation involving the lumbar spine (Fig. 1). Our patient with SMA Type-1 had not had spinal fixation but had severe kyphoscoliosis (Fig. 2).Fig. 1. Lumbar spine x-ray images of five of the patients who had spinal fixation prior to pregnancyFig. 2Lumbar spine x-ray image of patient with SMA Type-1 who has severe kyphoscoliosis
In our case series of severely affected individuals, 100% required general anaesthesia, which contrasts with Bencivenga’s case series [11] in which 80% received regional anaesthesia and 20% general anaesthesia.
One patient consented to an attempt at administering spinal anaesthesia, but unfortunately, this was unsuccessful and a general anaesthetic was given; in her second pregnancy this patient chose not to re-attempt regional anaesthesia.
All patients in our series had required general anaesthesia for other treatments prior to delivery, and as a result, three patients in our series were known to be difficult to intubate; these three patients received awake fibre-optic intubation using infusions of Remifentanil and Propofol to maintain anaesthesia. Where neuromuscular blockade was required, Rocuronium was used, with the reversal agent Sugammadex administered at the end of surgery to ensure full recovery of respiratory muscle function.
All patients received multimodal analgesia including an initial period of intravenous opioid analgesia in a nurse- or patient-controlled delivery device depending on their strength and ability to press the demand button.
Post-delivery care
As demonstrated in the current series, the multi-speciality team must be wholly knowledgeable of the potential for (a) extended anaesthetic recovery with muscle weakness e.g. neuromuscular blocking agents, (b) respiratory complications e.g. post-operative respiratory failure, impaired secretion clearance and respiratory infection, and (c) impact of post-operative analgesia e.g. respiratory depression from opiates [12]. The monitoring and management of these women in the intensive care unit or high dependency unit, during the post-operative stage, with judicious use of NIV with respiratory therapist-led use of cough assist devices for secretion clearance, reduces the risk of severe post-operative respiratory complications.
Enhanced post-partum care is essential. Skeletal muscle weakness will impact on the speed of recovery as well as caring for and bonding with the new infant. Therefore, early, regular postnatal multidisciplinary reviews should ensure adequate support is available, and aim to minimise the consequences of a potentially prolonged in-patient stay while the mother recovers from the delivery.
Maternal outcomes
In this case series, all women and their babies survived to time of writing, but seven of the eight pregnancies experienced complications. Women living with SMA can have a spectrum of impairment, the most common being issues with mobility and respiratory function. Indeed, all six women were wheelchair-dependent pre-pregnancy, suggesting that our cohort encompasses women with more severe type 2 SMA disease. In previous series, a significant number were independently mobile pre-pregnancy as these were predominantly SMA type 3 patients. Two in three of the women in the Bencivenga et al. series were ambulant pre-pregnancy [11]. However, Abati et al.’s systematic review reported that at least one in three women experienced persistent worsening of motor symptoms antenatally [4], and not all recovered mobility to pre-pregnancy levels postnatally.
Neonatal outcomes
In our series, 4 (50%) babies were admitted to the NICU within one week of birth, all for reasons related to prematurity, and 3 had documented RDS. In all cases, their premature delivery was a consequence of third-trimester deterioration in maternal health due to a more severe pre-pregnancy disease state. By contrast, in Abati et al.’s systematic review, the majority of babies were born healthy. Gestation at delivery was not well documented in all studies, but the largest case series reported an average gestational age of 36 weeks and one day [13], which broadly corresponds with the gestational age at birth in our series (35 weeks and five days). Overall, between 3–15% of babies were born with complications in Abati et al.’s review, the majority being related to prematurity and requiring brief admission to NICU. This again is possibly due to the fact that, in the past, women with more severe disease were less likely to get pregnant. Newborn screening for SMA was not offered to any patients in our series.
Strengths and limitations
Our case series adds significantly to the literature describing outcomes of pregnancies in women with SMA. It provides an up-to-date report and reflects the improved care for women living with more severe phenotypes of SMA who embark on a pregnancy. Although there are expected potential complications in these women and their babies, these can be managed effectively. Furthermore, this current series provides detailed clinical information on the complications and outcomes which can be discussed during pre-pregnancy counselling.
Limitations in our series include a paucity of precise detail in the degree of deterioration in spirometry in the women who decompensated, although this has limited value when patients are already established on nocturnal NIV. Several of our women had shared care between their local hospital and our tertiary specialist maternity centre, therefore not all complications during pregnancy may have been captured accurately in our records.
None of the women in our case series fell pregnant while using disease-modifying treatments (DMTs) for SMA (such as Nusinersen, Risdiplam, or Onasemnogene Abeparvovec). This is because most of the pregnancies in our series concluded before their widespread availability. We are therefore unable to comment on the management of DMTs during pregnancy, other than to point out that their use during pregnancy—and impact on fetus—is currently the subject of on-going research.
Conclusion
Guidance on managing pregnancy in women with SMA is limited. As with previous case series, our findings are supportive of pregnancy in women with SMA, with regular reviews and monitoring by an experienced multi-speciality team. In the era of disease modifying treatments, we would further recommend a Neurologist be a member of the MDT to help guide their management around pregnancy. Our series also demonstrates that women with a more severe phenotype of SMA can be successfully supported through pregnancy. Indeed, women living with SMA should not be discouraged from becoming pregnant. While pregnancy is likely to be more complicated than for healthy women, with appropriate counselling and clinical support, the overwhelming evidence is that both mother and baby will have good outcomes.