Clinical outcomes of endovascular treatment for acute basilar artery occlusion patients with extremely severe symptoms
Yongtao Guo, Yuqian Xie, Miao Chai, Linyu Li, Shuangzhi Wang, Sheng Zhou, Haoxuan Zhu, Gaoming Li, Lilan Wang, Chunye Chen, Mingyang Chen, Yuhan Fan, Qiuyi Yang, Yihui Yang, Yian Chen, Binghan Wang, Guanting Heng, Xuexiao Zhao, Chawen Ding, Jiaxing Song, Jie Tang, Zhenqian Liu

TL;DR
This study shows that endovascular treatment improves outcomes for patients with severe basilar artery strokes compared to standard care.
Contribution
The study provides real-world evidence on the effectiveness and safety of EVT in patients with extremely severe basilar artery occlusion.
Findings
EVT was associated with better functional outcomes and lower mortality compared to standard medical treatment.
Shorter treatment times improved outcomes, while higher stroke severity reduced the benefits of EVT.
Symptomatic intracerebral hemorrhage rates were similar between the two treatment groups after matching.
Abstract
This study aimed to investigate the effectiveness and safety of endovascular treatment (EVT) in acute basilar artery occlusion (ABAO) patients with extremely severe symptoms [National Institutes of Health Stroke Scale (NIHSS) score >25] in the real world. This study was a subgroup analysis of a prospective multicenter cohort study (EVT for Acute Basilar Artery Occlusion Study, BASILAR registry). Patients were categorized into EVT and standard medical treatment (SMT) groups. The primary effectiveness outcome was the distribution of modified Rankin Scale (mRS) scores at 90 days. Safety outcomes included 90-day mortality and symptomatic intracerebral hemorrhage (sICH) within 48 h. Among 436 ABAO patients with extremely severe symptoms, 342 (78.4%) underwent EVT. Compared with SMT, EVT was significantly associated with greater odds of favorable shift in mRS distribution [adjusted OR (aOR)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
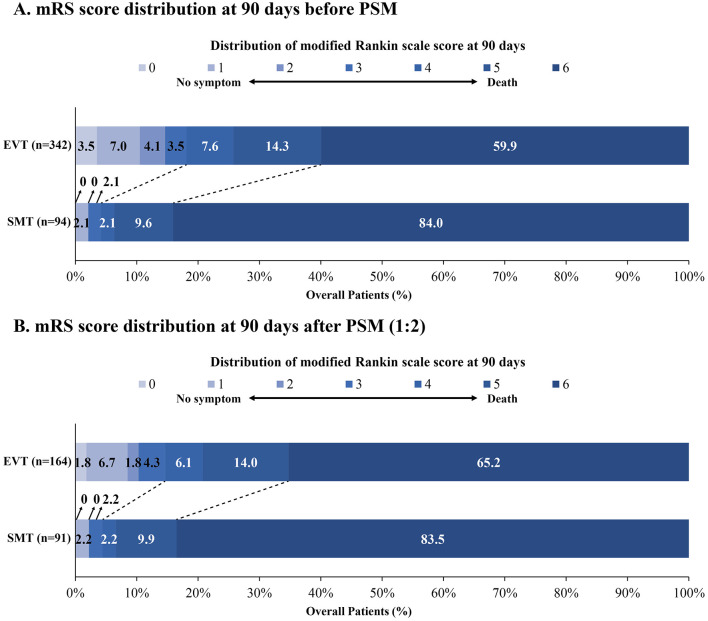 Figure 1
Figure 1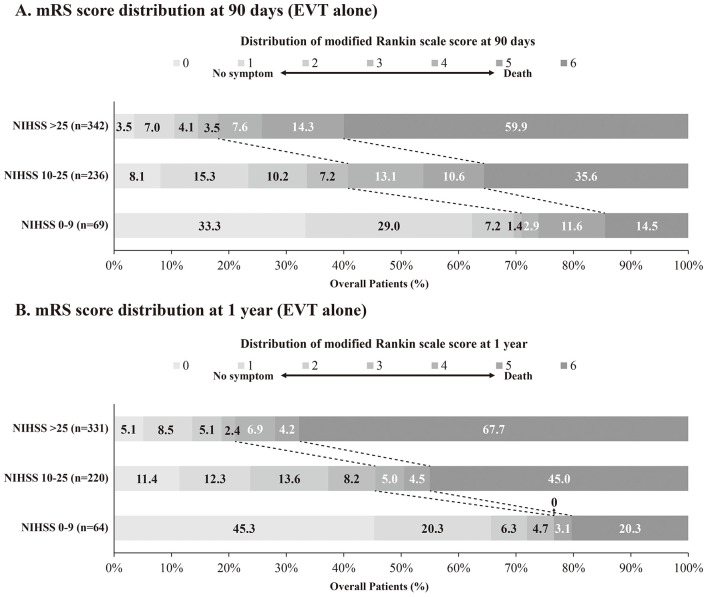 Figure 2
Figure 2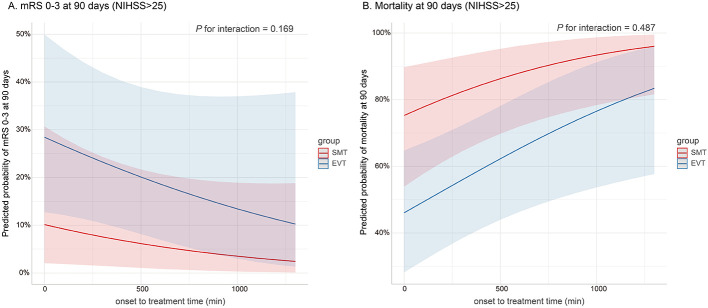 Figure 3
Figure 3|
|
|
| ||||||
|---|---|---|---|---|---|---|---|---|
|
|
| |||||||
| Age, | 65 (57–74) | 68 (59–76) | 65 (57–74) | 0.126 | 66 (59–74) | 66 (59–75) | 66 (58–74) | 0.730 |
| Sex, male, | 317 (72.7) | 64 (68.1) | 253 (74.0) | 0.256 | 172 (67.5) | 62 (68.1) | 110 (67.1) | 0.863 |
| Hypertension | 303 (69.5) | 65 (69.1) | 238 (69.6) | 0.934 | 184 (72.2) | 64 (70.3) | 120 (73.2) | 0.628 |
| Diabetes mellitus | 99 (22.7) | 20 (21.3) | 79 (23.1) | 0.709 | 54 (21.2) | 19 (20.9) | 35 (21.3) | 0.931 |
| Hyperlipidemia | 134 (30.7) | 30 (31.9) | 104 (30.4) | 0.779 | 79 (31.0) | 30 (33.0) | 49 (29.9) | 0.609 |
| Smoking | 136 (31.2) | 14 (14.9) | 122 (35.7) | <0.001 | 41 (16.1) | 14 (15.4) | 27 (16.5) | 0.822 |
| Ischemic stroke | 102 (23.4) | 25 (26.6) | 77 (22.5) | 0.408 | 57 (22.4) | 23 (25.3) | 34 (20.7) | 0.404 |
| AF | 103 (23.6) | 15 (16.0) | 88 (25.7) | 0.048 | 58 (22.7) | 15 (16.5) | 43 (26.2) | 0.076 |
| CHD | 81 (18.6) | 12 (12.8) | 69 (20.2) | 0.102 | 37 (14.5) | 12 (13.2) | 25 (15.2) | 0.655 |
| Prodromal transient ischemic stroke or minor stroke | 194 (44.5) | 45 (47.9) | 149 (43.6) | 0.457 | 116 (45.5) | 45 (49.5) | 71 (43.3) | 0.344 |
| SBP, mmHg, median (IQR)a | 151 (135–168) | 160 (145–172) | 150 (132–166) | <0.001 | 156 (140–171) | 160 (144–172) | 154 (140–170) | 0.319 |
| Baseline NIHSS score, median (IQR) | 33 (30–35) | 32 (30–35) | 33 (30–35) | 0.504 | 32 (30–35) | 32 (30–35) | 33 (30–35) | 0.807 |
| Baseline pc-ASPECTS, median (IQR)b | 8 (6–9) | 7 (6–8) | 8 (6–9) | 0.003 | 7 (6–8) | 7 (6–8) | 7 (6–8) | 0.969 |
| 0–1 | 332 (76.1) | 72 (76.6) | 260 (76.0) | 0.170 | 199 (78.0) | 69 (75.8) | 130 (79.3) | 0.131 |
| 2 | 82 (18.8) | 14 (14.9) | 68 (19.9) | 43 (16.9) | 14 (15.4) | 29 (17.7) | ||
| 3–4 | 22 (5.0) | 8 (8.5) | 14 (4.1) | 13 (5.1) | 8 (8.8) | 5 (3.0) | ||
|
| ||||||||
| 0 | 369 (84.6) | 81 (86.2) | 288 (84.2) | 0.757 | 223 (87.5) | 79 (86.8) | 144 (87.8) | 0.958 |
| 1 | 41 (9.4) | 7 (7.4) | 34 (9.9) | 18 (7.1) | 7 (7.7) | 11 (6.7) | ||
| 2 | 26 (6.0) | 6 (6.4) | 20 (5.8) | 14 (5.5) | 5 (5.5) | 9 (5.5) | ||
| LAA | 261 (59.9) | 55 (58.5) | 206 (60.2) | 0.003 | 146 (57.3) | 54 (59.3) | 92 (56.1) | 0.063 |
| CE | 123 (28.2) | 19 (20.2) | 104 (30.4) | 72 (28.2) | 19 (20.9) | 53 (32.3) | ||
| Others | 52 (11.9) | 20 (21.3) | 32 (9.4) | 37 (14.5) | 18 (19.8) | 19 (11.6) | ||
| Distal basilar artery | 162 (37.2) | 31 (33.0) | 131 (38.3) | 0.002 | 100 (39.2) | 29 (31.9) | 71 (43.3) | 0.002 |
| Middle basilar artery | 142 (32.6) | 45 (47.9) | 97 (28.4) | 88 (34.5) | 45 (49.5) | 43 (26.2) | ||
| Proximal basilar artery | 56 (12.8) | 6 (6.4) | 50 (14.6) | 28 (11.0) | 6 (6.6) | 22 (13.4) | ||
| Vertebral artery-V4 segment | 76 (17.4) | 12 (12.8) | 64 (18.7) | 39 (15.3) | 11 (12.1) | 28 (17.1) | ||
| IVT, | 98 (22.5) | 32 (34.0) | 66 (19.3) | 0.002 | 80 (31.4) | 30 (33.0) | 50 (30.5) | 0.683 |
| Onset to imaging time, min, median (IQR) | 210 (100–354) | 199 (94–370) | 214 (102–352) | 0.900 | 219 (100–356) | 195 (94–360) | 220 (100–356) | 0.762 |
| Onset to treatment time, min, median (IQR) | 247 (140–394) | 240 (134–408) | 248 (141–394) | 0.982 | 247 (135–394) | 236 (132–394) | 251 (142–400) | 0.738 |
| Onset to puncture time, min, median (IQR) | NA | NA | 320 (220–487) | NA | NA | NA | 333 (229–495) | NA |
| Puncture to reperfusion time, min, median (IQR) | NA | NA | 102 (70–142) | NA | NA | NA | 101 (76–150) | NA |
| General anesthesia, | NA | NA | 152 (45.0) | NA | NA | NA | 92 (57.1) | NA |
| mTICI score of 2b-3 at final angiogram, | 274 (62.8) | 7 (7.4) | 267 (78.1) | <0.001 | 136 (53.3) | 7 (7.7) | 129 (78.7) | <0.001 |
|
|
|
| ||||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|
| |||||
| mRS score at 90dc, median (IQR) | 6 (6–6) | 6 (4–6) | 3.98 (2.02–7.84) | <0.001 | 6 (6–6) | 6 (5–6) | 3.53 (1.73–7.20) | <0.001 |
| mRS 0–3 at 90dd | 4 (4.3) | 62 (18.1) | 4.18 (1.28–13.67) | 0.018 | 4 (4.4) | 24 (14.6) | 4.41 (1.27–15.29) | 0.019 |
| mRS 0–2 at 90dd | 2 (2.1) | 50 (14.6) | 6.58 (1.39–31.22) | 0.018 | 2 (2.2) | 17 (10.4) | 7.24 (1.39–37.80) | 0.019 |
| mRS 0–1 at 90dd | 2 (2.1) | 36 (10.5) | 4.36 (0.90–21.13) | 0.067 | 2 (2.2) | 14 (8.5) | 5.50 (1.01–29.85) | 0.048 |
| Mortality at 90dd | 79 (84.0) | 205 (59.9) | 0.26 (0.13–0.53) | <0.001 | 76 (83.5) | 107 (65.2) | 0.30 (0.14–0.64) | 0.002 |
| sICH within 48ha, d | 1 (1.1) | 35 (10.5) | 8.80 (1.14–67.70) | 0.037 | 1 (1.1) | 13 (8.1) | 8.09 (0.97–67.23) | 0.053 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Retinal and Optic Conditions · Cerebrovascular and Carotid Artery Diseases
Introduction
Despite accounting for only 1% of all ischemic strokes and 5–10% of large vessel occlusions (LVO), acute basilar artery occlusion (ABAO) is associated with exceptionally high rates of disability and mortality (1, 2). The advent of endovascular treatment (EVT) has provided a promising therapeutic approach for patients with ABAO. Four landmark randomized controlled trials (RCTs) evaluated the efficacy and safety of EVT compared with standard medical treatment (SMT) in patients with ABAO. Although the BASICS (3) and BEST (4) trials failed to demonstrate the superiority of EVT over SMT, these pivotal studies laid the foundation for subsequent research. More recently, the ATTENTION (5) and BAOCHE (6) trials have demonstrated compelling evidence supporting the clinical efficacy of EVT in ABAO patients. Consistent with these findings, our prospective cohort study [Endovascular Treatment for Acute Basilar Artery Occlusion Study (BASILAR)] (7) revealed that EVT was significantly associated with improved functional outcomes and decreased mortality in patients with ABAO.
Previous studies found that EVT seemed to be safer and more effective for ABAO patients with mild to moderate symptoms compared to those with more severe symptoms (8, 9). These findings suggest that clinical severity at admission is associated with functional outcomes after EVT. Notably, while a prior study indicated that EVT was associated with improved functional outcomes even in ABAO patients with severe symptoms [National Institutes of Health Stroke Scale (NIHSS) score > 20] (10), dedicated studies investigating the effectiveness of EVT in ABAO patients with extremely severe symptoms (NIHSS score > 25) remain limited. This patient population is frequently excluded from clinical trials or analyzed only as subgroups. Consequently, whether EVT confers clinical benefit in ABAO patients with extremely severe symptoms remains unknown.
Therefore, this study aimed to investigate the effectiveness and safety of EVT in ABAO patients with extremely severe symptoms in the real world.
Methods
Study design and participants
The data analyzed in this study were obtained from the BASILAR registry (7). The BASILAR registry was a prospective multicenter cohort study that enrolled patients with ABAO from 47 stroke centers across China between January 2014 and May 2019. This study followed the ethical principles of the Helsinki Declaration and was approved by the ethics committees of all participating centers. All patients or their legal representatives provided written informed consent before enrollment. The inclusion criteria of enrolled centers have been published in the BASILAR main study.
The inclusion criteria for this study were as follows: (1) age ≥ 18 years; (2) ABAO confirmed by computed tomographic angiography (CTA), magnetic resonance angiography (MRA), or digital subtraction angiography (DSA); (3) time from symptom onset or last known well within 24 h; (4) ability to provide informed consent. The exclusion criteria were: (1) pre-stroke modified Rankin scale (mRS) score > 2; (2) neuroimaging evidence of intracranial hemorrhage on initial presentation; (3) absence of 90-day follow-up data; (4) current pregnancy or lactation; (5) severe, advanced or terminal illnesses.
Data collection
The following data were collected for all patients: demographics characteristics, medical history, prodromal symptoms, systolic blood pressure (SBP), stroke severity at admission, pre-stroke modified Rankin Scale score (mRS) score, neuroimaging findings, stroke etiology, intravenous thrombolysis (IVT) administration, workflow (time from symptom onset to imaging and treatment), EVT characteristics, anesthesia type, reperfusion status, and functional outcomes at 90 days and 1 year. Stroke severity of ABAO was dichotomized into extremely severe symptoms (i.e., NIHSS score > 25), moderate to severe symptoms (ie, NIHSS score 10–25) and mild to moderate symptoms (i.e., NIHSS score <10) groups using baseline NIHSS score from the BASILAR study. Stroke etiology was classified according to the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification system. Collateral circulation was evaluated using the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) grading system, with collateral status categorized as poor (grades 0–1), moderate (grade 2), or good (grades 3–4). The extent of ischemic injury was assessed using the posterior circulation-Alberta Stroke Program Early Computed Tomography Score (pc-ASPECTS). Reperfusion status was evaluated on the final angiogram using the modified Treatment in Cerebral Ischemia (mTICI) score, with successful reperfusion defined as mTICI 2b-3.
Outcomes
The primary effectiveness outcome was the distribution of mRS scores at 90 days (ranging from 0 [no symptoms] to 6 [death]). Secondary effectiveness outcomes included the proportion of patients achieving mRS 0–3, mRS 0–2, and mRS 0–1 at 90 days. Safety outcomes included 90-day mortality and symptomatic intracerebral hemorrhage (sICH) within 48 h confirmed by computed tomography (CT) or magnetic resonance imaging (MRI). sICH was defined according to the Heidelberg Bleeding Classification (11).
Statistical analysis
Normality of continuous variables was assessed using the Kolmogorov-Smirnov test. Normally distributed continuous variables were presented as mean ± standard deviation (SD), while non-normally distributed variables were presented as median [interquartile range (IQR)]. Categorical variables were expressed as frequencies and percentages. Between-group comparisons were performed using Student's t-test for normally distributed continuous variables or Mann–Whitney U test for non-normally distributed variables. Categorical variables were compared using the chi-square test or Fisher's exact test when appropriate.
Logistic regression analyses were performed to assess the association between EVT and clinical outcomes. The shift in mRS score distribution was analyzed using ordinal logistic regression. Binary logistic regression was performed for dichotomous outcomes including mRS 0–3, mRS 0–2, mRS 0–1, sICH, and mortality. Results were reported as odds ratios (OR) with 95% confidence intervals (CIs). Multivariable regression analyses were performed adjusting for covariates selected based on clinical relevance and baseline characteristics. For analyses of patients with extremely severe symptoms (NIHSS score > 25) and moderate to severe symptoms (NIHSS score 10–25), covariates included age, sex, systolic blood pressure (SBP), baseline NIHSS, baseline pc-ASPECTS, smoking history, ASITN/SIR grade, stroke etiology, occlusion site, and IVT. For analyses of patients receiving EVT, we adjusted for age, sex, baseline pc-ASPECTS, atrial fibrillation (AF), coronary heart disease (CHD), ASITN/SIR grade, stroke etiology, anesthesia type, and reperfusion status.
Two separate propensity score matching (PSM) analyses were conducted to minimize selection bias and balance baseline characteristics between treatment groups. For patients with extremely severe symptoms, propensity scores were estimated using multivariable logistic regression with age, SBP, smoking history, baseline pc-ASPECTS, occlusion site, and IVT as covariates. For patients with moderate to severe symptoms, propensity scores incorporated SBP, baseline NIHSS, baseline pc-ASPECTS, and occlusion site as covariates. For both analyses, 1:2 nearest neighbor matching algorithm without replacement was employed to compare outcomes between SMT and EVT groups. Matching was conducted using a caliper width of 0.2 standard deviations of the logit of the propensity score. Detailed information regarding both PSM analyses was provided in Methods S1 and S2, respectively.
Marginal effects plots were constructed to visualize the association between key variables (onset to treatment time and puncture to reperfusion time) and clinical outcomes (mRS 0–3 and mortality), adjusting for the same covariates used in the multivariable logistic regression models. Subgroup analyses were performed to assess the effects of EVT on mRS distribution in specific subgroups. Interaction terms between treatment groups and subgroup indicators were incorporated into the models to evaluate treatment effect heterogeneity across subgroups. Given the minimal missing data for key variables, no imputation methods were employed. A two-tailed P-value <0.05 was considered statistically significant. Statistical analyses were conducted using IBM SPSS Statistics version 27.0 (IBM Corp., Armonk, NY, USA) and R version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics of patients with extremely severe symptoms (NIHSS score > 25)
Among 829 patients with ABAO, 436 patients with extremely severe symptoms were included in the analysis (Figure S1). Of these, 342 (78.4%) underwent EVT. The median age was 65 (IQR, 57–74) years, and 317 (72.7%) patients were male. Compared with the SMT group, patients treated with EVT had higher proportions of AF (25.7% vs. 16.0%, P = 0.048) and smoking history (35.7% vs. 14.9%, P < 0.001), lower SBP (150 vs. 160 mmHg, P < 0.001), and higher baseline pc-ASPECTS (8 vs. 7, P = 0.003). EVT patients were less frequently to receive IVT (19.3% vs. 34.0%, P = 0.002). Additionally, significant differences were observed between groups in stroke etiology (P = 0.003) and occlusion sites (P = 0.002). No significant differences were observed in other baseline characteristics between treatment groups. Among EVT patients, the median onset to puncture time was 320 (IQR, 220–487) min, and the median puncture to reperfusion time was 102 (IQR, 70–142) min. General anesthesia was administered in 152 (45.0%) patients, and successful reperfusion was achieved in 267 (78.1%) patients. After PSM, baseline characteristics were well-balanced between the two groups. Other details were presented in Table 1.
Clinical outcomes of patients with extremely severe symptoms (NIHSS score > 25; SMT group vs. EVT group)
The median mRS score was 6 (IQR, 6-6) in the SMT group and 6 (IQR, 4–6) in the EVT group. Patients receiving EVT demonstrated significantly greater odds of favorable shift in mRS distribution compared to those receiving SMT [adjusted OR (aOR) 3.98, 95% CI 2.02–7.84, P < 0.001; Figure 1A and Table 2]. Compared with the SMT group, the EVT group showed significantly higher odds of achieving mRS 0–3 (aOR 4.18, 95% CI 1.28–13.67, P = 0.018) and mRS 0–2 (aOR 6.58, 95% CI 1.39–31.22, P = 0.018). The incidence of sICH within 48 hours was higher in the EVT group (aOR 8.80, 95% CI 1.14–67.70, P = 0.037). However, mortality was significantly lower in the EVT group than in the SMT group (aOR 0.26, 95% CI 0.13–0.53, P < 0.001). Following PSM, this difference in sICH was no longer statistically significant. Other results remained consistent before and after PSM (Figure 1B and Table 2). Long-term follow-up at 1 year demonstrated comparable clinical outcomes between the two groups (Figure S2 and Table S1). Additionally, we compared the effectiveness and safety of EVT vs. SMT among patients with NIHSS score of 10–25, with detailed results presented in Tables S2–S4.
Distribution of modified Rankin scale score at 90 days in ABAO patients with extremely severe symptoms (NIHSS score >25). The distributions of mRS scores at 90 days in ABAO patients with extremely severe symptoms are presented for the SMT and EVT groups before (A) and after (B) PSM. Abbreviations: ABAO, acute basilar artery occlusion; EVT, endovascular treatment; mRS, modified Rankin scale; PSM, propensity score matching; SMT, standard medical treatment.
Clinical outcomes of patients stratified by NIHSS score in EVT group (NIHSS score 0–9 vs. 10–25 vs. >25)
To evaluate the impact of baseline stroke severity on treatment outcomes, we stratified the 647 ABAO patients receiving EVT into three groups based on NIHSS scores: 0–9 (mild to moderate), 10–25 (moderate to severe), and >25 (extremely severe), and compared treatment effectiveness. Baseline characteristics of patients were shown in Table S5. Higher stroke severity was significantly associated with increased rates of AF (P = 0.008) and CHD (P = 0.014), lower baseline pc-ASPECTS (P < 0.001), and higher rates of general anesthesia (P < 0.001). Additionally, significant differences in ASITN/SIR grade distribution were observed across the three severity groups (P < 0.001). No significant differences were observed among the three groups for other baseline characteristics. Compared with the NIHSS 0–9 group, both NIHSS 10–25 (aOR 0.29, 95% CI 0.17–0.50, P < 0.001) and NIHSS > 25 (aOR 0.14, 95% CI 0.08–0.25, P < 0.001) were significantly associated with lower odds of achieving a favorable shift in mRS distribution (Figure 2A and Table S6). Similar trends were observed for outcomes of mRS 0–3, mRS 0–2, and mRS 0–1. Additionally, NIHSS 10–25 (aOR 2.42, 95% CI 1.06–5.49, P = 0.035) and NIHSS > 25 (aOR 5.16, 95% CI 2.30–11.61, P < 0.001) were significantly associated with higher odds of mortality compared with NIHSS 0–9. No significant differences in the odds of sICH within 48 h among the three severity groups. These findings persisted at 1-year follow-up, with similar long-term clinical outcomes observed between groups (Figure 2B and Table S7).
Distribution of modified Rankin Scale score at 90 days and 1 year in ABAO patients stratified by NIHSS score in EVT group (NIHSS score 0–9 vs. 10–25 vs. >25). The distributions of mRS scores at 90 days (A) and 1 year (B) in ABAO patients in EVT group are presented, stratified by NIHSS score. ABAO, acute basilar artery occlusion; EVT, endovascular treatment; mRS, modified Rankin scale; NIHSS, National Institutes of Health Stroke Scale; PSM, propensity score matching.
Marginal effects and clinical outcomes
The predicted probabilities of achieving mRS 0–3 and mortality among ABAO patients with extremely severe symptoms (NIHSS score > 25) were estimated based on onset to treatment time, as illustrated in Figure 3. The predicted probability of achieving mRS 0–3 progressively decreased with increasing onset to treatment time, while the predicted probability of mortality correspondingly increased. The EVT group consistently demonstrated a higher predicted probability of achieving mRS 0–3 and a lower predicted probability of mortality compared with the SMT group. However, no interaction was observed between the onset to treatment time and groups for either outcome (P for interaction = 0.169 and 0.487, respectively).
Association of onset to treatment time with the predicted probability of clinical outcomes in ABAO patients with extremely severe symptoms. The predicted probabilities of achieving mRS 0–3 and mortality by onset to treatment time among ABAO patients with extremely severe symptoms are presented in (A) and (B). The predicted probability of achieving mRS 0–3 progressively decreases with longer onset to treatment time, while the predicted probability of mortality correspondingly increases. Compared to the SMT group, the EVT group exhibits higher predicted probabilities of mRS 0–3 and lower predicted probabilities of mortality. However, no interaction was found between the onset to treatment time and groups for either outcome (P for interaction = 0.169 and 0.487, respectively). Solid lines indicate predicted probabilities of outcomes; shaded areas represent 95% CIs. ABAO, acute basilar artery occlusion; CI, confidence interval; EVT, endovascular treatment; mRS, modified Rankin scale; SMT, standard medical treatment.
The predicted probabilities of achieving mRS 0–3 and mortality among ABAO patients stratified by NIHSS score in the EVT group (NIHSS score 0–9 vs. 10–25 vs. >25) were estimated based on puncture to reperfusion time, as depicted in Figure S3. The predicted probability of achieving mRS 0–3 progressively decreased with longer puncture to reperfusion time, while the predicted probability of mortality correspondingly increased. Lower baseline stroke severity was associated with higher predicted probability of achieving mRS 0–3 and lower predicted probability of mortality. Additionally, no interaction was found between the puncture to reperfusion time and baseline stroke severity for either outcome (P for interaction = 0.322 and 0.869, respectively).
Subgroup analyses
Subgroup analyses were conducted to explore potential heterogeneity in EVT treatment effects on mRS distribution across different patient populations. No significant heterogeneity was observed across all subgroups stratified by age, sex, baseline NIHSS score, baseline pc-ASPECTS, AF, ASITN/SIR grade, stroke etiology, occlusion site, IVT administration, and onset to treatment time (Figure S4).
Discussion
This study investigated the effectiveness and safety of EVT in ABAO patients with extremely severe symptoms. Our findings demonstrated that EVT was significantly associated with improved functional outcomes in this patient population. Shorter onset to treatment time and puncture to reperfusion time were associated with higher predicted probabilities of achieving mRS 0–3 and lower predicted probabilities of mortality. Additionally, the benefit of EVT with longer onset-to-treatment intervals was negatively associated with increasing baseline stroke severity.
Patients with NIHSS score > 25 demonstrated a higher frequency of posterior circulation stroke and more commonly presented with impaired consciousness upon admission compared to patients with anterior stroke (12). The ATTENTION (5) and BAOCHE (6) trials provided compelling evidence for the efficacy and safety of EVT in patients with ABAO. Notably, these pivotal trials only analyzed patients with NIHSS score > 20 within subgroup analyses. A previous study demonstrated that EVT was safe and successful recanalization was strongly associated with better functional outcomes in patients with extremely severe anterior circulation ischemic stroke; however, the study lacked an SMT group for comparison (13). However, the real-world effectiveness and safety of EVT for ABAO patients with extremely severe symptoms remained unclear. Our findings demonstrated significant clinical benefits of EVT in ABAO patients with extremely severe symptoms at both short-term and long-term follow-up. These findings provide robust evidence to support clinical decision-making for EVT in this challenging patient population.
SICH is a serious complication after EVT for acute ischemic stroke, has been shown to be associated with poor functional prognosis and increased mortality (14, 15). The risk of sICH after IVT or EVT appears substantially lower in posterior circulation stroke patients compared to those with anterior circulation stroke (16, 17). Additionally, higher baseline NIHSS score has been identified as a predictor of sICH (18). In our cohort, although the EVT group had a significantly higher incidence of sICH compared with the SMT group among ABAO patients with extremely severe symptoms, the EVT group achieved superior clinical outcomes. Notably, we did not observe significant differences in sICH rates across varying baseline stroke severity groups among ABAO patients undergoing EVT. These observations suggest that EVT maintains an acceptable safety profile in this patient population.
The principle of “time is brain” emphasizes that treatment delays in acute ischemic stroke lead to irreversible neuronal loss of approximately 1.9 million neurons per minute (19). Previous studies have demonstrated that shorter onset to treatment time is significantly associated with better functional outcomes (20, 21). Consistent with previous findings, our results demonstrated that the predicted probability of achieving mRS 0–3 progressively declined with increasing onset to treatment time. These findings underscore the critical importance of reducing treatment delays to optimize functional outcomes in ABAO patients with extremely severe symptoms.
Shorter procedural time was associated with reduced risk of mortality and higher odds of favorable outcomes (22, 23). In patients with ABAO, the risk of complications and mortality increased by 0.5% and 1.5% with every 10-min increase in procedural time, respectively (23). Our findings also revealed that among ABAO patients treated with EVT, longer puncture to reperfusion time was associated with decreased predicted probability of achieving mRS 0–3 and increased predicted probability of mortality. Shortening EVT procedure time contributes to minimizing perioperative complications and reducing ischemic duration, thereby improving neurological outcomes (24). Therefore, maximizing technical proficiency and enhancing both the efficiency and quality of reperfusion are crucial for ABAO patients with extremely severe symptoms. Furthermore, when procedural time is significantly prolonged, clinicians should carefully assess the benefit-risk ratio of continuing the intervention to avoid futile or potentially harmful overtreatment.
Limitations
However, this study has several limitations. First, the observational study design inherently carries the risk of selection bias, and our findings require validation through RCTs. Second, as the enrolled population was Chinese, the generalizability of our results to other ethnic populations requires further investigation. Finally, our findings necessitate confirmation in larger-scale studies.
Conclusions
In ABAO patients with extremely severe symptoms, EVT was associated with superior functional outcomes and lower mortality compared to SMT alone. Minimizing onset to treatment time and puncture to reperfusion time is essential for optimizing clinical outcomes in this patient population. Additionally, the effectiveness and safety of EVT decreased progressively with increasing baseline stroke severity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mattle HP Arnold M Lindsberg PJ Schonewille WJ Schroth G. Basilar artery occlusion. Lancet Neurol. (2011) 10:1002–14. doi: 10.1016/S 1474-4422(11)70229-022014435 · doi ↗ · pubmed ↗
- 2Alemseged F Nguyen TN Alverne FM Liu X Schonewille WJ Nogueira RG. Endovascular therapy for basilar artery occlusion. Stroke. (2023) 54:1127–37. doi: 10.1161/STROKEAHA.122.04080736722343 · doi ↗ · pubmed ↗
- 3Langezaal LCM van der Hoeven E Mont'Alverne FJA de Carvalho JJF Lima FO Dippel DWJ . Endovascular therapy for stroke due to basilar-artery occlusion. New Engl J Med. (2021) 384:1910–20. doi: 10.1056/NEJ Moa 203029734010530 · doi ↗ · pubmed ↗
- 4Liu X Dai Q Ye R Zi W Liu Y Wang H . Endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion (best): an open-label, randomised controlled trial. Lancet Neurol. (2020) 19:115–22. doi: 10.1016/S 1474-4422(19)30395-331831388 · doi ↗ · pubmed ↗
- 5Tao C Nogueira RG Zhu Y Sun J Han H Yuan G . Trial of endovascular treatment of acute basilar-artery occlusion. New Engl J Med. (2022) 387:1361–72. doi: 10.1056/NEJ Moa 220631736239644 · doi ↗ · pubmed ↗
- 6Jovin TG Li C Wu L Wu C Chen J Jiang C . Trial of thrombectomy 6 to 24 hours after stroke due to basilar-artery occlusion. New Engl J Med. (2022) 387:1373–84. doi: 10.1056/NEJ Moa 220757636239645 · doi ↗ · pubmed ↗
- 7Zi W Qiu Z Wu D Li F Liu H Liu W . Assessment of endovascular treatment for acute basilar artery occlusion via a nationwide prospective registry. JAMA Neurol. (2020) 77:561–73. doi: 10.1001/jamaneurol.2020.015632080711 PMC 7042866 · doi ↗ · pubmed ↗
- 8Guenego A Dargazanli C Weisenburger-Lile D Gory B Richard S Ducroux C . Thrombectomy for basilar artery occlusion with mild symptoms. World Neurosurg. (2021) 149:e 400–14. doi: 10.1016/j.wneu.2021.02.01033578025 · doi ↗ · pubmed ↗