A real-world study on clinical features and prognosis of Chinese breast cancer patients with brain metastases
Hong-dan Chen, Xiao-wen Liao, Xiao-geng Chen, Yu-nan Su, Ding-long Pan, Guo-zhong Chen, Min Wu, Shuang-long Cai

TL;DR
This study examines the clinical features and survival outcomes of Chinese breast cancer patients who develop brain metastases.
Contribution
The study identifies distinct metastatic patterns and prognostic factors specific to breast cancer molecular subtypes in a real-world cohort.
Findings
Luminal subtype correlates with bone metastases, HER2-positive with liver metastases, and luminal with leptomeningeal metastases.
HER2-positive subtype and brain metastasis as first metastatic site are protective for survival, while leptomeningeal metastasis is a risk factor.
Most patients received radiotherapy, and 81.52% had died after a median follow-up of 63.1 months.
Abstract
This study aimed to analyze the clinical characteristics and prognosis of breast cancer (BC) patients with brain metastases (BM). We performed a retrospective analysis of breast cancer patients with brain metastases (BCBM) in a real-world setting. In a cohort of 249 breast cancer brain metastasis (BCBM) patients (all female; median age 46 years), molecular subtypes were distributed as follows: luminal (38.95%), HER2-positive (32.93%), and triple-negative (28.11%). Distinct metastatic patterns were observed: luminal subtype correlated with bone metastases (55.73%, p<0.001), HER2-positive with liver metastases (46.34%, p<0.001), and luminal with leptomeningeal metastases (19.59%, p=0.002). For CNS-directed treatment, 70.28% received radiotherapy (69.71% whole-brain radiotherapy, 30.28% stereotactic radiosurgery), while 23.69% received no local treatment. After median follow-up of 63.1…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
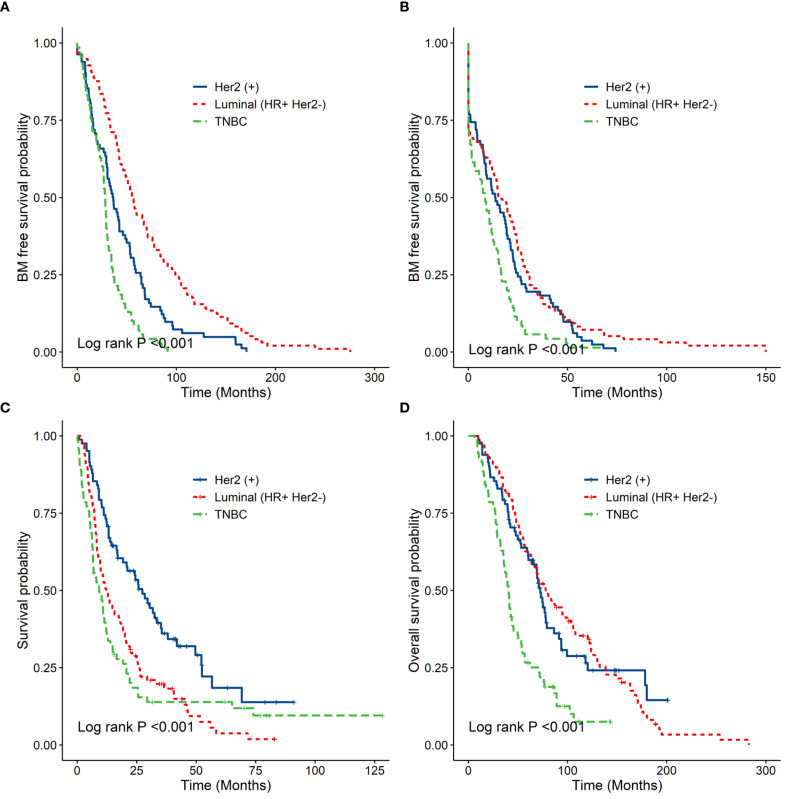 Figure 1
Figure 1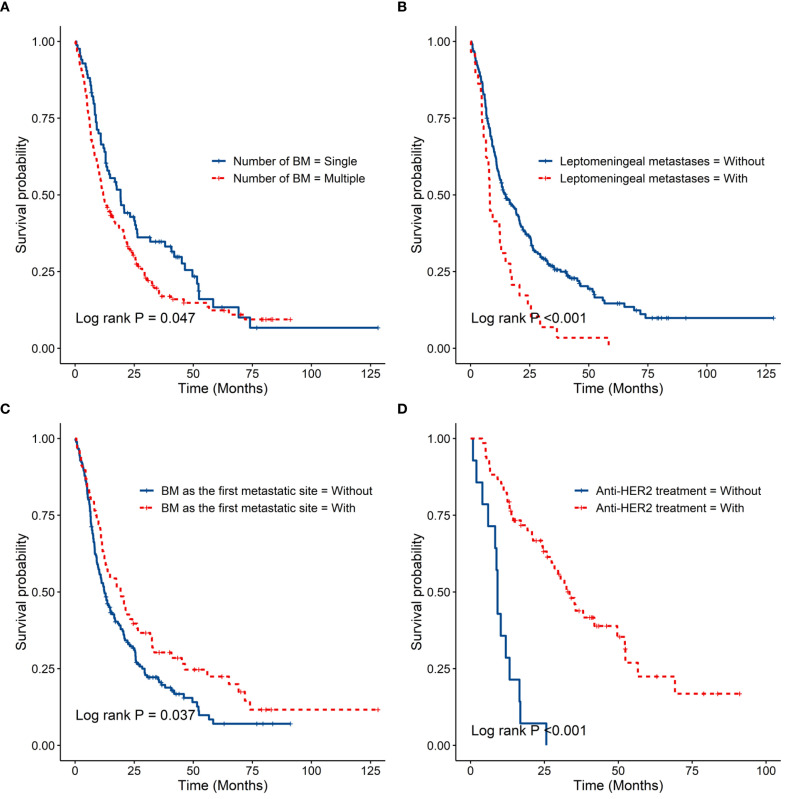 Figure 2
Figure 2| Variables | Total (n=249) | Molecular subtypes | P value | ||
|---|---|---|---|---|---|
| LUMINAL (n=97) | HER2 POSITIVE (n=82) | TNBC (n=70) | |||
| No.(%) | No.(%) | No.(%) | No.(%) | ||
| Age (years) | 46 | 46 | 46.5 | 47.5 | 0.674 |
| Median(range) | (23, 75) | (23, 66) | (23, 70) | (27, 75) | |
| Menopausal status at diagnosis | 0.875 | ||||
| Premenopausal | 166 (66.67%) | 66 | 55 (67.07%) | 45 (64.29%) | |
| Postmenopausal | 83 (33.33%) | 31 (31.96%) | 27 (32.93%) | 25 (35.71%) | |
| Family history | 0.944 | ||||
| No | 223 (89.56%) | 87 (89.69%) | 74 (90.24%) | 62 (88.57%) | |
| Yes | 26 (10.44%) | 10 (10.31%) | 8 (9.76%) | 8 (11.43%) | |
| Pathology type | 0.561 | ||||
| IDC | 212 (85.14%) | 84 (86.60%) | 69 (84.15%) | 59 (84.29%) | |
| IBC | 5 (2.01%) | 2 (2.06%) | 0 (0.00%) | 3 (4.29%) | |
| Mix | 26 (10.44%) | 8 (8.25%) | 11 (13.41%) | 7 (10.00%) | |
| Others | 6 (2.41%) | 3 (3.09%) | 2 (2.44%) | 1 (1.43%) | |
| TNM staging | 0.006 | ||||
| 0 | 3 (1.20%) | 0 (0.00%) | 0 (0.00%) | 3 (4.29%) | |
| I | 38 (15.26%) | 18 (18.56%) | 10 (12.20%) | 10 (14.29%) | |
| II | 73 (29.32%) | 28 (28.87%) | 16 (19.51%) | 29 (41.43%) | |
| III | 82 (32.93%) | 31 (31.96%) | 29 (35.37%) | 22 (31.43%) | |
| IV | 39 (15.66%) | 15 (15.46%) | 19 (23.17%) | 5 (7.14%) | |
| Missing | 14 (5.62%) | 5 (5.15%) | 8 (9.76%) | 1 (1.43%) | |
| First metastatic site | |||||
| Lung metastases | 0.337 | ||||
| No | 98 (39.36%) | 42 (43.30%) | 27 (32.93%) | 29 (41.43%) | |
| Yes | 151 (60.64%) | 55 (56.70%) | 55 (67.07%) | 41 (58.57%) | |
| Liver metastases | <0.001 | ||||
| No | 182 (73.09%) | 77 (79.38%) | 44 (53.66%) | 61 (87.14%) | |
| Yes | 67 (26.91%) | 20 (20.62%) | 38 (46.34%) | 9 (12.86%) | |
| Bone metastases | <0.001 | ||||
| No | 125 (50.20%) | 34 (35.05%) | 37 (45.12%) | 54 (77.14%) | |
| Yes | 124 (49.80%) | 63 (64.95%) | 45 (54.88%) | 16 (22.86%) | |
| Brain metastases | 0.224 | ||||
| No | 181 (72.69%) | 69 (71.13%) | 65 (79.27%) | 47 (67.14%) | |
| Yes | 68 (27.31%) | 28 (28.87%) | 17 (20.73%) | 23 (32.86%) | |
| Metastatic site in the chest wall or regional lymph nodes | 0.5 | ||||
| No | 83 (33.33%) | 29 (29.90%) | 27 (32.93%) | 27 (38.57%) | |
| Yes | 166 (66.67%) | 68 (70.10%) | 55 (67.07%) | 43 (61.43%) | |
| Number of brain metastasis | 0.693 | ||||
| Single | 84 (34.57%) | 31 (32.98%) | 31 (32.98%) | 26 (38.81%) | |
| Multiple | 159 (65.43%) | 63 (67.02%) | 55 (67.07%) | 41 (61.19%) | |
| Leptomeningeal metastases | 0.002 | ||||
| No | 220 (88.35%) | 78 (80.41%) | 80 (97.56%) | 62 (88.57%) | |
| Yes | 29 (11.65%) | 19 (19.59%) | 2 (2.44%) | 8 (11.43%) | |
| Local treatments for brain metastases | 0.084 | ||||
| RT only | 149 (59.84%) | 65 (67.01%) | 48 (58.54%) | 36 (51.43%) | |
| Surgery alone | 15 (6.02%) | 2 (2.06%) | 9 (10.98%) | 4 (5.71%) | |
| Surgery+RT | 26 (10.44%) | 8 (8.25%) | 10 (12.20%) | 8 (11.43%) | |
| No Local treatment | 59 (23.69%) | 22 (22.68%) | 15 (18.29%) | 22 (31.43%) | |
| Clinical progressions | Median time(months) | P value | ||||
|---|---|---|---|---|---|---|
| From | To | All patients (N=249) | Molecular subtypes | |||
| LUMINAL (n=97) | HER2 POSITIVE (n=82) | TNBC (n=70) | ||||
| BC | BM | 37 (32.9-42.5) | 56.6 (46.4-70.3) | 36.1 (30.5-46.1) | 28.2 (25.1-30.8) | <0.001 |
| FR | BM | 12.2 (9.33-15.3) | 16.67 (11.90-23.5) | 13.57 (8.80-19.3) | 8.42 (3.07-12.5) | <0.001 |
| BM | DOFU | 13.6 (11.6-18.1) | 12.2 (9.63-18.6) | 27.4 (19.23-35.5) | 9.2 (6.63-12.2) | <0.001 |
| BC | DOFU | 63.1 (54.6-72.4) | 77.9 (63.7-105.5) | 72.4 (60.5-86.3) | 40.5 (35.7-49.7) | <0.001 |
| Stratified variables | Median time(month) | P value | |
|---|---|---|---|
| Number of BM | Single (n=84) | 19.2 (13.2-26.2) | 0.047 |
| Multiple (n=159) | 11.9 (10.2-16.6) | ||
| Leptomeningeal metastases | With (n=29) | 8.13 (6.53-14.8) | <0.001 |
| Without (n=220) | 14.80 (12.23-20.4) | ||
| BM as the first metastatic site | With (n=68) | 19.3 (12.4-31.8) | 0.037 |
| Without (n=181) | 12.5 (10.2-16.6) | ||
| Anti-HER2 treatment | With (n=68) | 33.50 (27.40-52.2) | <0.001 |
| Without (n=11) | 9.13 (8.33-16.8) | ||
| Variables | Univariate analyses | Multivariate analyses | ||||
|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | |
| Age | ||||||
| ≤40 years | 1 | — | — | — | ||
| >40 years | 1.103 | 0.797-1.526 | 0.555 | — | — | — |
| Menopausal status at diagnosis | ||||||
| Premenopausal | 1 | — | — | — | ||
| Postmenopausal | 1.15 | 0.859-1.541 | 0.347 | — | — | — |
| Family history | ||||||
| No | 1 | — | — | — | ||
| Yes | 0.657 | 0.403-1.069 | 0.091 | — | — | — |
| Molecular Subtype | ||||||
| HR Positive Her2 Negative | 1 | 1 | ||||
| TNBC | 1.141 | 0.819-1.589 | 0.437 | 1.261 | 0.901-1.765 | 0.176 |
| Her2 Positive | 0.544 | 0.388-0.764 | <0.001 | 0.555 | 0.39-0.789 | 0.001 |
| Lung Metastasis as First Metastatic Site | ||||||
| No | 1 | — | — | — | ||
| Yes | 1.059 | 0.799-1.403 | 0.692 | — | — | — |
| Liver Metastasis as First Metastatic Site | ||||||
| No | 1 | — | — | — | ||
| Yes | 1.093 | 0.803-1.487 | 0.573 | — | — | — |
| Bone Metastasis as First Metastatic Site | ||||||
| No | 1 | — | — | — | ||
| Yes | 1.033 | 0.784-1.361 | 0.819 | — | — | — |
| Brain Metastasis as First Metastatic Site | ||||||
| No | 1 | 1 | ||||
| Yes | 0.717 | 0.524-0.981 | 0.038 | 0.649 | 0.47-0.897 | 0.009 |
| Chest Wall and Regional Lymph Nodes Metastasis as First Metastatic Site | ||||||
| No | 1 | — | — | — | ||
| Yes | 1.308 | 0.969-1.767 | 0.079 | — | — | — |
| Numbers of Brain Metastases | ||||||
| Single | 1 | 1 | ||||
| Multiple | 1.384 | 1.029-1.861 | 0.032 | 1.347 | 1-1.815 | 0.0501 |
| Leptomeningeal Metastases | ||||||
| No | 1 | 1 | ||||
| Yes | 1.961 | 1.319-2.916 | 0.001 | 1.653 | 1.098-2.488 | 0.016 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrain Metastases and Treatment · Lung Cancer Research Studies · Lung Cancer Treatments and Mutations
Introduction
1
Brain metastases (BM) represent one of the most significant causes of mortality in patients with malignant tumors. The incidence of brain metastasis in breast cancer patients ranks second among all malignant tumors, accounting for approximately 10% to 16% of all BM, surpassed only by lung cancer (1, 2). With recent advancements in brain imaging technology and systemic therapies, the incidence of BM is increasing. It has been reported that 5.1% of newly diagnosed breast cancer (BC) patients will develop BM within one year (3, 4), with the proportion increasing to 30% among metastatic BC patients (5). Since most antitumor drugs do not effectively cross the blood-brain barrier, patients with breast cancer brain metastases (BCBM) generally experience poor quality of life and an unfavorable prognosis (6, 7). Current data indicate that the median survival time for BCBM patients is less than six months, with a mortality rate of approximately 80% within one year (8). Furthermore, the prognosis for BCBM patients has not significantly improved over the past decades (9).
The incidence and survival rates of BM appear to vary across different BC subtypes (10, 11). Studies have shown that triple-negative breast cancer (TNBC) and HER2-positive BC patients are at a higher risk of developing BM compared to those with luminal-type BC (12, 13). TNBC exhibits the shortest median survival time when compared to luminal and HER2-positive types of BC (14). In this study, we aimed to analyze the clinical features and prognosis of BCBM patients in a real-world setting to provide valuable insights for the clinical diagnosis and treatment of BCBM.
Materials and methods
2
Patients
2.1
This retrospective analysis included 249 BCBM patients who were pathologically confirmed and treated at the Second Affiliated Hospital of Fujian Medical University from February 1, 2000, to June 1, 2023. Male patients, those with a history of other malignant tumors, or patients without BM were excluded from the study.
Clinical staging was performed according to the 7th edition of the TNM classification for breast cancer promulgated by the American Joint Committee on Cancer (AJCC). The status of estrogen receptor (ER), progesterone receptor (PR), and HER2 was determined through immunohistochemistry or in situ hybridization analysis of tissues from primary or metastatic lesions. Tumors with ≥1% of cells positive for ER and/or PR were classified as ‘ER and/or PR positive.’ HER2 overexpression/amplification was defined by a 3+ immunohistochemical score or a positive result in fluorescence in situ hybridization. Based on these immunohistochemical results, the patients were categorized into three groups: Luminal subtype group (ER and/or PR positive and HER2 negative), HER2-positive group, and triple-negative group (ER, PR, and HER2 negative).Due to inconsistent Ki-67 index data and lack of routine PR re-testing in this retrospective cohort, further subclassification into Luminal A and Luminal B subtypes was not feasible. All immunohistochemical staining and laboratory procedures were performed following strictly standardized and clinically validated protocols that were in place at our institution during the respective time periods. All staining results were interpreted by experienced two pathologists and were used for critical clinical decision-making.
Systemic treatment regimens
2.2
During the study period, common systemic treatment regimens included: chemotherapy (anthracycline-based, taxane-based, platinum-based agents, etc.); endocrine therapy (aromatase inhibitors, tamoxifen, fulvestrant [for patients with luminal disease]); and targeted therapy (trastuzumab, pertuzumab [for HER2-positive patients]). A proportion of patients with more advanced disease received immunotherapy (e.g., immune checkpoint inhibitors). Specific treatment plans were selected based on tumour subtype, prior therapy, clinical performance status, and patient preference.
BM diagnosis and follow-up
2.3
The diagnosis of brain metastases (BM) is primarily based on clinical manifestations and cranial imaging examinations. Clinical symptoms may include unexplained headaches, vomiting, sensory or motor peripheral/central nervous system symptoms, as well as abnormalities in defecation and urination. Cranial imaging examinations typically involve both plain and enhanced CT scans and MRI scans. Routine practice employs cranial plain and enhanced MRI scans, while plain and enhanced CT scans are recommended for patients with contraindications to MRI. In some cases, where surgery was performed to remove brain metastases, the diagnosis of BM was confirmed through pathological examination.
All breast cancer (BC) patients included in our study were monitored primarily via telephone follow-up or visits to our outpatient clinic, with results recorded meticulously. The follow-up period commenced from the initial diagnosis of BC and continued until the most recent follow-up date, which was gathered up to June 1, 2023. The time from the diagnosis of BC to the diagnosis of BM (TTBM) was defined as the duration from the first diagnosis of breast cancer to the identification of brain metastases. The time from the first recurrence to BM diagnosis (TFR-BM) was defined as the interval from the detection of the first recurrence to the discovery of brain metastases. The first recurrence encompassed both local and distant recurrences of BC. The overall survival from BM diagnosis (OS-BM) was defined as the period from the identification of brain metastases to death or the last follow-up. Finally, the overall survival from BC diagnosis (OS) was determined as the duration from the first diagnosis of breast cancer to death or the last follow-up.
Treatments for BM
2.4
The treatments for BCBM patients were guided by major clinical guidelines and recommendations. Local treatment was prioritized as the preferred modality, while systemic treatment was considered a supplementary approach. Additionally, specific patient and family factors such as economic conditions and patient preferences were taken into account. For symptomatic BCBM patients requiring urgent local brain treatment or those with leptomeningeal metastases, local treatment (either radiotherapy or surgery for BM) was the preferred option. Conversely, asymptomatic BCBM patients were directed towards systemic treatment as the first line of management. During treatment, the effectiveness of the interventions was regularly evaluated, with local treatment implemented in cases of intracranial lesion progression.
Statistical analysis
2.5
Statistical analyses were performed using IBM SPSS Statistics, Version 22.0 (Armonk, NY: IBM Corp). Univariate analysis utilized a one-way ANOVA test, chi-square test, and Fisher’s exact test. A one-way ANOVA test was conducted for the comparison of quantitative indicators among the three groups, while the chi-square test and Fisher’s exact test were employed for comparing sample rates across these groups. The Kaplan-Meier method was used for survival analysis of all patients, and the log-rank test was applied to analyze prognostic differences among groups. P-values <0.05 were considered statistically significant.
Results
3
A total of 249 patients with breast cancer brain metastases (BCBM) were identified, all of whom were female, with a median age of 46 years (range: 23–75 years). Among these patients, 97 (38.95%) had luminal subtype breast cancer, 82 (32.93%) had HER2-positive subtype breast cancer, and 70 (28.11%) had triple-negative breast cancer (TNBC). The most common initial distant metastatic sites in the study population included the lung (151 cases, 60.64%), bone (124 cases, 49.80%), liver (67 cases, 26.91%), and brain (68 cases, 27.31%). Notably, luminal subtype patients exhibited a higher proportion of bone metastases (55.73%, P < 0.001), while HER2-positive patients accounted for the majority of liver metastases (46.34%, P < 0.001). Although TNBC patients had the highest proportion of BM (32.86%), this difference was not statistically significant compared to the other two subtypes. Throughout the disease course, luminal subtype patients were more likely to develop leptomeningeal metastases (19.59%, P = 0.002 < 0.05) (see Table 1).
In terms of CNS-directed treatment, 175 patients (70.28%) underwent radiotherapy for brain metastases. Among these, most patients (69.71%) received whole-brain radiotherapy, while a minority (30.28%) underwent stereotactic radiosurgery. Additionally, 41 patients (16.46%) required neurosurgery, and 26 patients (10.44%) received both radiotherapy and neurosurgery for their brain lesions. Conversely, 59 patients (23.69%) did not receive any local treatments for brain metastases. Systemic disease control rates following BM diagnosis varied by subtype and treatment line, but overall, intracranial disease control was challenging, with many patients experiencing progression despite multimodal therapy.
The median follow-up time for the cohort was 63.1 months (95% CI: 54.6-72.4 months). At the most recent follow-up, 203 patients (81.52%) had died, while 46 (18.47%) were still alive. Over the entire disease course, 84 patients (34.57%) had single BM, whereas 159 patients (65.43%) had multiple BM; the number of BM in 6 patients was not documented. Additionally, 29 patients (11.65%) experienced leptomeningeal metastases. Among the 82 patients with HER2-positive breast cancer, 11 did not receive anti-HER2-targeted therapy after BM diagnosis, while 68 patients did receive such treatment; information on 3 additional patients regarding subsequent anti-HER2-targeted therapy was missing.
The median time from diagnosis of BC to BM diagnosis (TTBM) was 56.6 months for luminal BC, 36.1 months for HER2+ BC, and 28.2 months for TNBC (P < 0.001). The median overall survival after BM diagnosis (OS-BM) was 12.2 months for luminal BC, 27.4 months for HER2+ BC, and 9.2 months for TNBC (P < 0.001) (Table 2, Figures 1A–D). The OS-BM between patients with single versus multiple BM was statistically different (19.2 vs. 11.9 months, P < 0.05). There was a significant difference in OS-BM between patients with and without LM (8.1 vs. 14.8 months, P < 0.001). Additionally, OS-BM differed significantly between patients with BM as the first metastatic site and those without (19.3 vs. 12.5 months, P < 0.05). Furthermore, the difference in OS-BM between HER2+ patients receiving anti-HER2-targeted therapy and those not treated was significant (33.5 vs. 9.1 months, P < 0.001). (Table 3, Figures 2A–D). To account for the evolution of anti-HER2 therapy, we stratified HER2+ patients into pre-2013 (n=28) and post-2013 (n=54) eras. The post-2013 group showed a significantly longer OS-BM (38.1 vs. 11.1 months, P<0.001), likely reflecting improved treatment options.
(A) showed the time from diagnosis of BC to diagnosis of BM. (B) showed the time from first recurrence to diagnosis of BM. (C) showed from diagnosis of BM to death or follow-up time. (D) showed the time from diagnosis of BC to death or follow-up time.
(A) showed the overall survival from BM diagnosis with different numbers of BM. (B) showed the overall survival from BM diagnosis with or without leptomeningeal metastases. (C) showed the overall survival from BM diagnosis with or without BM as the first metastatic site. (D) showed the overall survival from BM diagnosis with or without Anti-HER2 treatment for Her2 positive breast cancer patients.
COX univariable and multivariable analyses identified the following as independent factors influencing overall survival after brain metastasis (OS-BM): the HER2-positive molecular subtype of breast cancer (protective factor), brain metastasis as the first site of metastasis (protective factor), and leptomeningeal metastasis (risk factor) (Table 4).
Discussion
4
With advancements in imaging technology and the enhancement of comprehensive treatment options, the survival time for breast cancer (BC) patients has significantly increased in recent years. As a result, BC patients with prolonged survival may exhibit a greater tendency to develop brain metastases (BM). Consequently, the incidence of BCBM appears to be rising. Our real-world analysis of 249 patients with breast cancer brain metastases (BCBM) elucidates the profound heterogeneity in metastatic patterns, treatment approaches, and survival outcomes across molecular subtypes, providing contemporary evidence to refine the management of this challenging condition.
Our findings firmly establish the molecular subtype as a cornerstone of the BCBM disease trajectory. Consistent with prior literature (15–17), patients with triple-negative breast cancer (TNBC) experienced the shortest median time from breast cancer diagnosis to BM (TTBM) and the poorest overall survival after BM (OS-BM), underscoring the aggressive nature and limited therapeutic options for this subtype. In contrast, patients with HER2-positive disease, while exhibiting a high risk and short TTBM, demonstrated the most favorable OS-BM, with a median survival of 27.4 months. This “survival paradox” is largely attributable to the widespread use and intracranial efficacy of anti-HER2 targeted therapies (18, 19). Our data provide robust support for this, showing a dramatic extension in OS-BM for HER2-positive patients who received anti-HER2 therapy compared to those who did not (33.5 months vs. 9.1 months). This underscores the foundational importance of continuing effective systemic therapy beyond the diagnosis of BM in the modern treatment paradigm for HER2-positive disease (20, 21).
We observed distinct patterns of organotropism among the subtypes. Luminal patients had a higher propensity for bone metastases, whereas HER2-positive patients accounted for the majority of liver metastases, aligning with the intrinsic biological behavior of these cancers (22, 23). A notable finding was the significantly higher incidence of leptomeningeal metastases (LM) in the luminal subtype. Although luminal breast cancer is often characterized by a more indolent course, its specific tropism for the leptomeninges suggests unique tumour-microenvironment interactions and blood-brain barrier penetration mechanisms that warrant further translational investigation (24, 25).
Multivariable Cox regression analysis identified three independent prognostic factors for OS-BM: HER2-positive subtype (protective factor), BM as the first site of distant metastasis (protective factor), and the development of LM (risk factor). BM as the first metastatic site likely portends a better prognosis because it is associated with a lower systemic tumour burden and better performance status, allowing for more aggressive and timely local and systemic interventions (26). Conversely, LM represents a catastrophic prognostic indicator, with our data confirming a median OS-BM of only 8.1 months, highlighting the critical need for improved early detection and novel therapeutic strategies for this complication (27, 28).
Our real-world treatment data reflect contemporary clinical practice. Whole-brain radiotherapy remained the most common local therapy, although stereotactic radiosurgery was used in a substantial minority of cases, reflecting an effort to preserve neurocognitive function in selected patients (29, 30). However, nearly a quarter of the cohort received no local therapy for their BM, a decision likely influenced by poor performance status, extensive extracranial disease, or patient preference, pointing to an area where palliative and supportive care can be optimized (31–33).
Limitations
5
Our study has several limitations. Its retrospective, single-institute design introduces potential for selection bias. The 23-year study period encompasses evolving standards for diagnosis, staging, and treatment, particularly for HER2+ disease, creating patient heterogeneity. Molecular subtyping was based primarily on the primary tumor IHC/FISH, and re-biopsy of metastatic lesions was not routine; thus, subtype conversion could not be assessed, and further biomarker validation (e.g., Ki-67, PIK3CA, BRCA) was not feasible for most patients, limiting deeper biological insights. The sample size, while substantial for a single-center BCBM study, remains relatively modest for extensive subgroup analyses. Details on some systemic treatment regimens and systemic disease control metrics were incomplete in some historical records. Future prospective, multi-center studies with larger cohorts and comprehensive biomarker profiling are warranted.
Conclusion
6
In summary, our real-world analysis elucidates subtype-specific patterns of metastasis and identifies key prognostic factors in BCBM patients. These insights reinforce the importance of molecular subtyping in guiding surveillance and treatment strategies. As therapeutic options continue to expand, individualized approaches that integrate tumor biology, metastatic burden, and patient performance status will be essential to improving outcomes in this high-risk population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fontanella C De Carlo E Cinausero M Pelizzari G Venuti I Puglisi F . Central nervous system involvement in breast cancer patients: is the therapeutic landscape changing too slowly? Cancer Treat Rev. (2016) 46:80–8. doi: 10.1016/j.ctrv.2016.03.014, PMID: 27218867 · doi ↗ · pubmed ↗
- 2Costa R Carneiro BA Wainwright DA Santa-Maria CA Kumthekar P Chae YK . Developmental therapeutics for patients with breast cancer and central nervous system metastasis: current landscape and future perspectives. Ann Oncol. (2017) 28:44–56. doi: 10.1093/annonc/mdw 532, PMID: 28177431 PMC 7360139 · doi ↗ · pubmed ↗
- 3Davis FG Dolecek TA Mc Carthy BJ Villano JL . Toward determining the lifetime occurrence of metastatic brain tumors estimated from 2007 United States cancer incidence data. Neuro Oncol. (2012) 14:1171–7. doi: 10.1093/neuonc/nos 152, PMID: 22898372 PMC 3424213 · doi ↗ · pubmed ↗
- 4Vogelbaum MA Brown PD Messersmith H Brastianos PK Burri S Cahill D . Treatment for brain metastases: ASCO-SNO-ASTRO guideline. J Clin Oncol. (2022) 40:492–516. doi: 10.1200/JCO.21.02314, PMID: 34932393 · doi ↗ · pubmed ↗
- 5Lin NU Bellon JR Winer EP . CNS metastases in breast cancer. J Clin Oncol. (2004) 22:3608–17. doi: 10.1200/JCO.2004.01.175, PMID: 15337811 · doi ↗ · pubmed ↗
- 6Cruz-Muñoz W Kerbel RS . Preclinical approaches to study the biology and treatment of brain metastases. Semin Cancer Biol. (2011) 21:123–30. doi: 10.1016/j.semcancer.2010.12.001, PMID: 21147227 PMC 4540600 · doi ↗ · pubmed ↗
- 7Matsuo S Watanabe J Mitsuya K Hayashi N Nakasu Y Hayashi M . Brain metastasis in patients with metastatic breast cancer in the real world: a single-institution, retrospective review of 12-year follow-up. Breast Cancer Res Treat. (2017) 162:169–79. doi: 10.1007/s 10549-017-4107-x, PMID: 28084583 · doi ↗ · pubmed ↗
- 8Altundag K Bondy ML Mirza NQ Kau SW Broglio K Hortobagyi GN . Clinicopathologic characteristics and prognostic factors in 420 metastatic breast cancer patients with central nervous system metastasis. Cancer. (2007) 110:2880–7. doi: 10.1002/cncr.23088, PMID: 17960791 · doi ↗ · pubmed ↗