Case Report: Trastuzumab deruxtecan in human epidermal growth factor receptor 2-mutated lung cancer with continuous renal replacement therapy
Sumin Wu, Chengming Ke, Min Wei

TL;DR
A patient with HER2-mutated lung cancer and kidney failure received trastuzumab deruxtecan, showing disease control with manageable side effects.
Contribution
First reported case of T-DXd use in a CRRT-dependent patient with HER2-mutant lung cancer.
Findings
T-DXd achieved disease control with symptomatic improvement in a patient on CRRT.
No significant nephrotoxicity or interstitial lung disease was observed.
Patient experienced severe myelosuppression but it resolved with supportive care.
Abstract
Human epidermal growth factor receptor 2 (HER2)-mutated lung cancer is a rare and aggressive subtype of non-small cell lung cancer (NSCLC), characterized by poor prognosis and limited response to conventional therapies. Trastuzumab deruxtecan (T-DXd), a HER2-targeting antibody-drug conjugate (ADC), has shown promising results in HER2-mutated cancers. However, its safety and efficacy in patients with renal dysfunction requiring continuous renal replacement therapy (CRRT) remain unclear. A 69-year-old female with advanced HER2-mutant NSCLC developed acute kidney injury (AKI) requiring intermittent CRRT after failing standard chemotherapy. With strong patient commitment, T-DXd was initiated following multidisciplinary discussion. Although severe myelosuppression occurred following targeted therapy, it resolved with appropriate supportive care. Notably, no significant toxicities such as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
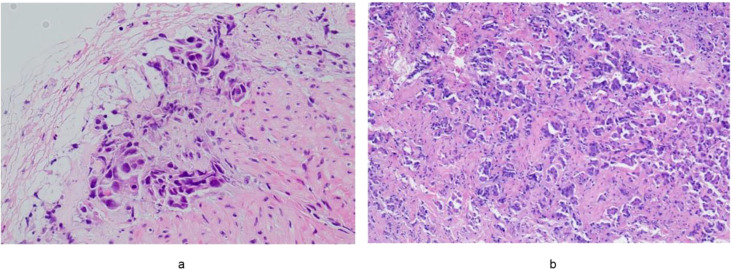 Figure 1
Figure 1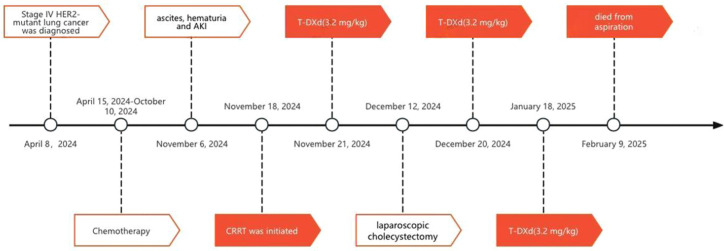 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHER2/EGFR in Cancer Research · Lung Cancer Treatments and Mutations · Lung Cancer Research Studies
Introduction
Human epidermal growth factor receptor 2 (HER2) mutations have been increasingly recognized as a critical driver of malignancy in non-small cell lung cancer (NSCLC) (1), particularly in patients with advanced or metastatic disease. HER2-mutant lung cancer is known for its aggressive clinical course, poor prognosis, and resistance to conventional therapies, including chemotherapy and immunotherapy (2). Targeted therapies designed to inhibit HER2, such as trastuzumab deruxtecan (T-DXd), have demonstrated efficacy in other cancers, including breast cancer (3). T-DXd is now the recommended second-line therapy for HER2-mutant NSCLC per NCCN and other international guidelines, following platinum-based chemotherapy (4, 5).
Continuous Renal Replacement Therapy (CRRT) is primarily used in cancer patients to manage critical conditions complicated by acute kidney injury (AKI), particularly tumor lysis syndrome, septic shock, or anticancer drug-related nephrotoxicity. Compared to intermittent hemodialysis, CRRT offers slower and sustained solute clearance and ultrafiltration, which enables better hemodynamic stability, precise fluid balance control, and effective removal of inflammatory mediators and certain chemotherapeutic agents (6). It provides continuous support for renal function, allowing for the removal of waste products, fluid management, and the correction of electrolyte imbalances (7). However, its use in cancer patients, particularly those undergoing targeted therapy, has been less well-documented. This case explores the combination of T-DXd with CRRT in a patient with advanced HER2-mutant lung cancer, highlighting the potential clinical significance and safety of this approach.
Case presentation
The patient was a 69-year-old woman with a history of hypertension for over 10 years. In March 2024, she presented to a local hospital with a one-month history of recurrent cough and dyspnea. Physical examination revealed diminished breath sounds in the right lung. Chest CT imaging identified a large right pleural effusion. Thoracentesis and drainage were performed, and cytological analysis of the pleural fluid revealed numerous atypical cells. Whole-body PET/CT demonstrated focal thickening of the mid-to-distal esophageal wall, along with multiple FDG-avid enlarged lymph nodes in the bilateral supraclavicular regions, right axilla, medial to the right pectoralis minor muscle, bilateral hilar and mediastinal areas, parasternal region, right anterior costophrenic angle, gastrohepatic space, and para-aortic regions, highly suggestive of esophageal carcinoma with lymph node metastasis. Gastroscopy confirmed focal thickening in the lower thoracic esophagus, while colonoscopy was unremarkable. Endoscopic ultrasound-guided biopsy of the esophageal lesion revealed fibrous connective and smooth muscle tissue infiltrated by clusters and scattered individual cells with enlarged, eccentrically located nuclei. The histopathological diagnosis was malignant tumor, consistent with invasive adenocarcinoma. Based on imaging and immunohistochemical findings, a pulmonary origin was considered most likely (Figure 1a). Immunohistochemistry results were as follows: P40 (–), CK7(+), TTF-1(+), Napsin A(–), ALK (D5F3)(–), ALK-N(–), CEA(–), Villin(–), STAB2(–), GATA-3 (focally+), CK5/6(–), CDX2 (rare weakly+).Next-generation sequencing (NGS) identified an ERBB2 exon 19 p.L755P missense mutation (variant allele frequency: 15.82%), a TP53 mutation, and MYC gene amplification. The final diagnosis was stage IV poorly differentiated HER2-mutant lung adenocarcinoma.
(a) Hematoxylin and eosin staining (HE×20) of a biopsy specimen obtained by gastroscopy revealing lung-derived esophageal metastasis. (b) Hematoxylin and eosin staining (HE×20) of a biopsy specimen obtained by cystoscopy revealing lung-derived bladder metastasis.
From April 15 to July 30, 2024, the patient received first-line therapy with six cycles of pemetrexed, carboplatin, pembrolizumab, and bevacizumab. During treatment, her serum creatinine rose from normal to 102.8 μmol/L(1.16mg/dL), necessitating dose reduction of the chemotherapeutic agents. On August 20, 2024, she developed abdominal distension and gross hematuria. Follow-up CT imaging indicated disease progression, prompting a change in regimen to albumin-bound paclitaxel, cisplatin, pembrolizumab, and bevacizumab. Her symptoms progressively worsened, accompanied by anorexia and postprandial vomiting.
She was transferred to our institution for further management on November 6, 2024. Physical examination revealed pale skin and mucous membranes, reduced breath sounds on the right, marked abdominal distension, and shifting dullness. Laboratory studies showed hemoglobin at 86 g/L and serum creatinine elevated to 210.24 μmol/L(2.38mg/dL). Whole-body contrast-enhanced CT revealed disease progression with new findings including multiple right lung lesions, numerous hepatic metastases, diffuse gastric wall thickening, diffuse bladder wall thickening, thickening of the left ureter’s pelvic segment with associated left hydronephrosis, peritoneal thickening and extensive ascites. Pathological assessment of a bladder biopsy confirmed metastatic lung adenocarcinoma (Figure 1b). Immunohistochemistry of the tumor cells showed TTF-1(+), ER(–), GATA3(–), SOX-10(–), and Mammaglobin(–).During hospitalization, she underwent drainage of right pleural effusion and ascites, along with supportive care. On November 16, 2024, she developed oliguria and generalized edema. Blood tests revealed hyperkalemia, metabolic acidosis, and a progressive rise in serum creatinine to 616.42 μmol/L(6.97mg/dL). CRRT in Continuous Veno-Venous Hemofiltration (CVVH) mode was initiated on November 18, 2024, for life support. Despite AKI, after thorough discussion and respecting the patient’s strong preference, targeted therapy with T-DXd at 3.2 mg/kg was administered on November 21, 2024. The second and third cycles of T-DXd were given on December 20, 2024, and January 18, 2025, respectively.
Treatment-related toxicities were manageable. Hematologic adverse events included grade III neutropenia and thrombocytopenia following targeted therapy, both resolving with supportive measures. Significant hepatic or pulmonary toxicity was not observed. Regarding renal function, CRRT was discontinued on November 28, 2024, following clinical improvement characterized by urine output exceeding 1000 mL/day, decline in serum creatinine to approximately 250 μmol/L(2.82mg/dL), and stabilization of her internal environment. However, due to a subsequent rebound in creatinine, CRRT was resumed on January 17, 2025. Notably, on December 12, 2024, prior to the second T-DXd cycle, she underwent laparoscopic cholecystectomy for cholecystitis; pathology confirmed metastatic lung adenocarcinoma involving the gallbladder wall. After three cycles of T-DXd treatment, her clinical condition improved, with alleviated abdominal distension, significantly reduced ascites, and resolved hematuria. A follow-up CT scan on January 20, 2025, showed stable disease with minimal regression in some mediastinal, bilateral hilar, and axillary lymph nodes, as well as hepatic metastases. Unfortunately, the patient died due to aspiration on February 9, 2025 (Figure 2).
Flow chart of patient from diagnosis to current treatment. HER2, human epidermal growth factor receptor 2; AKI, acute kidney injury; CRRT, continuous renal replacement therapy; T-DXd, trastuzumab deruxtecan.
Discussion
HER2-mutant lung cancer demonstrates a more aggressive clinical course and distinct metastatic behavior (8). The metastatic spread in this case was extensive. HER2-mutant lung cancer is generally poorly responsive to conventional chemotherapy and immunotherapy (9), as observed in this patient. T-DXd has been shown to be effective in treating adult patients with unresectable locally advanced or metastatic NSCLC harboring HER2 (ERBB2) activating mutations (5, 10). T-DXd is an antibody-drug conjugate (ADC) targeting HER2. It consists of a humanized anti-HER2 immunoglobulin G1 (IgG1) monoclonal antibody linked to the topoisomerase I inhibitor DXd. Upon binding to HER2 receptors on tumor cells, T-DXd undergoes internalization, and its linker is cleaved by lysosomal enzymes. The released DXd induces DNA damage, leading to tumor cell apoptosis (4). Pharmacokinetic studies have shown that DXd is primarily metabolized by CYP3A4 in the liver and excreted via bile, with most of the drug appearing in urine, feces, and bile (5). The pharmacokinetics of T-DXd or its released DXd are not affected by mild to moderate renal impairment (11). However, caution is advised in patients with severe renal impairment or undergoing dialysis, as there are no studies in these populations (12).
In this case, T-DXd was initiated during continuous renal replacement therapy (CRRT) for acute kidney injury (AKI). Nephrology consultation confirmed that the AKI was multifactorial in origin, attributable to renal hypoperfusion from inadequate intake and third-space fluid sequestration, nephrotoxic effects of prior chemotherapy (particularly platinum-based agents), and obstructive uropathy secondary to bladder metastasis with associated left hydronephrosis. Although severe myelosuppression occurred following targeted therapy, it resolved with appropriate supportive care. Notably, no significant toxicities such as interstitial lung disease, hepatotoxicity, or further nephrotoxicity were observed. During the treatment course, the patient also successfully underwent cholecystectomy. After three cycles of T-DXd, symptomatic improvement was achieved, including resolution of abdominal distension, significant reduction of ascites, and disappearance of hematuria. Follow-up imaging studies confirmed stable disease. Together, these findings suggest meaningful clinical benefit from T-DXd in this complex clinical scenario. Nonetheless, the patient’s short overall survival period necessitates cautious interpretation of these findings, and further investigations are required to validate these observations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chevallier M Borgeaud M Addeo A Friedlaender A . Oncogenic driver mutations in non-small cell lung cancer: Past, present and future. World J Clin Oncol. (2021) 12:217. doi: 10.5306/wjco.v 12.i 4.217, PMID: 33959476 PMC 8085514 · doi ↗ · pubmed ↗
- 2Ren S Wang J Ying J Mitsudomi T Lee DH Wang Z . Consensus for HER 2 alterations testing in non-small-cell lung cancer. ESMO Open. (2022) 7:100395. doi: 10.1016/j.esmoop.2022.100395, PMID: 35149428 PMC 8844658 · doi ↗ · pubmed ↗
- 3Lau KH Tan AM Shi Y . New and emerging targeted therapies for advanced breast cancer. Int J Mol Sci. (2022) 23:2288. doi: 10.3390/ijms 23042288, PMID: 35216405 PMC 8874375 · doi ↗ · pubmed ↗
- 4Li BT Smit EF Goto Y Nakagawa K Udagawa H Mazières J . Trastuzumab deruxtecan in HER 2-mutant non-small-cell lung cancer. New Engl J Med. (2022) 386:241–51. doi: 10.1056/NEJ Moa 2112431, PMID: 34534430 PMC 9066448 · doi ↗ · pubmed ↗
- 5Goto K Goto Y Kubo T Ninomiya K Kim SW Planchard D . Trastuzumab deruxtecan in patients with HER 2-mutant metastatic non-small-cell lung cancer: primary results from the randomized, phase II DESTINY-lung 02 trial. J Clin Oncol Off J Am Soc Clin Oncol. (2023) 41:4852–63. doi: 10.1200/JCO.23.01361, PMID: 37694347 PMC 10617843 · doi ↗ · pubmed ↗
- 6Darmon M Vincent F Camous L Canet E Bonmati C Braun T . Tumour lysis syndrome and acute kidney injury in high-risk haematology patients in the rasburicase era. A prospective multicentre study from the Groupe de Recherche en Réanimation Respiratoire et Onco-Hématologique. Br J haematology. (2013) 162:489–97. doi: 10.1111/bjh.12415, PMID: 23772757 · doi ↗ · pubmed ↗
- 7Perner A Prowle J Joannidis M Young P Hjortrup PB PettiläV . Fluid management in acute kidney injury. Intensive Care Med. (2017) 43:807–15. doi: 10.1007/s 00134-017-4817-x, PMID: 28470347 · doi ↗ · pubmed ↗
- 8Fois SS Paliogiannis P Zinellu A Fois AG Cossu A Palmieri G . Molecular epidemiology of the main druggable genetic alterations in non-small cell lung cancer. Int J Mol Sci. (2021) 22:612. doi: 10.3390/ijms 22020612, PMID: 33435440 PMC 7827915 · doi ↗ · pubmed ↗