Utility of extended HPV genotyping in cervical cancer screening: a prospective population-based cohort study in China
Kexin Yi, Jinyu Zhang, Hong Wang, Peipei Chen, Xingyuan Sun, Mengjie Li, Shaokai Zhang

TL;DR
This study shows that extended HPV genotyping improves cervical cancer screening accuracy in China by identifying more high-risk HPV types beyond HPV16/18.
Contribution
Demonstrates the clinical benefit of extended HPV genotyping in a high-burden population with diverse oncogenic genotypes.
Findings
HPV16/18/33/52/58 genotyping increased CIN2+ sensitivity to 55.1% compared to 51.0% for HPV16/18 alone.
Non-16/18 genotypes like HPV33/58 showed comparable CIN2+ risks to HPV16/18, with 96-fold higher risk than HR-HPV negatives.
Extended genotyping maintained high specificity (>93%) while improving screening sensitivity in a Chinese cohort.
Abstract
Cervical cancer poses a substantial global health burden, particularly in China where it contributes substantially to incidence and mortality. Conventional HR-HPV screening tests primarily target HPV16/18, limiting efficacy in regions dominated by other oncogenic genotypes and underscoring the need for extended genotyping to refine risk-stratified approaches. This prospective cohort in Henan Province, China (2017–2020), enrolled 3,299 women aged 21–64 for baseline HR-HPV testing using an extended genotyping assay detecting 14 types and identifying HPV16/18/33/52/58. HR-HPV-positives were followed annually, negatives at year 3. Three-year cumulative CIN2+/CIN3+ risks, sensitivity, specificity, PPV, and NPV were computed independent of cytology. Baseline HR-HPV positivity was 18.3%. Over 3 years, 98 CIN2+ and 60 CIN3+ cases were detected. Absolute CIN2+ risks was highest for HPV16…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
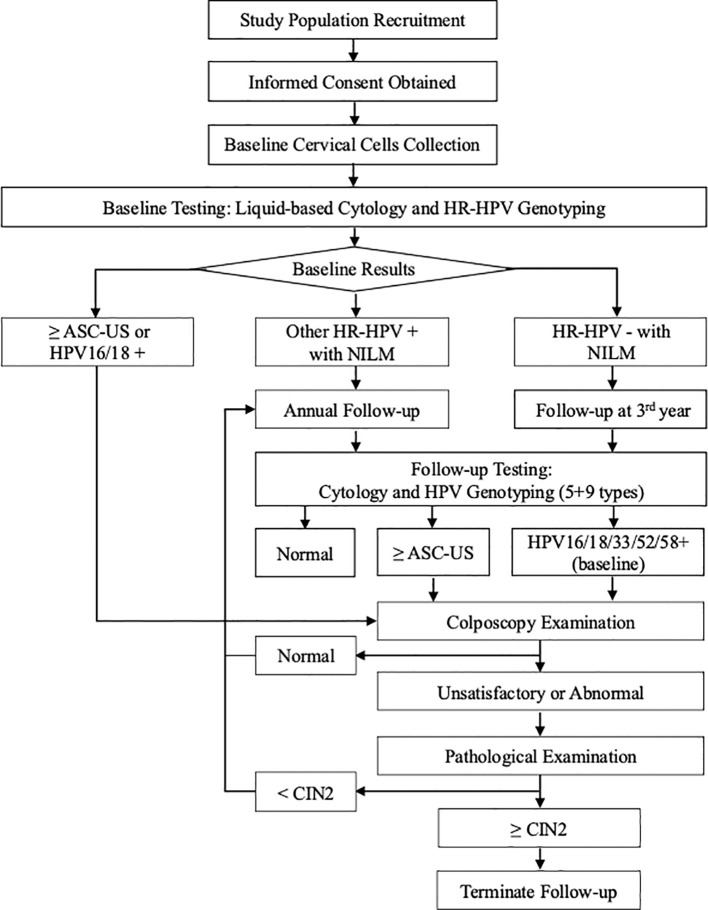 Figure 1
Figure 1| Baseline HPV infection | N (%) | Baseline (n) | 1st year (n) | 2nd year (n) | 3rd year (n) | Overall | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CIN2+ | CIN3+ | CIN2+ | CIN3+ | CIN2+ | CIN3+ | CIN2+ | CIN3+ | CIN2+ | CIN3+ | ||
| HR-HPV positive | 604 (18.3) | 43 | 29 | 18 | 16 | 18 | 8 | 12 | 6 | 91 | 59 |
| HPV16 positive | 128 (3.9) | 26 | 20 | 6 | 6 | 7 | 2 | 3 | 1 | 42 | 29 |
| HPV18 positive | 39 (1.2) | 9 | 5 | 0 | 0 | 0 | 0 | 2 | 1 | 11 | 6 |
| HPV52 positive | 138 (4.2) | 10 | 7 | 5 | 4 | 5 | 2 | 2 | 1 | 22 | 14 |
| HPV58 positive | 108 (3.3) | 11 | 6 | 7 | 6 | 4 | 2 | 5 | 2 | 27 | 16 |
| HPV33 positive | 46 (1.4) | 3 | 3 | 2 | 2 | 3 | 1 | 4 | 3 | 12 | 9 |
| HPV16/18 positive | 159 (4.8) | 32 | 22 | 6 | 6 | 7 | 2 | 5 | 2 | 50 | 32 |
| HPV52/58/33 positive | 266 (8.1) | 22 | 16 | 13 | 11 | 11 | 5 | 8 | 4 | 54 | 36 |
| Other nine types positive | 329 (10.0) | 15 | 9 | 5 | 5 | 12 | 5 | 5 | 1 | 37 | 20 |
| HR-HPV negative | 2695 (81.7) | 1 | 0 | 0 | 0 | 2 | 1 | 4 | 0 | 7 | 1 |
| Total | 3299 | 44 | 29 | 18 | 16 | 20 | 9 | 16 | 6 | 98 | 60 |
| Baseline HPV infection | Absolute risk (%, 95%CI) of CIN2+ | Relative risk (%, 95%CI) of CIN2+ | |
|---|---|---|---|
| HR-HPV negative | Other nine types positive | ||
| HR-HPV positive | 15.07 (12.43, 18.15) | 58.00 (27.03, 124.50) | — |
| HPV16 positive | 32.81 (25.27, 41.36) | 126.30 (57.90, 275.60) | 2.92 (1.97, 4.32) |
| HPV18 positive | 28.21 (16.42, 43.90) | 108.60 (44.45, 265.30) | 2.51 (1.40, 4.50) |
| HPV52 positive | 15.94 (10.70, 23.03) | 61.38 (26.68, 141.20) | 1.42 (0.87, 2.31) |
| HPV58 positive | 25.00 (17.74, 33.97) | 96.25 (42.87, 216.10) | 2.22 (1.42, 3.47) |
| HPV33 positive | 26.09 (15.47, 40.38) | 100.40 (41.44, 243.40) | 2.32 (1.31, 4.12) |
| HPV16/18 positive | 31.45 (24.73, 39.04) | 121.10 (55.80, 262.70) | 2.80 (1.91, 4.09) |
| HPV58/52/33 positive | 20.30 (15.89, 25.56) | 78.16 (35.93, 170.00) | 1.80 (1.23, 2.66) |
| Other nine types positive | 11.25 (8.24, 15.15) | 43.30 (19.46, 96.33) | — |
| HR-HPV negative | 0.26 (0.11, 0.55) | — | — |
| Total | 2.97 (2.44, 3.61) | — | — |
| Baseline HPV infection | Absolute risk (%, 95%CI) of CIN3+ | Relative risk (%, 95%CI) of CIN3+ | |
|---|---|---|---|
| HR-HPV negative | Other nine types positive | ||
| HR-HPV positive | 9.77 (7.64, 12.41) | 263.30 (36.55, 1896.00) | — |
| HPV16 positive | 22.66 (16.22, 30.68) | 610.60 (83.84, 4446.00) | 3.73 (2.19, 6.34) |
| HPV18 positive | 15.38 (6.86, 30.11) | 414.60 (51.12, 3363.00) | 2.53 (1.08, 5.92) |
| HPV52 positive | 10.14 (6.03, 16.42) | 273.40 (36.22, 2064.00) | 1.67 (0.87, 3.21) |
| HPV58 positive | 14.81 (9.22, 22.82) | 399.30 (53.44, 2983.00) | 2.44 (1.31, 4.53) |
| HPV33 positive | 19.57 (10.43, 33.39) | 527.30 (68.21, 4076.00) | 3.22 (1.56, 6.64) |
| HPV16/18 positive | 20.13 (14.59, 27.07) | 542.40 (74.60, 3943.00) | 3.31 (1.96, 5.60) |
| HPV58/52/33 positive | 13.53 (9.91, 18.20) | 364.70 (50.21, 2649.00) | 2.23 (1.32, 3.75) |
| Other nine types positive | 6.08 (3.92, 9.25) | 163.80 (22.06, 1217.00) | — |
| HR-HPV negative | 0.04 (0.00, 0.23) | — | — |
| Total | 1.82 (1.41, 2.34) | — | — |
| Baseline HPV infection | N | Sensitivity (%, 95% CI) | Specificity (%, 95% CI) | PPV (%, 95% CI) | NPV (%, 95% CI) |
|---|---|---|---|---|---|
| HR-HPV positive | 604 | 92.86 (85.98, 96.50) | 83.97 (82.66, 85.2) | 15.07 (12.43, 18.14) | 99.74 (99.46, 99.87) |
| HPV16 positive | 128 | 42.86 (33.51, 52.74) | 97.31 (96.69, 97.82) | 32.81 (25.28, 41.34) | 98.23 (97.71, 98.64) |
| HPV18 positive | 39 | 11.22 (6.38, 18.99) | 99.13 (98.74, 99.39) | 28.21 (16.54, 43.78) | 97.33 (96.72, 97.83) |
| HPV52 positive | 138 | 22.45 (15.32, 31.66) | 96.38 (95.67, 96.97) | 15.94 (10.77, 22.96) | 97.60 (97.00, 98.07) |
| HPV58 positive | 108 | 27.55 (19.68, 37.12) | 97.47 (96.87, 97.96) | 25.00 (17.79, 33.93) | 97.77 (97.20, 98.23) |
| HPV33 positive | 46 | 12.24 (7.15, 20.19) | 98.94 (98.52, 99.24) | 26.09 (15.60, 40.26) | 97.36 (96.75, 97.85) |
| HPV16/18 positive | 159 | 51.02 (41.27, 60.69) | 96.59 (95.91, 97.17) | 31.45 (24.74, 39.03) | 98.47 (97.98, 98.85) |
| HPV58/52/33 positive | 266 | 55.10 (45.25, 64.57) | 93.38 (92.46, 94.19) | 20.30 (15.91, 25.54) | 98.55 (98.06, 98.92) |
| Other nine types positive | 329 | 37.76 (28.79, 47.64) | 90.88 (89.83, 91.83) | 11.25 (8.27, 15.12) | 97.95 (97.37, 98.40) |
| Baseline HPV infection | N | Sensitivity (%, 95% CI) | Specificity (%, 95% CI) | PPV (%, 95% CI) | NPV (%, 95% CI) |
|---|---|---|---|---|---|
| HR-HPV positive | 604 | 98.33 (91.14, 99.71) | 83.84 (82.52, 85.07) | 10.21 (8.00, 12.94) | 99.96 (99.79, 99.99) |
| HPV16 positive | 128 | 48.33 (36.17, 60.69) | 97.26 (96.64, 97.77) | 24.79 (17.85, 33.33) | 99.02 (98.61, 99.31) |
| HPV18 positive | 39 | 10.00 (4.66, 20.15) | 99.10 (98.71, 99.37) | 17.14 (8.10, 32.68) | 98.33 (97.83, 98.72) |
| HPV52 positive | 138 | 23.33 (14.44, 35.44) | 96.36 (95.65, 96.95) | 10.69 (6.47, 17.14) | 98.54 (98.05, 98.90) |
| HPV58 positive | 108 | 26.67 (17.13, 39.01) | 97.38 (96.77, 97.88) | 16.00 (10.10, 24.42) | 98.61 (98.14, 98.96) |
| HPV33 positive | 46 | 15.00 (8.10, 26.11) | 98.91 (98.49, 99.22) | 20.45 (11.15, 34.50) | 98.42 (97.93, 98.80) |
| HPV16/18 positive | 159 | 53.33 (40.89, 65.37) | 96.51 (95.82, 97.09) | 22.22 (16.20, 29.68) | 99.10 (98.71, 99.38) |
| HPV58/52/33 positive | 266 | 60.00 (47.37, 71.43) | 93.27 (92.35, 94.09) | 14.29 (10.50, 19.14) | 99.21 (98.82, 99.47) |
| Other nine types positive | 329 | 33.33 (22.73, 45.94) | 90.78 (89.73, 91.73) | 6.33 (4.13, 9.57) | 98.65 (98.16, 99.00) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Head and Neck Cancer Studies · Women's cancer prevention and management
Introduction
Cervical cancer represents one of the most preventable malignancies, primarily caused by persistent infection with high-risk human papillomavirus (HR-HPV) genotypes (1). Despite substantial progress in vaccination and screening, its incidence has not been fully controlled over decades. In 2022, an estimated 660,000 new cases and 350,000 deaths occurred worldwide, ranking it as the fourth most common cancer among women (2). In China, approximately 150,700 new cases and 55,700 deaths were reported that year, accounting for 22.8% of global incidence and 15.9% of mortality (3), placing the country at a high burden level internationally.
The World Health Organization (WHO) launched the Global Strategy to Accelerate the Elimination of Cervical Cancer in 2020, targeting “90-70-90” by 2030, where the “70” refers to 70% of women receiving effective screening by ages 35 and 45 (4). Current screening modalities include cytology and HR-HPV testing (5). Cytology, however, suffers from limitations such as low sensitivity, reliance on subjective interpretation, and quality control challenges (6). In contrast, HR-HPV testing provides high sensitivity and reproducibility, detecting more precancerous lesions and cancers than cytology (7). In recent years, many countries have adopted HR-HPV testing as a primary or co-testing method, with guidelines from the United States, Australia, France, the United Kingdom, India, and Brazil endorsing it for primary screening (8–14). In 2021, WHO published the second edition of its “Guidelines for Screening and Treatment of Cervical Precancerous Lesions”, which recommends HPV DNA testing as the preferred screening approach and specifies that HR-HPV assays typically detect 14 genotypes: HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68 (15).
Globally, the predominant HR-HPV types in cervical cancer are HPV16 (55.2%), 18 (14.2%), 45 (5.0%), 33 (4.2%), and 58 (3.9%) (16). While HPV16, HPV18, and HPV45 are most oncogenic in the USA and Europe, HPV16, HPV58, and HPV52 are more prevalent in China and other Asia countries (17, 18). Risk of progression to cervical lesions varies by HR-HPV type (19, 20), with HPV31, 33, 52, and 58 posing elevated risks for low- and high-grade squamous intraepithelial lesions (LSIL/HSIL) after HPV16/18 (21, 22). This regional heterogeneity poses a challenge for standard HPV16/18-focused screening, potentially leading to suboptimal risk assessment and missed opportunities for early intervention in Asian populations. To address this, this prospective population-based cohort study evaluated the practical utility of extended genotyping in screening by assessing 3-year risks of precancerous lesions and cancer associated with different HR-HPV types in Chinese women, independent of cytology, thereby providing evidence to support its adoption for refined, risk-based screening strategies.
Methods
Study population and inclusion criteria
A population-based cervical cancer screening cohort was established in Jiyuan City, Henan Province, China, from April to May 2017, with participants followed for 3 years until September 2020. Eligible women were aged 21–64 years, had an intact cervix, were not pregnant or within 8 weeks postpartum, had no history of hysterectomy, cervical surgery, or cervical cancer treatment, and could provide informed consent and undergoing routine screening. The study was approved by the Institutional Ethics Committee of the Affiliated Cancer Hospital of Zhengzhou University (2017009).
Sample collection
All eligible women underwent a gynecological examination, during which cervical samples were collected using a broom-type brush at baseline and during follow-up visits. Exfoliated cells were preserved in PreservCyt solution (Hologic Inc., Boston, USA) and stored at 4°C for subsequent liquid-based cytology and HPV DNA testing. Colposcopy was performed by experienced colposcopists. If adequate visualization was achieved during colposcopy and lesions were identified, tissue biopsy was obtained from the abnormal sites; if visualization was inadequate, endocervical curettage (ECC) was performed.
Laboratory detection
All testing and diagnostic procedures were performed in a strictly blinded manner. HPV genotyping was conducted using HR-HPV (5 + 9) DNA Genotyping Kit (Tellgen Cor., Shanghai, China), based on multiple nucleic acid amplification polymerase chain reaction (PCR) method with fluorescence detection. This assay detects 14 HR-HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) in cervical exfoliated cells and specifically identifies HPV types 16, 18, 33, 52, and 58. Each run included positive, negative, and blank controls, along with amplification of the reference gene β-Globin to identify false negatives due to inadequate sampling or procedural errors.
Cervical cells were stained and evaluated according to The Bethesda System (TBS). Satisfactory cytological samples were classified as negative for intraepithelial lesion or malignancy (NILM), atypical squamous cells undetermined significance (ASC-US), atypical squamous cells, atypical squamous cells cannot exclude high-grade squamous intraepithelial (ASC-H), atypical glandular cells (AGC), low-grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion (HSIL), squamous cell carcinoma (SCC), adenocarcinoma in situ (AIS), adenocarcinoma (ADC). NILM was considered normal liquid-based cytology (LBC). Biopsy or ECC samples were evaluated by pathologists at the Affiliated Cancer Hospital of Zhengzhou University using the cervical intraepithelial neoplasia (CIN) classification system.
Baseline screening and follow-up procedures
At baseline, women with ASC-US or worse cytology (≥ASC-US) or HPV16/18 positivity were immediately referred for colposcopy. Those with abnormal colposcopy findings underwent biopsy and histopathological examination. A diagnosis of CIN2 or worse (CIN2+), concluding participation; otherwise, follow-up continued.
HR-HPV-positive women at baseline were followed annually, while HR-HPV -negative women were reassessed at the third year. During follow-up, all participants underwent cytology and HPV DNA (5 + 9) testing. Women with normal cytology results continued to the next year visit. Women with ≥ASC-US cytology during the follow-up or baseline HPV16/18/33/52/58 positivity were referred to colposcopy, followed by biopsy and histopathological diagnosis if abnormal. CIN2+ was confirmed as the positive outcome; absence of CIN2+ by study end was deemed negative (Figure 1).
Flowchart of baseline screening and follow-up procedures. NILM, negative for intraepithelial lesion or malignancy; HPV, human papillomavirus; HR-HPV, high-risk HPV; CIN2, cervical intraepithelial neoplasia grade 2; ASC-US, atypical squamous cells undetermined significance.
Statistical analysis
Data analysis was performed using SAS version 9.4 (SAS Institute Inc., NC, USA). Continuous variables were presented as mean ± standard deviation (SD), and categorical variables as frequencies and percentages. Three-year cumulative absolute and relative risks of CIN2+ and CIN3 or worse (CIN3+), with 95% confidence intervals (95% CIs), were calculated for different baseline HR-HPV genotypes, irrespective of cytology. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for baseline HR-HPV results in detecting cumulative CIN2+ and CIN3+ over three-year period. CIN2+ served as the primary clinical endpoint. Two-sided P-values ≤0.05 were considered statistically significant.
Results
Of 4,026 eligible women enrolled in the baseline screening cohort, 3,299 (81.9%) completed the 3-year follow-up and were included in the analysis after excluding 727 (18.1%) lost to follow-up or not reaching endpoints. The mean age was 47.00 ± 9.69 years (range, 21–64 years). No significant differences were observed between completers and non-completers in baseline characteristics and HPV positivity. At baseline, HR-HPV positivity was 18.3% (604/3,299), with HPV16/18 and HPV52/58/33 being the most prevalent high-risk groups (4.8% and 8.1%, respectively), while other nine types accounted for 10.0% (Table 1). Over the study period, 98 CIN2+ cases and 60 CIN3+ cases were identified, with 44 CIN2+ and 29 CIN3+ at baseline, 18 CIN2+ and 16 CIN3+ during the first follow-up year, 20 CIN2+ and 9 CIN3+ during the second year, and 16 CIN2+ and 6 CIN3+ during the third year. Among CIN2+ cases, 93% (91/98) were baseline HR-HPV positive, predominantly involving HPV16/18 (51%) or HPV52/58/33 (55%), as detailed in Table 1.
Women with different baseline HPV statuses exhibited varying 3-year absolute and relative risks of CIN2 +. Absolute risks were highest for HPV16 (32.81%; 95% CI, 25.27-41.36%) and comparable among HPV18, HPV33, and HPV58 (25-28%), exceeding 15% for HPV52 and dropping to <12% for other types, with HR-HPV-negatives at 0.26%. Relative risks versus HR-HPV-negatives surpassed 96-fold for HPV16/18/33/58, while comparisons to other types showed HPV16 conferring the greatest elevation (2.92%; 95% CI, 1.97-4.32%), underscoring the disproportionate contribution of these genotypes in Chinese women (Table 2).
A similar pattern emerged for CIN3+ (Table 3), with absolute risks peaking at 22.66% (95% CI, 16.22-30.68%) for HPV16 and ranging 14-20% for HPV18/33/58, versus <11% for HPV52 and other types, and 0.04% (95% CI, 0.00-0.23%) for negatives. Relative to HR-HPV-negatives, risks were markedly elevated (>400-fold) for HPV16/18/33/58. Compared with other nine types positives, HPV16 again showed the greatest relative risk (3.73%; 95%CI, 2.19-6.34%), followed by HPV16/18 (3.31%; 95%CI, 1.96-5.60%), with HPV52 the lowest (1.67%; 95%CI, 0.87-3.21%) (Table 3), highlighting genotype-specific progression potential.
Using histopathology as the gold standard, baseline HPV genotyping exhibited robust diagnostic performance for detecting cumulative 3-year CIN2+ and CIN3+ lesions (Tables 4 and 5). For CIN2+, overall HR-HPV positivity yielded high sensitivity (92.86%; 95%CI, 85.98-96.50%) but moderate specificity (83.97%; 95%CI, 82.66-85.20%), with near-perfect NPV of 99.74% (95%CI, 99.46-99.87%). HPV16/18 positivity balanced sensitivity (51.02%; 95%CI, 41.27-60.69%) and high specificity (96.59%; 95%CI, 95.91-97.17%), while extending to HPV52/58/33 modestly improved sensitivity (55.10%; 95%CI, 45.25-64.57%) at maintained high specificity (>93%) and NPV (>98%). For CIN3+, sensitivities were even higher (98.33% for HR-HPV; 60.00% for HPV52/58/33), with NPVs approaching 100%, supporting extended genotyping’s utility in risk stratification.
Discussion
Traditional HR-HPV assays primarily target the most common oncogenic genotype, especially HPV16 and 18. However, accumulating evidence highlights the substantial oncogenic contributions of other genotypes, such as HPV31, 33, 52, and 58, particularly in Asian populations (23–25). This prospective population-based cohort study of 3,299 women in China addresses this gap by evaluating the 3-year cumulative risks of CIN2+ and CIN3+ stratified by baseline extended HPV genotyping, independent of cytology. Our findings demonstrate a distinct risk hierarchy, with HPV33 and HPV58 exhibiting risks comparable to HPV18, thereby supporting the integration of extended genotyping (HPV16/18/33/52/58) into risk-based triage to optimize screening efficiency in high-burden regions.
The 3-year absolute risks of CIN2+ were highest for HPV16 (32.81%), followed by HPV18 (28.21%), HPV33 (26.09%), and HPV58 (25.00%), with relative risks exceeding 96-fold compared to HR-HPV-negative women. This oncogenic hierarchy, where HPV33 and HPV58 rival HPV18, likely stems from genotype-specific biological factors, including higher persistence rates and enhanced E6/E7 oncoprotein activity in alpha-9/7 species, promoting transformation in host genetic backgrounds (5, 19, 20). In rural Chinese settings, cofactors like smoking may exacerbate clearance failure, as evidenced by prevalence data linking HPV58 to 15-20% of CIN2+ in high-exposure groups (17). These observations align with a recent Chinese cohort, which confirmed that HPV58 predominated in high-grade lesions among TCT-positive women, indicating shared pathways in progression (22). Conversely, Western studies like ATHENA report HPV16/18 dominating >70% of CIN3+ cases, with minimal HPV58 contribution (<5%), attributable to differences in host genetics, cofactor exposures, or viral variants (9). Our findings align closely with national and multicenter Chinese data (17) and global estimates for China (3), supporting the broader applicability of these genotype-specific risks across mainland China while acknowledging potential regional variations due to socioeconomic or environmental factors. These disparities underscore the application of extended genotyping in diverse scenarios, enabling tailored triage to reduce under-detection in Asia; future studies should incorporate persistence to refine thresholds.
Extending this stratification, baseline prevalences (HPV58: 3.3%, 27 CIN2+ cases; HPV52: 4.2%, 22 CIN2+ cases) and differential risks (HPV52: 15.94% vs. HPV58: 25.00%) highlight subtype-specific contributions, potentially amplified by co-infections that may increase progression risk through prolonged infection duration and higher viral loads, reflecting varying integration efficiencies (18). Consequently, HPV16/18 genotyping alone yielded modest sensitivities (51.0% for CIN2+, 53.3% for CIN3+), but adding HPV33/52/58 improved to 55.1% and 60.0%, respectively, with specificity >93% and enhanced PPV (20.30% for CIN2+), optimizing triage in resource-strained programs. A study of Yunnan Province complements this by linking HPV33 to E6/E7 mRNA expression in biopsies, a marker of active carcinogenesis, advocating hybrid cytology-genotyping models (21). However, another analysis in Sichuan revealed higher HPV52 burdens in unscreened groups, indicating access disparities that could affect outcomes (26). Thus, extended genotyping optimizes algorithms by reducing unnecessary colposcopies (potentially by 20-30%) (27), addressing resource strain in China’s rural programs, particularly in self-sampling contexts where cytology uptake varies.
From a public health perspective, our results amid China’s low vaccine coverage (28, 29) highlight the rising relevance of non-HPV16/18 high-risk types (HPV52/58/33 at 8.1% prevalence, 54 CIN2+ cases), which may be further amplified by potential type replacement effects post-vaccination, such as increased circulation of non-vaccine types like HPV52/58 observed in cross-sectional studies following vaccine introduction. Integrating extended genotyping with China’s expanding vaccination programs, could enable real-time monitoring of vaccine impact, refine risk-stratified screening intervals for vaccinated women, and mitigate resurgence in high-burden areas, thereby supporting WHO’s 90-70–90 targets (3, 4) through adaptive, evidence-based strategies. The lower HPV52 risk relative to HPV58 suggests tailored monitoring intervals, enabling sustainable screening in high-burden areas like Henan. This is corroborated by a 2025 survey of 24,588 rural women, where HR-HPV genotyping guided vaccination integration to mitigate disparities (30). Integrating extended genotyping into guidelines could enhance equity and early intervention, especially in resource-limited settings; longitudinal epidemiological studies should track post-vaccination dynamics to prevent resurgence and inform adaptive strategies.
This study’s strengths include prospective design, large sample size, blinded assessments, and >80% follow-up retention, yielding robust risk estimates aligned with real-world Chinese screening. The cohort’s genotype distribution mirrors national patterns, enhancing generalizability, while CIN2+ as the endpoint ensures clinical relevance. The study also has several limitations. First, the single-center design may overlook regional variations. Second, the lack of genotype persistence data risks overestimating risks from transient infections, however, which will be incorporated in subsequent analysis. Furthermore, the 18.1% loss to follow-up rate may introduce selection bias. However, the lack of differences in baseline characteristics between completers and non-completers supports the robustness of our risk estimates. Future work should extend follow-up, establish a dynamic cohort, and expand the study regions to provide more robust evidence.
In conclusion, this study provides longitudinal evidence of genotype-specific risks in Chinese women, advocating extended HPV genotyping for refined screening algorithms and accelerated elimination efforts in evolving epidemiological contexts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Viveros-Carreño D Fernandes A Pareja R . Updates on cervical cancer prevention. Int J Gynecol Cancer. (2023) 33:394–402. doi: 10.1136/ijgc-2022-003703, PMID: 36878567 · doi ↗ · pubmed ↗
- 2Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I . Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834, PMID: 38572751 · doi ↗ · pubmed ↗
- 3Han B Zheng R Zeng H Wang S Sun K Chen R . Cancer incidence and mortality in China, 2022. J Natl Cancer Inst. (2024) 4:47–53. doi: 10.1016/j.jncc.2024.01.006, PMID: 39036382 PMC 11256708 · doi ↗ · pubmed ↗
- 4World Health Organization . Global strategy to accelerate the elimination of cervical cancer as a public health problem (2020). Available online at: https://www.who.int/publications/i/item/9789240014107 (Accessed November 17, 2020).
- 5World Health Organization . WHO guideline for screening and treatment of cervical pre-cancer lesions for cervical cancer prevention (2021). Available online at: https://www.who.int/publications/i/item/9789240030824 (Accessed July 6, 2021). 34314129 · pubmed ↗
- 6Zhang M Bao HL Wang LM Zhao ZP Huang ZJ Zhang X . Analysis of cervical cancer screening and related factors in China. Zhonghua Yi Xue Za Zhi. (2021) 101:1869–74. doi: 10.3760/cma.j.cn 112137-20210108-00054, PMID: 34192843 · doi ↗ · pubmed ↗
- 7Zhao YX Ma L Ren WH Song B Wang LH Di JL . Analysis of the reported data of National Cervical Cancer Screening Program in Rural Areas in China from 2009 to 2018. Zhonghua Yi Xue Za Zhi. (2021) 101:1863–8. doi: 10.3760/cma.j.cn 112137-20210111-00075, PMID: 34192844 · doi ↗ · pubmed ↗
- 8Ciavattini A Carpini GD Giannella L Arbyn M Kyrgiou M Joura EA . European Federation for Colposcopy (EFC) and European Society of Gynaecological Oncology (ESGO) joint considerations about human papillomavirus (HPV) vaccination, screening programs, colposcopy, and surgery during and after the COVID-19 pandemic. Int J Gynecol Cancer. (2020) 30:1097–100. doi: 10.1136/ijgc-2020-001617, PMID: 32487685 PMC 7418593 · doi ↗ · pubmed ↗