Demographic/clinicopathological characteristics and prognosis of resectable Epstein-Barr virus-associated gastric cancer: a nested case-control study from an Eastern China
Lihu Gu, Qiufeng Zhang, Yuying Hu, Zhiyi Xiang, Shengqiang Ji, Weiming Yu, Xingchen Liu, Ping Chen, Feng Wu, Qi Zheng

TL;DR
This study examines the characteristics and outcomes of a specific type of stomach cancer linked to the Epstein-Barr virus in patients from Eastern China.
Contribution
The study provides new insights into the clinicopathological features and prognosis of resectable EBV-associated gastric cancer through a nested case-control design.
Findings
EBVaGC patients were predominantly male and had more undifferentiated tumors.
Elevated CEA levels and pTNM stage III were independent risk factors for survival outcomes in EBVaGC patients.
EBVaGC showed a trend toward better disease-free survival compared to EBV-negative gastric cancer, though not statistically significant.
Abstract
Epstein-Barr virus-associated gastric cancer (EBVaGC) represents a distinct molecular subtype of gastric cancer (GC). This multicenter study aimed to investigate the clinicopathological characteristics and prognosis of resectable EBVaGC patients. Data were prospectively collected and retrospectively analyzed from 1,400 patients at Ningbo No. 2 Hospital from January 2014 to December 2023 and 55 EBVaGC patients were identified. Additionally, 95 EBVaGC patients from two external cooperative centers were included. A 1:4 propensity score matching (PSM) analysis was performed between EBVaGC patients and EBV-negative gastric cancer (EBVnGC) patients. Median follow-up duration was 34 months. Among the 150 EBVaGC patients, the median age was 64, and 88.7% were male. Undifferentiated tumors were more common. During the follow-up, 121 EBVaGC patients did not experience recurrence. After PSM,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
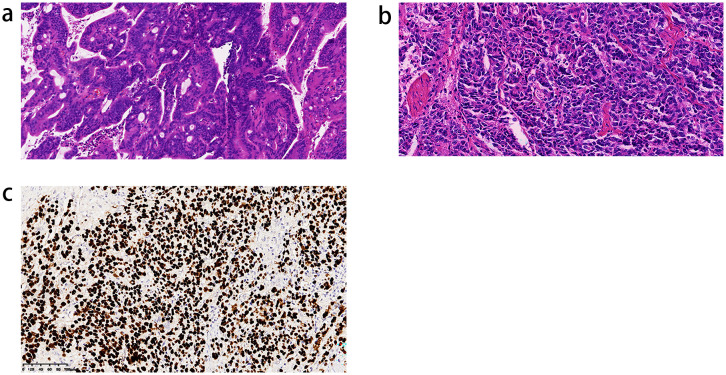 Figure 1
Figure 1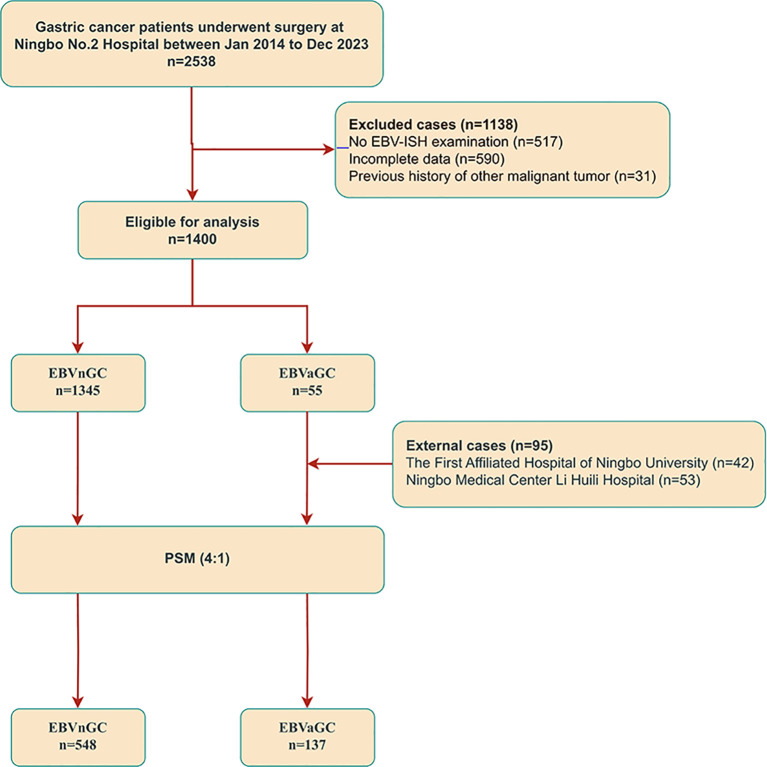 Figure 2
Figure 2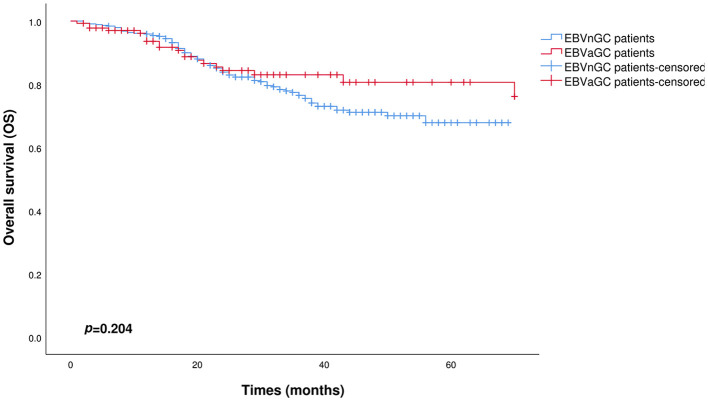 Figure 3
Figure 3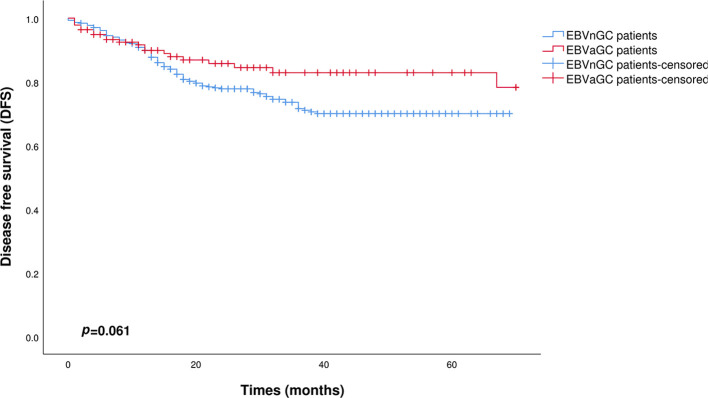 Figure 4
Figure 4| Clinical features | N=150 |
|---|---|
| Age (years) (mean ± SD) | 64.3 ± 9.1 |
| Gender | |
| Male | 133 (88.7%) |
| Female | 17 (11.3%) |
| BMI (kg/m2) (mean ± SD) | 22.6 ± 3.0 |
| Comorbidity | |
| Absence | 24 (16.0%) |
| Presence | 73 (48.7%) |
| NA | 53 (35.3%) |
| CEA (ng/mL) | |
| ≤5 | 93 (62.0%) |
| >5 | 8 (5.3%) |
| NA | 49 (32.7%) |
| Tumor location | |
| Upper third | 44 (25.0%) |
| Middle third | 51 (34.0%) |
| Lower third | 45 (30.0%) |
| At least two-thirds | 10 (6.7%) |
| Surgical type | |
| Proximal stomach | 3 (2.0%) |
| Distal stomach | 54 (36.0%) |
| Remnant stomach | 4 (2.7%) |
| Total stomach | 89 (59.3%) |
| Postoperative chemotherapy | |
| Absence | 50 (33.3%) |
| Presence | 100 (66.7%) |
| N=150 | |
|---|---|
| Differentiation | |
| Differentiated | 51 (34.0%) |
| Undifferentiated | 99 (66.0%) |
| Tumor size (cm) | |
| ≤5 | 110 (73.3%) |
| >5 | 40 (26.7%) |
| Perineural invasion | |
| Absence | 76 (50.7%) |
| Presence | 74 (49.3%) |
| Lymphovascular invasion | |
| Absence | 68 (45.3%) |
| Presence | 82 (54.7%) |
| pT category | |
| T1 | 32 (21.3%) |
| T2 | 27 (18.0%) |
| T3 | 30 (20.0%) |
| T4a | 55 (36.7%) |
| T4b | 6 (4.0%) |
| pN category | |
| N0 | 71 (47.3%) |
| N1 | 28 (18.7%) |
| N2 | 20 (13.3%) |
| N3a | 27 (18.0%) |
| N3b | 4 (2.7%) |
| pTNM | |
| 1a | 29 (19.3%) |
| 1b | 22 (14.7%) |
| 2a | 21 (14.0%) |
| 2b | 14 (9.3%) |
| 3a | 33 (22.0%) |
| 3b | 24 (16.0%) |
| 3c | 7 (4.7%) |
| HER-2 | |
| Negative | 125 (83.3%) |
| Positive | 3 (2.0%) |
| 2+ | 22 (14.7%) |
| MMR | |
| pMMR | 124 (82.7%) |
| dMMR | 2 (1.3%) |
| NA | 24 (16.0%) |
| Number of lymph node dissection (median, IQR) | 26 (20-33) |
| Prognostic parameters | N=150 |
|---|---|
| Postoperative recurrence | |
| Absence | 121 (80.7%) |
| Presence | 23 (15.3%) |
| NA | 6 (4.9%) |
| Number of patients surviving | 121 (80.7%) |
| Follow-up period (median, IQR) | 33.82 (13-42) |
| Clinicopathological features | OS | DFS | ||||
|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | |
| Age (years) | ||||||
| ≤60 | 1 | 1 | ||||
| >60 | 4.02 | 0.83-19.55 | 0.085 | 3.28 | 0.74-14.61 | 0.120 |
| CEA (ng/mL) | ||||||
| ≤5 | 1 | 1 | ||||
| >5 | 8.11 | 1.30-50.44 | 0.025 | 6.23 | 1.14-33.99 | 0.035 |
| pTNM | ||||||
| I/II | 1 | 1 | ||||
| III | 19.57 | 2.18-175.42 | 0.008 | 18.51 | 2.19-156.77 | 0.007 |
| Clinicopathological feature | EBVnGC patients N=548 | EBVaGC patients N=137 | P |
|---|---|---|---|
| Age (years) | |||
| ≤60 | 188 (34.3%) | 49 (35.8%) | |
| >60 | 360 (65.7%) | 88 (64.2%) | 0.748 |
| Gender | |||
| Male | 490 (89.4%) | 122 (89.1%) | |
| Female | 58 (10.6%) | 15 (10.9%) | 0.901 |
| BMI (kg/m2) | |||
| <18.5 | 42 (7.7%) | 10 (7.3%) | |
| 18.5-23.9 | 329 (60.0%) | 87 (63.5%) | |
| ≥24 | 177 (32.3%) | 40 (29.2%) | 0.752 |
| Comorbidity | |||
| Absence | 17 (3.1%) | 23 (16.8%) | |
| Presence | 295 (53.8%) | 68 (49.6%) | |
| NA | 236 (43.1%) | 46 (33.6%) | <0.001 |
| Surgical type | |||
| Proximal stomach | 7 (1.3%) | 3 (2.2%) | |
| Distal stomach | 369 (67.3%) | 53 (38.7%) | |
| Remnant stomach | 0 (0) | 4 (2.9%) | |
| Total stomach | 172 (31.4%) | 77 (56.2%) | <0.001 |
| Tumor location | |||
| Upper third | 85 (15.5%) | 36 (26.3%) | |
| Middle third | 124 (22.6%) | 47 (34.3%) | |
| Lower third | 328 (59.9%) | 44 (32.1%) | |
| At least two-thirds | 11 (2.0%) | 10 (7.3%) | <0.001 |
| Tumor size (cm) | |||
| ≤5 | 408 (74.5%) | 99 (72.3%) | |
| >5 | 140 (25.5%) | 38 (27.7%) | 0.601 |
| Differentiation | |||
| Differentiated | 297 (54.2%) | 46 (33.6%) | |
| Undifferentiated | 251 (45.8%) | 91 (66.4%) | <0.001 |
| Perineural invasion | |||
| Absence | 295 (53.8%) | 69 (50.4%) | |
| Presence | 253 (46.2%) | 68 (49.6%) | 0.467 |
| Lymphovascular invasion | |||
| Absence | 257 (46.9%) | 63 (46.0%) | |
| Presence | 291 (53.1%) | 74 (54.0%) | 0.848 |
| pT category | |||
| T1 | 147 (26.8%) | 30 (21.9%) | |
| T2 | 107 (19.5%) | 26 (19.0%) | |
| T3 | 103 (18.8%) | 25 (18.2%) | |
| T4a | 166 (30.3%) | 50 (36.5%) | |
| T4b | 25 (4.6%) | 6 (4.4%) | 0.661 |
| pN category | |||
| N0 | 290 (52.9%) | 66 (48.2%) | |
| N1 | 91 (16.6%) | 26 (19.0%) | |
| N2 | 69 (12.6%) | 17 (12.4%) | |
| N3a | 83 (15.1%) | 24 (17.5%) | |
| N3b | 15 (2.7%) | 4 (2.9%) | 0.870 |
| pTNM | |||
| 1a | 126 (23.0%) | 27 (19.7%) | |
| 1b | 87 (15.9%) | 21 (15.3%) | |
| 2a | 76 (13.9%) | 19 (13.9%) | |
| 2b | 62 (11.3%) | 13 (9.5%) | |
| 3a | 94 (17.2%) | 29 (21.2%) | |
| 3b | 82 (15.0%) | 21 (15.3%) | |
| 3c | 21 (3.8%) | 7 (5.1%) | 0.889 |
| Number of lymph node dissection (median, IQR) | 24 (19-31) | 25 (20-33) | 0.227 |
| HER-2 | |||
| Negative | 408 (74.5%) | 116 (84.7%) | |
| Positive | 47 (8.6%) | 3 (2.2%) | |
| 2+ | 93 (17.0%) | 18 (13.1%) | 0.013 |
| CEA (ng/mL) | |||
| ≤5 | 450 (82.1%) | 87 (63.5%) | |
| >5 | 70 (12.8%) | 8 (5.8%) | |
| NA | 28 (5.1%) | 42 (30.7%) | 0.175 |
| Postoperative chemotherapy | |||
| Absence | 217 (39.6%) | 48 (35.0%) | |
| Presence | 331 (60.4%) | 89 (65.0%) | 0.327 |
| Clinicopathological features | OS | DFS | ||||
|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | |
| Age (years) | ||||||
| ≤60 | 1 | 1 | ||||
| >60 | 1.95 | 1.22-3.13 | 0.006 | 1.57 | 1.03-2.39 | 0.037 |
| EBV-ISH | ||||||
| negative | 1 | 1 | ||||
| positive | 0.56 | 0.29-1.09 | 0.085 | 0.49 | 0.26-0.93 | 0.028 |
| CEA (ng/mL) | ||||||
| ≤5 | 1 | 1 | ||||
| >5 | 1.64 | 1.03-2.61 | 0.039 | 1.65 | 1.07-2.56 | 0.025 |
| Perineural invasion | ||||||
| Absence | 1 | |||||
| Presence | 1.68 | 1.01-2.77 | 0.044 | 1.56 | 0.99-2.48 | 0.058 |
| pTNM | ||||||
| I | 1 | 1 | ||||
| II | 2.51 | 1.01-6.27 | 0.048 | 3.52 | 1.39-8.95 | 0.008 |
| III | 6.34 | 2.67-15.06 | <0.001 | 9.35 | 3.87-22.59 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral-associated cancers and disorders · Gastric Cancer Management and Outcomes · Helicobacter pylori-related gastroenterology studies
Introduction
Gastric cancer (GC) remains a major global health burden, ranking fifth in cancer incidence and mortality. Data from a study published in 2024 indicated over 968,000 new cases and nearly 660,000 fatalities from GC (1). In a seminal study conducted in 1993, Tokunaga and associates utilized in situ hybridization (ISH) technology to confirm the presence of Epstein-Barr virus-encoded small RNAs (EBERs) in GC cells (2). In 2014, The Cancer Genome Atlas (TCGA) classified GC into four distinct subtypes based on molecular profiles: microsatellite instability (MSI), genomic stability (GS), chromosomal instability (CIN), and EBV-associated gastric cancer (EBVaGC) (3).
EBVaGC is one of the predominant subgroups among EBV-associated tumors. The proportion of EBVaGC among all GC cases varies significantly across geographic regions, with reported rates ranging from 1.3% to 20.1% (4–7). This subtype is characterized by clonal expansion of EBV-infected cells. It exhibits distinct molecular features such as phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA) mutations, hypermethylation of DNA, and overexpression of programmed cell death ligand 1 (PD-L1) and programmed cell death ligand 2 (PD-L2), suggesting that EBV infection contributes to the malignant transformation of normal cells in gastric carcinogenesis (3, 8). Studies have revealed a higher incidence of EBVaGC in males than females, with a predilection for the proximal stomach or the proximal part of the residual stomach post-surgery (9). Notably, EBVaGC is associated with a relatively low rate of lymph node metastasis and a more favorable prognosis following surgical resection (10). Furthermore, patients with EBVaGC demonstrate a positive response to immune checkpoint inhibitors, highlighting its potential as a target for therapeutic interventions and a valuable biomarker (11).
While the unique aspects of EBVaGC are receiving increased recognition, there remains ongoing debate concerning its epidemiological features and prognostic implications. Geographical variations exist in the prevalence of EBVaGC across different regions (5, 12). More importantly, whether EBVaGC confers a more favorable prognosis compared to EBV-negative gastric cancer (EBVnGC) remains inconclusive, and the potential clinicopathological determinants influencing its prognosis warrant systematic elucidation (5, 6). It is worth noting that most research in this area is hampered by limitations such as small sample sizes and other potential sources of bias. To overcome these gaps, this case-control study collected data from patients with resectable GC across multiple Chinese medical institutions, aiming to thoroughly investigate the clinical characteristics of EBVaGC patients who underwent radical gastrectomy and to explore their prognosis.
Methods
Patients
The following inclusion criteria determined the eligibility of this study: 1) histopathologically confirmed primary gastric adenocarcinoma; 2) no history of other malignant tumors; 3) availability of comprehensive clinical and pathological data. Additionally, patients who underwent radical surgery were included in the final analysis. Based on these criteria, this study identified 1,400 GC patients who underwent surgical treatment at Ningbo No. 2 Hospital from January 2014 to December 2023, of which 55 were diagnosed with EBVaGC through ISH. Simultaneously, 95 EBVaGC patients diagnosed with ISH from the First Affiliated Hospital of Ningbo University and Ningbo Medical Center Li Huili Hospital were enrolled within the same time frame under identical criteria. Clinical data were prospectively collected and subsequently analyzed retrospectively. Specimen collection and utilization were approved by the Ethics Committee of Ningbo No. 2 Hospital (Ethics Approval Number: PJ-NBEY-KY-2019-153-01). The study was conducted according to the ethical standards of all participating institutions, and written informed consent was obtained from patients through signed consent forms.
EBV ISH examination
ISH is recognized as the gold standard for diagnosing EBVaGC in GC tissues. When tumor cells in gastric specimens treated by surgery show positive results for EBV-ISH, the diagnostic criteria for EBVaGC are designated as “EBV positive”. The EBV-ISH procedure uses EBER probes, detection kits, ISH protease, and staining solution. Formalin-fixed paraffin-embedded (FFPE) tissue sections were cut into 3 μm slices after dewaxing and pretreated with ISH protease. Hybridization and visualization were performed using fluorescently labeled probes and detection kits and restaining with a staining solution. For EBV-ISH, representative FFPE tissue sections that best reflected the overall histopathological characteristics of each GC case were selected. Three pathologists independently evaluated ISH results. Figures 1a, b show the pathological images of EBVnGC and EBVaGC. Representative staining of a case of EBVaGC by ISH is shown in Figure 1c, demonstrating specific nuclear positivity for EBER.
Pathological sections demonstrating differences between EBVnGC and EBVaGC patients ((a) EBVnGC group, (b) EBVaGC group, (c) EBER-ISH staining EBVaGC).
Clinical and pathological data
Prospective clinical data related to patient characteristics were collected, including basic demographic data (age, sex, body mass index (BMI), comorbidities) and cancer-related information (tumor location, carcinoembryonic antigen (CEA) levels, type of gastrectomy, and postoperative treatment). Additionally, pathological features included degree of differentiation, tumor size, perineural invasion, lymphovascular invasion, pathological tumor-node-metastasis (pTNM) staging, number of lymph nodes dissected, and expression levels of human epidermal growth factor receptor 2 (HER-2) and mismatch repair proteins (MMR). Pathological staging was performed according to the American Joint Committee on Cancer (AJCC) Staging Classification for Gastric Cancer (8th edition, 2016).
Follow-up
This study utilized information from outpatient and inpatient records, as well as physical examination, imaging, endoscopy, and laboratory test results obtained via telephone, text messages, and social media platforms, to systematically monitor the disease status of patients. In the first two years following surgery, follow-up intervals were set at every 3–6 months, followed by annual check-ups thereafter. Patients lost to follow-up were designated as censored patients, and the date of the last known contact was recorded. Overall survival (OS) was described as the time from the date of surgery to death from any cause. Disease-free survival (DFS) was defined as the duration from surgery to the first occurrence of local recurrence, distant metastasis. All patients participating in this study were followed up until December 2024.
Statistical analysis
Statistical analysis was performed using SPSS 25.0. To reduce bias, propensity score matching (PSM) was performed between the EBVaGC and EBVnGC groups at a ratio of 1:4, with a caliper width of 0.02. Variables included in PSM were age, sex, BMI, tumor size, CEA level, perineural and lymphovascular invasion, pTNM stage, number of lymph nodes dissected, and postoperative chemotherapy. For normally distributed data, continuous variables were presented as mean ± standard deviation (SD), and for data that did not conform to a normal distribution, the median with interquartile range (IQR) was presented, with data comparison applying independent samples t-test or Wilcoxon rank-sum test. Categorical variables were expressed as frequency and percentage, and their data comparison was analyzed using Pearson’s chi-square test or Fisher’s exact test according to expected frequency. The Cox proportional hazards model was used for univariate and multivariate analysis of OS and DFS, with results presented as hazard ratio (HR) and 95% confidence interval (CI). Univariate analysis was conducted first for all potential prognostic factors. Variables with a P< 0.05 or those considered to have clinically relevant and potentially important associations with prognosis were then selected for multivariate analysis. Survival curves were plotted using the Kaplan-Meier method and compared using the log-rank test. All statistical tests were two-sided, with p < 0.05 considered statistically significant.
Results
Study population
From January 2014 to December 2023, a total of 2,538 patients underwent gastrectomy at Ningbo No. 2 Hospital. Based on the inclusion criteria, 1,138 patients were excluded, including 517 without EBV-ISH examination, 590 with incomplete data, and 31 with a history of other malignant tumors. Ultimately, 1,400 patients met the analysis criteria. Among them, 55 cases of EBVaGC were detected through ISH examination. In addition, this study included 42 patients from the First Affiliated Hospital of Ningbo University and 53 patients from Ningbo Medical Center Li Huili Hospital who were confirmed with EBVaGC through ISH. A total of 150 patients with EBVaGC from Eastern China were enrolled in this study. After excluding 13 patients who did not undergo radical surgery, a four-to-one match was conducted, including 685 patients, of which 548 were EBVnGC patients, and 137 were EBVaGC patients. For more details, see Figure 2.
Flowchart detailing the selection process for the study participants.
Clinical and pathological characteristics of EBVaGC patients
The baseline clinical characteristics of the 150 EBVaGC patients from Eastern China are shown in Table 1. The average age of the patients was 64 years, with an average BMI of 22.6. Male patients accounted for 88.7%, and female patients accounted for 11.3%. The 48.7% had comorbidities, including hypertension, coronary heart disease, diabetes, etc. Among all patients, 5.3% had a serum CEA level higher than 5 ng/mL. In terms of tumor location, 34% were located in the middle third of the stomach, 30% in the lower third, and 25% in the upper third. The most common type of gastrectomy was total gastrectomy (59.3%), followed by distal gastrectomy (36%) and proximal gastrectomy (2%). The 66.7% of patients received postoperative chemotherapy.
Table 2 describes the pathological characteristics of the 150 EBVaGC patients from Eastern China in detail. Undifferentiated tumors accounted for 66%, and differentiated tumors accounted for 34%. In terms of HER-2 expression, most patients were HER-2 negative (83.3%), and only 2% were HER-2 positive. Patients with mismatch repair-proficient (pMMR) accounted for 82.7%, those with mismatch repair-deficient (dMMR) accounted for 1.3%, and the MMR status of the remaining 16% was not clear. Patients with a maximum tumor diameter of ≤5 cm accounted for 73.3%. Perineural invasion was present in 49.3%, and lymphatic invasion in 54.7%. In the pTNM, stage I accounted for 34%, stage II for 23.3%, and stage III for 42.7%. The median number of lymph nodes dissected was 25.5. The median follow-up time in the queue was 34 months.
Prognosis of EBVaGC patients
Table 3 describes the prognosis of the 150 EBVaGC patients from Eastern China. In terms of postoperative recurrence, by the end of the follow-up period, most patients (80.7%) did not experience recurrence, 15.3% had recurrence, and the recurrence data for the remaining patients were missing. During the observation period, 80.7% of the patients remained alive.
Factors affecting the prognosis of EBVaGC patients
Supplementary Table 1 shows the results of Cox univariate analysis for OS in 137 EBVaGC patients, indicating that tumor location, lymphovascular invasion, and pTNM stage were potentially associated with OS. Supplementary Table 2 shows the results of Cox univariate analysis for DFS in 137 EBVaGC patients, indicating that tumor location, tumor size, lymphovascular invasion, and pTNM stage were potentially associated with DFS. In Table 4, further Cox multivariate analysis revealed that elevated CEA levels and pTNM stage III were independent risk factors for OS and DFS in EBVaGC patients. Although age showed a certain risk trend, it did not reach statistical significance.
PSM analysis
Through 4-to-1 PSM, no significant differences were found between the EBVnGC group (548 patients) and the EBVaGC group (137 patients) in terms of age, gender, BMI, tumor size, perineural invasion, lymphatic invasion, pTNM category, number of lymph nodes dissected, and postoperative chemotherapy (Table 5). There were significant differences in the types of surgeries received between the two groups of patients. Among the EBVnGC patients, 67.3% underwent distal gastrectomy, and 31.4% underwent total gastrectomy. In contrast, among the EBVaGC patients, 38.7% underwent distal gastrectomy, and 56.2% underwent total gastrectomy. More than half of the EBVnGC patients had differentiated tumors, whereas only 33.6% of the EBVaGC patients had differentiated tumors. Additionally, there were significant differences in the HER-2 status between the two groups. Among the EBVnGC patients, 74.5% were HER-2 negative, and 8.6% (47 out of 548) were HER-2 positive. In comparison, among the EBVaGC patients, 84.7% were HER-2 negative and 2.2% were HER-2 positive.
Figures 3 and 4 show the Kaplan–Meier curves for OS and DFS, respectively, between the EBVnGC group and the EBVaGC group after PSM processing. In this study, there was no significant difference in OS between the two groups (p=0.204). The DFS was better in the EBVaGC group compared to the EBVnGC group, but the difference did not reach statistical significance (p=0.061).
Kaplan-Meier survival curves comparing OS between EBVaGC and EBVnGC patients after PSM (p=0.204).
Kaplan-Meier survival curves comparing DFS between EBVaGC and EBVnGC patients after PSM (p=0.061).
In the long-term prognosis of gastric cancer, both OS and DFS are influenced by various factors. The results show that advanced age, higher pTNM stage, and elevated CEA levels are independent risk factors, while EBV infection acts as a protective factor. For more details, see Table 6.
Discussion
This study conducted a detailed analysis of the clinicopathological characteristics and prognosis of patients with resectable EBVaGC. For patients with EBVaGC who underwent radical surgery, a survival comparison was made with patients with EBVnGC after propensity score matching (PSM). The results showed that EBVaGC accounts for approximately 4% of all gastric adenocarcinoma. The average age of EBVaGC patients was 64. Among 150 patients with EBVaGC, 88.7% were male, reflecting a male predominance within this subgroup. These characteristics are similar to those reported in other regions of China and in international studies (4, 13, 14). As shown in Table 5, among the PSM-matched gastric cancer patients, a similar gender distribution was observed between patients with EBVnGC and EBVaGC, and no significant difference was found between the two groups. This may be due to the higher likelihood of male being exposed to risk factors such as smoking, alcohol consumption, and high-salt diets. A study from Japan showed that salt intake and occupational exposure may damage the gastric mucosa, increasing the risk of EBV infection (15). Additionally, gender differences in sex hormones and immune regulation may be factors. One research suggested that male sex hormones, such as testosterone, may suppress immune responses, while estrogen provides stronger immune control against EBV (16). Most EBVaGC patients were HER-2 negative. This suggests that EBV infection may inhibit differentiation and interfere with HER-2 expression through specific molecular pathways such as Latent Membrane Protein 1/2A (LMP1/2A)-mediated oncogenic signaling (3).
In the EBVaGC patients from Eastern China discussed in this study, tumors were predominantly located in the middle stomach. This distribution is likely attributable to the combined effects of EBV infection mechanisms, local immune responses, chronic inflammatory microenvironments, and molecular epigenetic features. The mucosa of the gastric body and cardia may recruit a large number of nonspecific lymphocytes through cytokines in the context of chronic inflammation, creating an immunosuppressive microenvironment conducive to EBV infection and tumor development (17). Meanwhile, EBV-driven DNA hypermethylation may affect the differentiation regulation of stem cells in the gastric body and cardia, leading to malignant transformation (18). Moreover, BamHI-A rightward transcript (BART) miRNAs encoded by EBV can promote tumor cell survival by inhibiting host tumor suppressor genes, and specific cell types in the middle stomach may be more sensitive to these miRNAs (17). Histologically, EBVaGC can be divided into three subtypes and lymphoepithelioma-like carcinoma (LELC) is more common. LELC often manifests as undifferentiated carcinoma with dense lymphocytic infiltration, resembling nasopharyngeal carcinoma (NPC) (19). This finding was confirmed in our study. Additionally, more than 80% of LELC cases have been reported to be EBV-positive (20).
It is generally believed that EBVaGC is associated with a better prognosis. In this study, the postoperative recurrence rate was 15.3%. Cox regression analysis showed that pTNM stage III is an independent risk factor for OS and DFS in EBVaGC patients. This indicates that the stage of pTNM has an important prognostic value for patients. CEA is an acidic glycoprotein with embryonic antigen characteristics that can enhance tumor invasiveness through its adhesion, immune suppression, and protease inhibition functions. Li et al. found that serum CEA levels in EBVaGC patients are lower than normal values, but no correlation was found between CEA levels and long-term prognosis (21). Further analysis in our study revealed that elevated CEA levels were an independent risk factor for OS and DFS in EBVaGC patients, suggesting that CEA may serve as a prognostic biomarker. After PSM analysis, no significant difference in OS was found between the EBVaGC and EBVnGC groups, but the DFS was better in the EBVaGC group. This result may be influenced by the limited sample size, insufficient follow-up duration, and other confounding factors.
The exact mechanisms by which EBV affects the prognosis of EBVaGC patients remain unclear, but it is widely acknowledged that its protective effects are closely related to immune factors. EBVaGC patients have a unique immune microenvironment, with more immune-active cells infiltrating the tumor microenvironment, such as CD8+ cytotoxic T cells and mature dendritic cells, forming an immune-activated phenotype (22, 23). This active immune environment may enhance immune surveillance and inhibit tumor progression, thereby providing a certain protective effect. Accordingly, the antitumor immune response is also enhanced in EBVaGC patients. Studies found a higher proportion of tumor-infiltrating lymphocytes (TILs) and significant increases in CD8+ T cells and cytotoxic T lymphocytes (CTLs) infiltration in these patients (24–26). These cells may inhibit tumor progression by directly killing tumor cells or modulating immune responses. Additionally, virus antigen-driven immune recognition may also play an important role. Viral proteins expressed during EBV latency, such as EBNA1 and LMP2A, can act as tumor-specific antigens to activate T cells and natural killer (NK) cells, forming continuous immune surveillance (27, 28). EBV infection also promotes an inflammatory response in GC tissues, which is closely related to interferon-γ-mediated signaling pathways and adaptive immune responses (29). Inflammatory responses are generally considered an important component of antitumor immunity, and thus, EBV infection may also indirectly inhibit tumor progression through this mechanism.
EBVaGC patients also exhibit unique genetic and molecular expression profiles that may inhibit tumor malignancy and reduce distant metastasis through epigenetic modifications and signaling pathway regulation. A significant feature of EBVaGC is genome-wide hypermethylation, which can lead to the silencing of tumor suppressor genes but may also suppress the expression of pro-metastatic genes (3, 30). For example, the promoter regions of genes such as PIK3CA and cyclin-dependent kinase inhibitor 2A (CDKN2A) show high levels of methylation in EBVaGC, which not only affects the expression of these genes but may also reduce metastatic potential by inhibiting tumor stemness. Studies found that high-frequency mutations in PIK3CA and activation of the Wnt pathway in EBVaGC promote clonal expansion, but hypermethylation may limit the overly invasive phenotype (31, 32). One research indicated that EBV infection induces fat mass and obesity-associated gene (FTO) expression through myelocytomatosis oncogene (MYC), inhibiting the translation of m6A-modified metastasis-related genes, thereby reducing lymph node metastasis (33).
The unique immune microenvironment and molecular expression profile of EBVaGC provide distinct advantages and potential for immunotherapy. PD-L1/PD-L2, important markers of tumor immune evasion, are highly expressed in EBVaGC, making them ideal targets for immune checkpoint inhibitor (ICI) therapy. Studies have shown that patients with EBVaGC have a higher overall response rate (ORR) to immunotherapy, with prolonged DFS and OS (34, 35). The special immune microenvironment of EBVaGC provides a “hot tumor” basis for immunotherapy, characterized by significant lymphocyte infiltration and an immune-activated phenotype (23). Specific immunotherapy strategies, such as EBV-specific CD8+ cytotoxic T-cell adoptive therapy, have shown success in nasopharyngeal carcinoma and lymphoma and may further optimize EBVaGC treatment by targeting EBV antigens in the future. In addition, chimeric antigen receptor T-cell (CAR-T) immunotherapy and cancer vaccines have also shown potential applications in the treatment of EBVaGC (36).
This study provides insights into the prognosis of EBVaGC patients from Eastern China through its large sample size and multicenter design. However, limitations such as the retrospective nature of the study, short follow-up duration and lack of data on immunotherapy restrict the comprehensiveness and applicability of the findings.
Conclusion
This research found that EBVaGC patients have a better prognosis compared to those with EBVnGC. EBVaGC exhibits unique clinicopathological features, including a male predominance, a high rate of undifferentiation, a low HER-2 positivity rate, and significant lymphocytic infiltration. Additionally, elevated CEA levels and pTNM stage III classification were identified as independent risk factors for OS and DFS in EBVaGC patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I . Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834, PMID: 38572751 · doi ↗ · pubmed ↗
- 2Tokunaga M Land CE Uemura Y Tokudome T Tanaka S Sato E . Epstein-Barr virus in gastric carcinoma. Am J Pathol. (1993) 143:1250–4. PMC 18871768238241 · pubmed ↗
- 3Cancer Genome Atlas Research Network . Comprehensive molecular characterization of gastric adenocarcinoma. Nature. (2014) 513:202–9. doi: 10.1038/nature 13480, PMID: 25079317 PMC 4170219 · doi ↗ · pubmed ↗
- 4Murphy G Pfeiffer R Camargo MC Rabkin CS . Meta-analysis shows that prevalence of Epstein-Barr virus-positive gastric cancer differs based on sex and anatomic location. Gastroenterology. (2009) 137:824–33. doi: 10.1053/j.gastro.2009.05.001, PMID: 19445939 PMC 3513767 · doi ↗ · pubmed ↗
- 5Camargo MC Kim WH Chiaravalli AM Kim KM Corvalan AH Matsuo K . Improved survival of gastric cancer with tumour Epstein-Barr virus positivity: an international pooled analysis. Gut. (2014) 63:236–43. doi: 10.1136/gutjnl-2013-304531, PMID: 23580779 PMC 4384434 · doi ↗ · pubmed ↗
- 6Li LL Yu AY Zhu M Ma LY Cao MH Liu WL . Clinicopathological characteristics and prognosis of Epstein-Barr virus-associated gastric cancer. Arch Virol. (2024) 169:114. doi: 10.1007/s 00705-024-06033-3, PMID: 38700535 · doi ↗ · pubmed ↗
- 7Tokunaga M Uemura Y Tokudome T Ishidate T Masuda H Okazaki E . Epstein-Barr virus related gastric cancer in Japan: a molecular patho-epidemiological study. Acta pathologica japonica. (1993) 43:574–81. doi: 10.1111/j.1440-1827.1993.tb 03233.x, PMID: 8291445 · doi ↗ · pubmed ↗
- 8Kaneda A Matsusaka K Aburatani H Fukayama M . Epstein-Barr virus infection as an epigenetic driver of tumorigenesis. Cancer Res. (2012) 72:3445–50. doi: 10.1158/0008-5472.CAN-11-3919, PMID: 22761333 · doi ↗ · pubmed ↗