Esophagopleural fistula and candidiasis: endoscopic stent management after steroid-induced perforation
Yali Chen, Ping Lei, Hui Guo, Shengzhi Teng, Xin Zhou, Zhining Fan, Zhonghua Jiang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
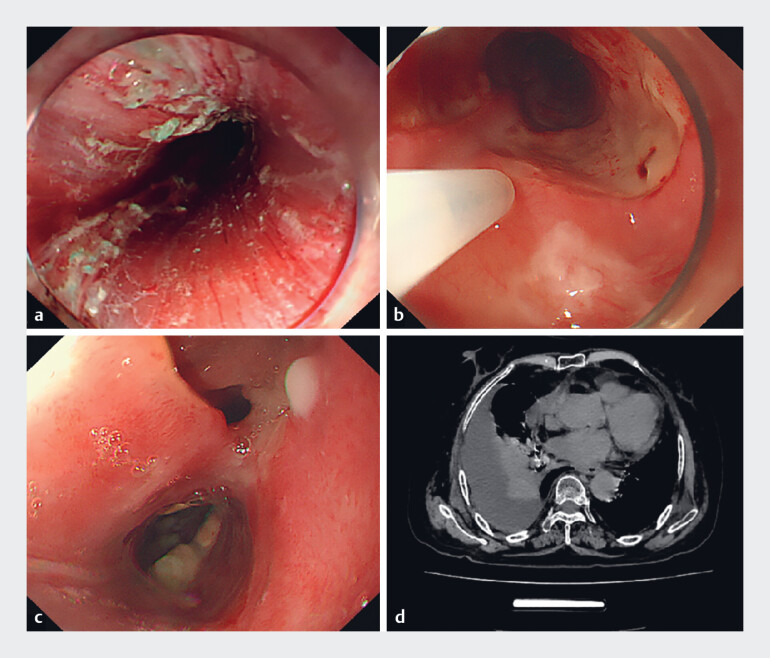 Fig. 1
Fig. 1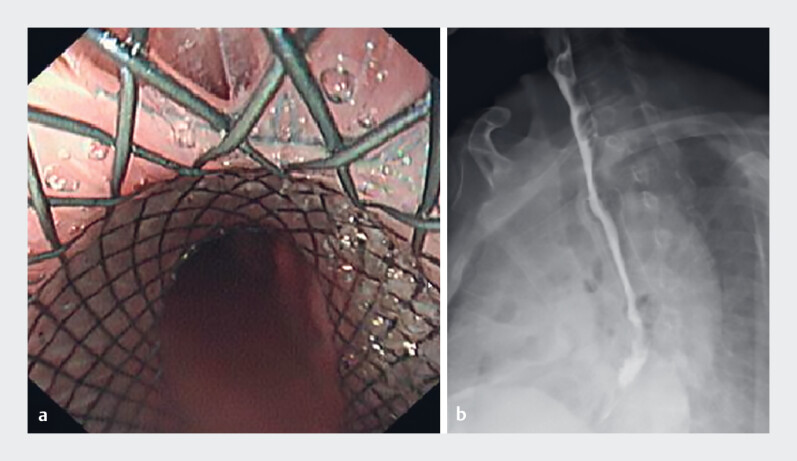 Fig. 2
Fig. 2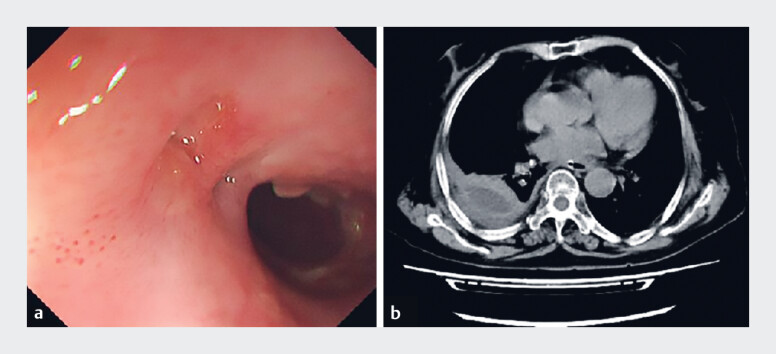 Fig. 3
Fig. 3- —Medical Research Project of Yancheng City Health Commission
- —Science and Technology Plan Project of Yancheng City
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Otolaryngology and Infectious Diseases · Gastroesophageal reflux and treatments
A 61-year-old woman was presented with acute chest pain and dyspnea. Five months earlier, she had undergone endoscopic submucosal dissection (ESD) for circumferential early esophageal cancer (20–27 cm from incisors; Fig. 1 a ). To prevent refractory postoperative stenosis, an intensive anti-fibrosis regimen was administered, including submucosal triamcinolone (200 mg per injection; Fig. 1 b ) three times, and a 6-week tapering course of oral prednisone. Subsequently, the patient underwent two esophageal dilation procedures at 50 and 110 days post-ESD, each combined with a submucosal injection of 200 mg triamcinolone. Post-procedural contrast examination showed no leakage; however, acute symptoms emerged 20 days after the second dilation.
a The wound of the circumferential early esophageal cancer (20–27 cm from incisors) after ESD excision. b Submucosal injection of 20 mL of triamcinolone acetonide 1 week post-ESD. c The fistulous orifice surrounded by extensive white plaques. d A chest CT scan demonstrating mediastinal emphysema and right pleural effusion. CT, computed tomography; ESD, endoscopic submucosal dissection.
Endoscopy disclosed a fistulous orifice at 25 cm surrounded by white plaques ( Fig. 1 c ), and computed tomography (CT) revealed mediastinal emphysema with pleural effusion ( Fig. 1 d ). Candida albicans was identified on culture, indicating severe candidal esophagitis as an opportunistic infection resulting directly from steroid-induced immunosuppression. We consider that the prolonged corticosteroid use critically impaired local tissue defense and integrity, ultimately leading to fungal invasion and delayed perforation.
A fully covered metal stent with an external traction string was deployed to prevent migration and assist retrieval ( Video 1 ). Following adequate thoracic irrigation combined with drainage and initiation of imipenem-cilastatin, the stent was placed endoscopically, achieving complete fistula closure and no evidence of Iohexol contrast leakage ( Fig. 2 a, b ). The stent was safely removed after 4 weeks via the external string. The patient recovered smoothly without stent migration or bleeding, and follow-up endoscopy and CT confirmed fistula healing ( Fig. 3 a, b ).
A case of esophagopleural fistula and candidiasis: endoscopic stenting as salvage therapy.Video 1
a The fully covered metal stent properly positioned at the fistula site. b An Iohexol contrast esophagogram obtained after stent implantation, showing no evidence of leakage at the previous fistula site.
a Endoscopic and b computed tomography (CT) demonstrated the complete healing of the fistula site.
This case underscores that steroid use in extensive ESD defects requires careful titration. Although steroids exert potent anti-fibrotic and immunosuppressive effects that help prevent stenosis 1 2 3 4 , they also impair tissue integrity and increase vulnerability to opportunistic infections 5 —a key contributor to delayed perforation. Therefore, clinical suspicion of fungal invasion warrants early endoscopy, aggressive antifungal therapy, and reevaluation of the corticosteroid use.
Our experience confirms that a string-attached fully covered stent provides triple advantages: reliable fistula closure combined with early oral feeding, migration prevention, and easy retrieval. Together with thorough drainage, it constitutes a safe, effective, minimally invasive approach to complex esophageal perforations.
Endoscopy_UCTN_Code_CPL_1AH_2AZ_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Miyake M Predictors of stricture after non-circumferential endoscopic submucosal dissection of the esophagus and single-dose triamcinolone injection immediately after the procedure Gastrointest Endosc 20239817017710.1016/j.gie.2023.03.01736990127 · doi ↗ · pubmed ↗
- 2Ando Y Risk of stricture after endoscopic submucosal dissection in the cervical esophagus and efficacy of local steroid injection for stricture prevention (with video)Gastrointest Endosc 20241001043104938964479 10.1016/j.gie.2024.06.033 · doi ↗ · pubmed ↗
- 3Zhou S Efficacy of different steroid therapies in preventing esophageal stricture after endoscopic submucosal dissection: a comparative meta-analysis Gastrointest Endosc 202410010201033 e 310.1016/j.gie.2024.08.01739173780 · doi ↗ · pubmed ↗
- 4Carpentier D Local triamcinolone injection and selective add-on oral steroids to prevent esophageal post-endoscopic submucosal dissection stricture: a retrospective analysis in a Western center Endoscopy 20245681181910.1055/a-2328-628238754465 · doi ↗ · pubmed ↗
- 5Gock M Fatal esophageal perforation caused by invasive candidiasis Ann Thorac Surg 2005801120112210.1016/j.athoracsur.2004.02.14716122508 · doi ↗ · pubmed ↗