Preemptive fixation of a jejunal enteral tube extension via novel anchoring system
Jonathan Rozenberg, Rami J. K. Musallam, William F. Abel, Vivek Kesar, Patrick I. Okolo, Varun Kesar

Abstract
Click any figure to enlarge with its caption.
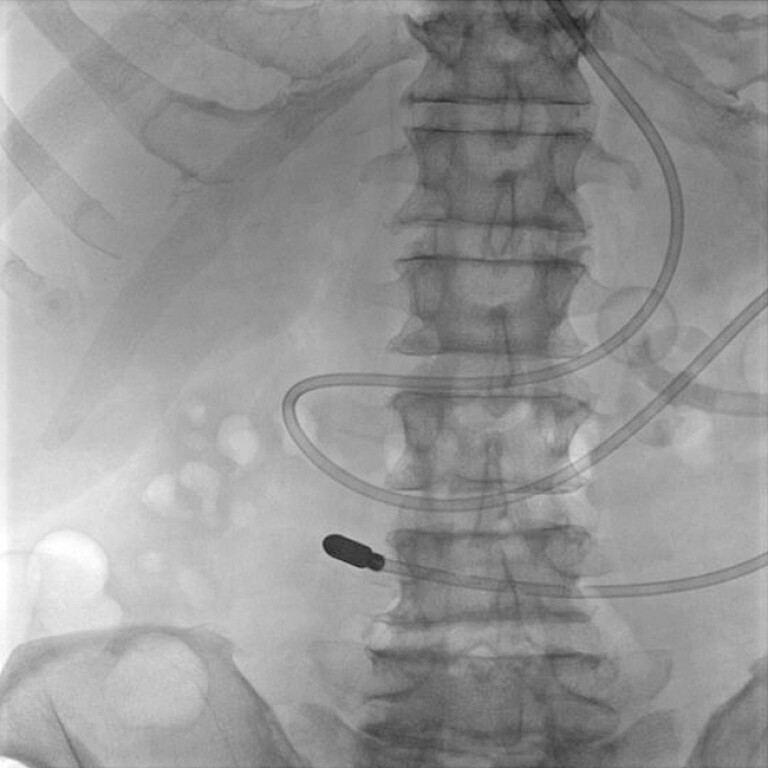 Fig. 1
Fig. 1 Fig. 2
Fig. 2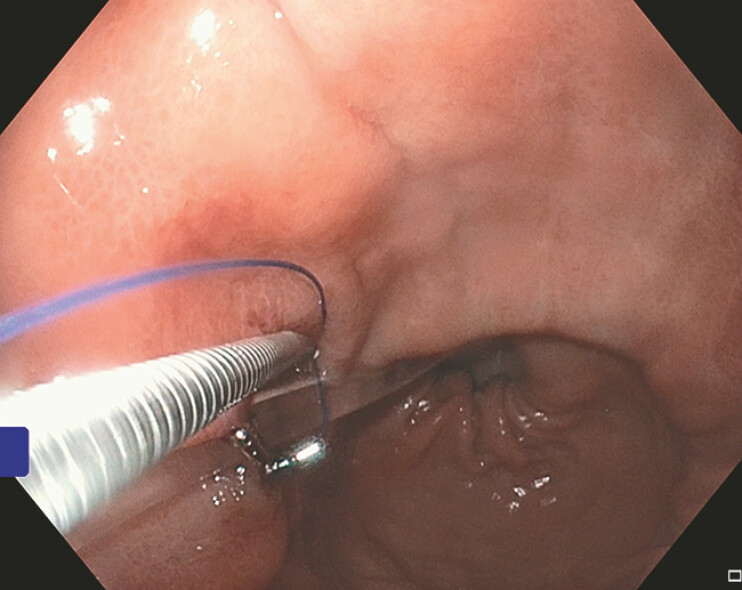 Fig. 3
Fig. 3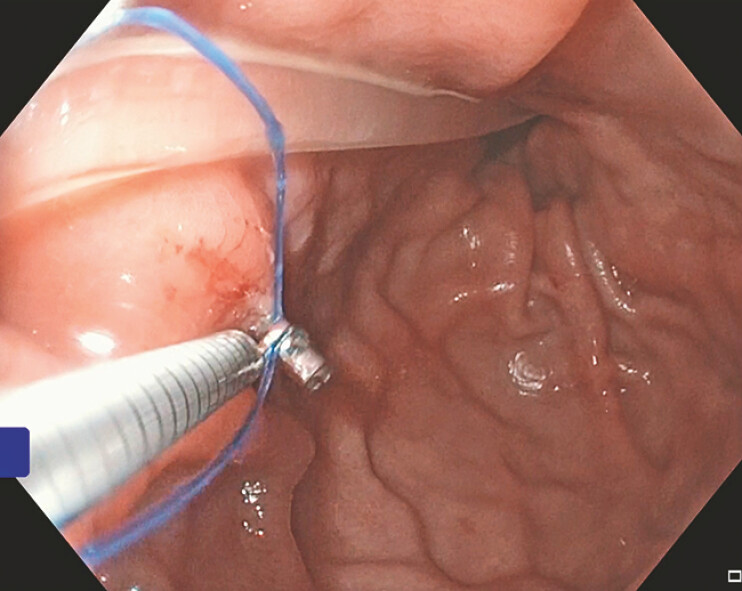 Fig. 4
Fig. 4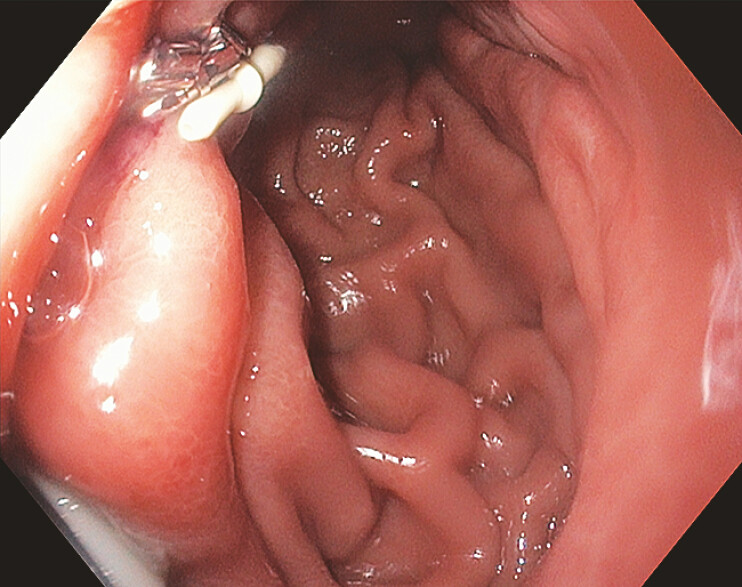 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical Nutrition and Gastroenterology · Esophageal and GI Pathology · Minimally Invasive Surgical Techniques
We present a case of a 76-year-old man with a pertinent past medical history of severe pharyngeal dysphagia status post percutaneous endoscopic gastrostomy (PEG) tube who presented for nasojejunal (NJ) to PEG-jejunostomy (PEG-J) conversion. Two prior attempts at jejunal-arm extension failed secondary to initial proximal positioning of the PEG tube and its consequent migration peri-procedurally. Initial scout films demonstrated the PEG tube bumper and the NJ tip in the proximal jejunum, respectively ( Fig. 1 ). A guidewire was positioned in the jejunum with subsequent NJ tube removal. The jejunal-arm was then extended, over the wire, into the proximal jejunum past the ligament of Treitz ( Fig. 2 ). Once in position, the X-Tack Endoscopic HeliX Tacking System (Boston Scientific; Marlborough, MA, USA) was utilized to secure the jejunal-arm to the proximal aspect of the gastric body ( Fig. 3 , Fig. 4 , Fig. 5 ) for the prevention of jejunal-arm coiling. Thereafter, he tolerated PEG-J feeds with minimal reflux into the venting gastrostomy-arm and was subsequently discharged.
A fluoroscopic image depicting scout imaging of the previously placed percutaneous endoscopic gastrostomy (PEG) tube bumper and a nasojejunal (NJ) tube with its tip in the proximal jejunum, respectively.
A fluoroscopic image demonstrating successful over the wire jejunal arm extension into the proximal jejunum past the ligament of Treitz.
An endoscopic image of HeliX Tack placement, superior to the PEG-jejunum (PEG-J) tube, along the anterior aspect of the proximal gastric body.
An endoscopic image of HeliX Tack placement, inferior to the PEG-J tube, along the anterior aspect of the proximal gastric body.
An endoscopic image exhibiting complete PEG-J arm fixation to the proximal aspect of the gastric body via the X-Tack anchoring system.
Prophylactic fixation of percutaneous endoscopic gastrostomy jejunal arm extension to the proximal aspect of the gastric body via the X-Tack Endoscopic HeliX Tacking System (Boston Scientific; Marlborough, MA, USA) for the prevention of gastric coiling.Video 1
PEG tubes routinely serve as a first-line medium to deliver enteral nutrition for a prolonged period; however, associated dysfunctions/complications are not uncommon 1 . PEG tube dislodgement has been reported to occur in 0.6–4.0% of cases within 7–10 days of initial placement, and up to 12.8% long-term 2 . Literature studies regarding endoscopic intervention in PEG tube dislodgement mainly consist of case reports/series for the management of recurrent dislodgment(s) 1 2 3 4 5 . Of these, the OverStitch device (Boston Scientific; Marlborough, MA, USA) has been predominantly utilized 1 2 3 4 with a recent case incorporating the X-Tack system 5 . Given the scarce literature pertaining to this topic, both the role of pre-emptive endoscopic suturing in jejunal-arm extension(s) as well as the efficacy of the X-Tack system in such cases is unclear. As such, this case illustrates the successful NJ to PEG-J conversion with precautionary jejunal-arm fixation via the X-Tack Endoscopic HeliX Tacking System ( Video 1 ).
Endoscopy_UCTN_Code_TTT_1AO_2AK
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Donald NM Storm AC Endoscopic suturing of a jejunal feeding tube extension to prevent recurrent gastric coiling Video GIE 2020612212310.1016/j.vgie.2020.11.01633738360 PMC 7947371 · doi ↗ · pubmed ↗
- 2Barola S Chen YI Ngamruengphong S Technique of endoscopic suturing of an enteral feeding tube to manage recurrent dislodgement Video GIE 20172646510.1016/j.vgie.2017.01.00129905246 PMC 5990889 · doi ↗ · pubmed ↗
- 3Agnihotri A Barola S Flickinger J Novel technique to manage recurrent PEG-J tube dislodgement with full-thickness endoscopic suturing Am J Gastroenterol 201711281581610.1038/ajg.2017.9428469206 · doi ↗ · pubmed ↗
- 4Agnihotri A Barola S Hill C Endoscopic suturing for the management of recurrent dislodgment of percutaneous endoscopic gastrostomy-jejunostomy tube J Dig Dis 20181917017610.1111/1751-2980.1258129389058 · doi ↗ · pubmed ↗
- 5Nasir A Bouvette C El Haj Chehade AS 3333 Apollo Endosurgery X-Tack Device in Securing Jejunal Extensions Am J Gastroenterol 2023118 S 220810.14309/01.ajg.0000962972.26990.26 · doi ↗