Endoscopic ultrasound-guided colorectal anastomosis using a lumen-apposing metal stent for complete anastomotic stricture
Rafael Prado Pessoa, Caroline Assis Aleixo Chaves, Júlia Gallo de Alvarenga Mafra, Eduardo Seubert Coelho Vieira, Lucas Gallo de Alvarenga Mafra, Luiz Claudio Miranda Rocha, Rodrigo Roda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
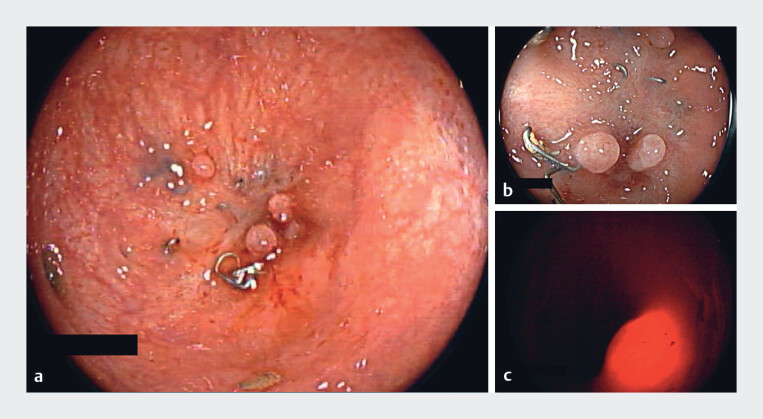 Fig. 1
Fig. 1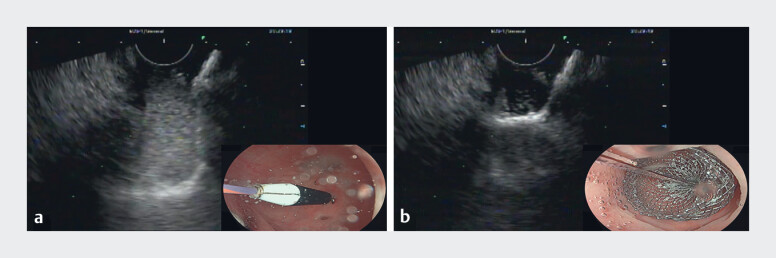 Fig. 2
Fig. 2 Fig. 3
Fig. 3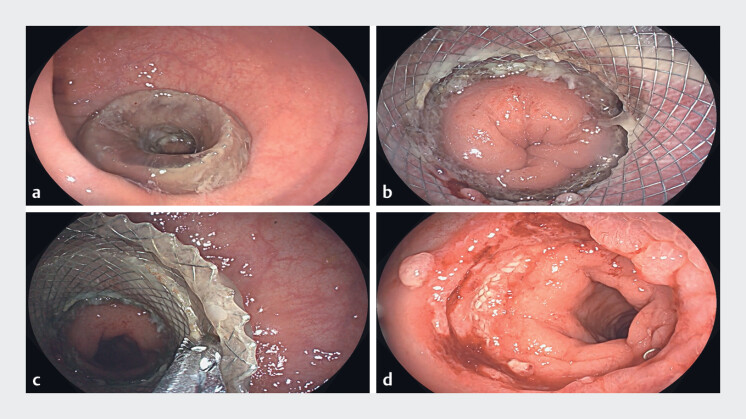 Fig. 4
Fig. 4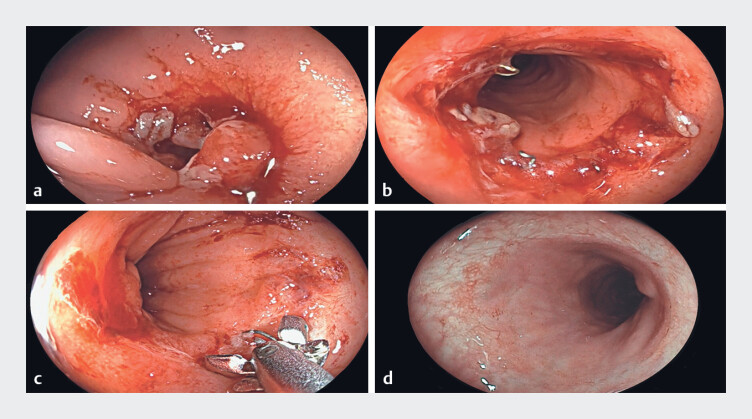 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Colorectal Cancer Surgical Treatments · Gastric Cancer Management and Outcomes
Lumen-apposing metal stents (LAMSs) were designed for pancreatic fluid collections and endoscopic ultrasound (EUS)-guided biliary drainage, but their applications have expanded to include enteric anastomosis creation and the management of gastrointestinal strictures, owing to their variable diameters, anti-migration design, and relatively simple deployment technique 1 2 3 .
A 74-year-old man underwent rectosigmoidectomy with primary anastomosis for recurrent diverticulitis. On postoperative day (POD) 7, he developed an anastomotic leak requiring surgical revision and creation of a loop ileostomy. Seven months later, intestinal continuity was restored. However, on POD 3 after stoma reversal, he developed an acute obstructive abdomen. Urgent flexible sigmoidoscopy revealed a complete colorectal anastomotic stricture. The patient then underwent urgent surgery with the creation of a loop colostomy. Two months later, colonoscopy confirmed persistent complete obstruction ( Fig. 1 ).
An endoscopic view of the colorectal anastomosis showing the complete stricture. a A view from the proximal segment. b A view from the rectal side. ( c ) Attempted transillumination, without a safe window to allow therapeutic intervention.
EUS-guided colorectal anastomosis with LAMSs was selected for recanalization ( Video 1 ). A colonoscope was advanced through the colostomy while a linear echoendoscope was inserted transrectally. A 19-gauge FNA needle was used for access, followed by guidewire introduction and deployment of a 20 × 10-mm electrocautery-enhanced LAMS (Hot Axios; Boston Scientific, Marlborough, Mass, USA; Fig. 2 ). Contrast-tinged water confirmed immediate communication between the segments.
EUS-guided colorectal anastomosis with a lumen-apposing metal stent for the management of the complete anastomotic stricture. EUS, endoscopic ultrasound.Video 1
Endosonographic and endoscopic images of LAMS deployment. a and b Deployment of the LAMS distal flange. LAMS, lumen-apposing metal stent.
A pelvic radiograph 1 week later demonstrated appropriate LAMS expansion ( Fig. 3 ). At 4 weeks, colonoscopy showed a well-positioned stent without adverse events, allowing safe removal and revealing a healed anastomosis ( Fig. 4 ). Persistent strictures required four hydrostatic balloon dilations of up to 20 mm to achieve satisfactory patency. The surgical clips were removed with forceps during the dilation sessions. The patient was subsequently cleared for colostomy takedown ( Fig. 5 ).
Pelvic radiography 1 week after LAMS placement showing an appropriate position and expansion. LAMS, lumen-apposing metal stent.
Endoscopic images from colonoscopy performed 4 weeks after LAMS placement. a The LAMS in the correct position, covered with the mucus. b The LAMS after mucus clearance, with no evidence of complications such as migration, bleeding, or ulceration. c LAMS removal using a retrieval forceps, without difficulties. d Appearance of the anastomotic site after LAMS removal. LAMS, lumen-apposing metal Stent.
a A partial anastomotic stricture visualized 1 week after stent removal, not allowing passage of the 12.8-mm standard colonoscope. b An endoscopic appearance after the first dilation session. c The surgical clips were removed with forceps during the dilation sessions. d An endoscopic appearance on follow-up colonoscopy after four dilation sessions.
EUS-guided colorectal anastomosis using LAMSs proved safe and effective for complete anastomotic obstruction in this case, enabling restoration of intestinal continuity and avoiding additional surgery. Despite promising outcomes, questions remain regarding an ideal dwell time and the need for larger studies 1 2 3 4 5 .
Endoscopy_UCTN_Code_TTT_1AQ_2AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giri S Vaidya A Kale A Efficacy of lumen-apposing metal stents for the management of benign gastrointestinal stricture: a systematic review and meta-analysis Ann Gastroenterol 20233652453210.20524/aog.2023.081937664226 PMC 10433256 · doi ↗ · pubmed ↗
- 2Larson B Adler DG Lumen-apposing metal stents for gastrointestinal luminal strictures: current use and future directions Ann Gastroenterol 20193214114610.20524/aog.2018.033730837786 PMC 6394263 · doi ↗ · pubmed ↗
- 3Santos-Fernandez J Paiji C Shakhatreh M Lumen-apposing metal stents for benign gastrointestinal tract strictures: an international multicenter experience World J Gastrointest Endosc 2017957157810.4253/wjge.v 9.i 12.57129290912 PMC 5740102 · doi ↗ · pubmed ↗
- 4Reddy R Patel U Tarnasky P Lumen-apposing stent placement for management of a short benign colonic anastomotic stricture Video GIE 201839910110.1016/j.vgie.2017.12.00129916480 PMC 6004025 · doi ↗ · pubmed ↗
- 5Kankotia RJ Law JK Shinn BJ Comparison of lumen-apposing metal stents versus endoscopic balloon dilation for the management of benign colorectal anastomotic strictures Gastrointest Endosc 202410013613900010.1016/j.gie.2024.03.00838462058 · doi ↗ · pubmed ↗