Overcoming sharp angulation for biliary access with a novel endoscopic retrograde cholangiopancreatography cannula in surgically altered anatomy
Koichi Soga, Mayumi Yamaguchi, Masaru Kuwada, Ryosaku Shirahashi, Ikuhiro Kobori, Masaya Tamano

Abstract
Click any figure to enlarge with its caption.
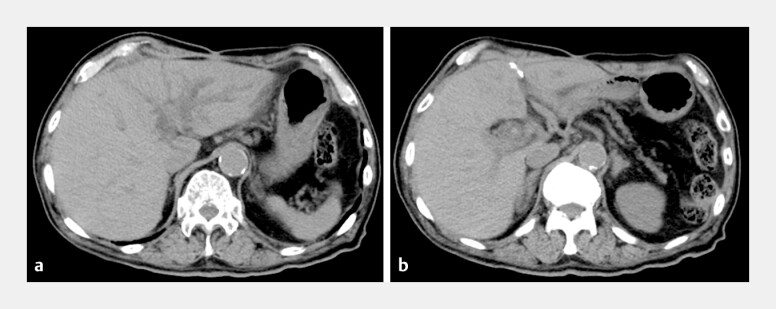 Fig. 1
Fig. 1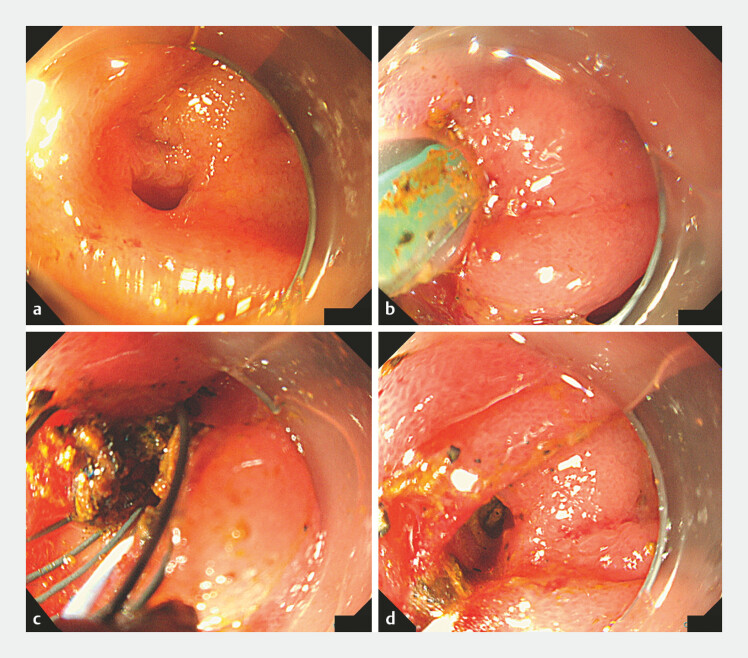 Fig. 2
Fig. 2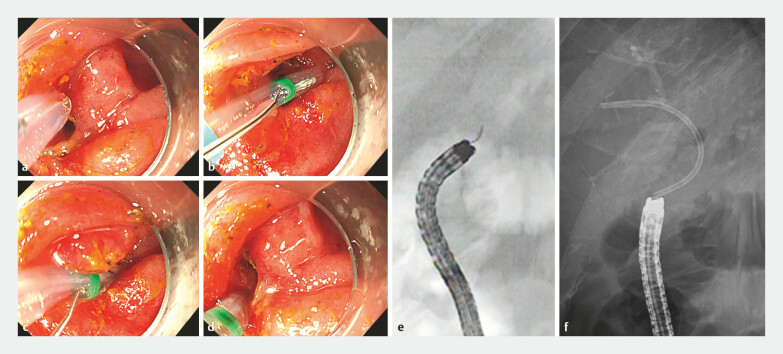 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Minimally Invasive Surgical Techniques · Esophageal and GI Pathology
Endoscopic retrograde cholangiopancreatography (ERCP) in patients with surgically altered anatomy (SAA) remains challenging due to the long afferent limb, sharp angulations, and altered biliary-enteric orientation 1 . Selective cannulation of the right intrahepatic bile duct (R-HBD) is particularly difficult because of the steep alignment between the jejunal limb and the R-HBD. Although single-balloon enteroscopy (SBE) has advanced ERCP in postoperative cases, anatomical angulation often limits device maneuverability and cannulation success.
An 85-year-old man who had undergone pancreaticoduodenectomy a year earlier for pancreatic cancer developed recurrent cholangitis. Endoscopic evaluation using SBE ( Fig. 1 ) identified hepaticojejunostomy sites for both the right and the left HBD (L-HBD). The L-HBD was markedly narrowed and contained intrahepatic stones. ERCP cannulation and guidewire insertion into the L-HBD were successfully performed, and cholangiography confirmed the stricture and stones. Dilation with a biliary balloon (REN 8 mm, Kaneka, Japan) followed by stone extraction using a retrieval basket was achieved. Subsequently, we attempted to access the R-HBD; however, after the left-sided procedure, the access angle from the jejunal limb to the R-HBD became sharply angulated, making conventional cannulation difficult. To overcome this, we utilized a novel ERCP cannula (Engetsu, Kaneka, Japan), with 360° rotational control and a wide vertical range of movement along the X-axis 2 3 4 . These features enabled fine adjustments and successful selective cannulation of the R-HBD, despite the steep anatomy. The procedure concluded with the placement of a plastic and metal stent in the R-HBD and L-HBD, respectively, considering the recurrent cholangitis likely caused by anastomotic strictures and the prolonged left-sided intervention time ( Fig. 2 , Fig. 3 , Video 1 ).
Pre-endoscopic computed tomographic scans. a Marked dilatation of the intrahepatic bile ducts, predominantly in the left hepatic lobe, suggesting biliary obstruction due to hepaticojejunostomy strictures. b Multiple hyperdense foci consistent with intrahepatic stones are identified within the dilated bile ducts at the hepatic hilum.
Endoscopic images during stone extraction. a Before intervention, two orifices were identified at the hepaticojejunostomy site: the 12 o’clock direction leading to the left hepatic duct and the 6 o’clock direction leading to the right hepatic duct. As significant stones were present in the left intrahepatic duct, stone removal was initiated from this side. b Balloon dilation of the anastomotic orifice was performed using a biliary expansion balloon. c Stones were retrieved from the left intrahepatic duct using a retrieval basket (RASEN, Kaneka, Japan). d Complete clearance of the left intrahepatic duct was achieved; however, the right duct could no longer be visualized due to mucosal changes after repeated intervention. Notably, selective access to the right hepatic duct could not be achieved using conventional ERCP cannulas and guidewires. ERCP, endoscopic retrograde cholangiopancreatography.
Endoscopic and fluoroscopic images during stone extraction using the novel endoscopic retrograde cholangiopancreatography (ERCP) cannula (Engetsu, Kaneka, Japan). a The left hepatic duct orifice was visible, but the right hepatic duct could not be identified; therefore, cannulation into the right intrahepatic duct was initiated using the novel ERCP cannula. b, c By rotating the novel ERCP cannula, selective access to the right hepatic duct was attempted under steep anatomical alignment. d By sharply bending the device tip along the X-axis toward the 6 o’clock direction, safe and rapid cannulation of the right hepatic duct was achieved. e A fluoroscopic image showing the novel ERCP cannula accessing the right hepatic duct in the opposite direction to the endoscope’s natural curvature, highlighting its unique range of movements. f Final placement of a plastic stent into the right hepatic duct was successfully performed, confirming the feasibility of selective biliary access in the surgically altered anatomy with acute angulation.
Overcoming sharp angulation for biliary access using a novel endoscopic retrograde cholangiopancreatography cannula in the surgically altered anatomy. This video demonstrates the cannula’s technical advantages and successful selective access where conventional devices failed.Video 1
This case demonstrates that the novel ERCP cannula facilitates precise biliary access in the SAA with sharp angulations, where conventional devices often fail. This video highlights its mechanical advantages and potential clinical utility in managing anatomically complex biliary reconstructions.
Endoscopy_UCTN_Code_TTT_1AR_2AK
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Krutsri C Kida M Yamauchi H Current status of endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy World J Gastroenterol 2019253313333331341358 10.3748/wjg.v 25.i 26.3313 PMC 6639547 · doi ↗ · pubmed ↗
- 2Kunogi Y Irisawa A Yamamiya A All-in-one sphincterotome with high rotation performance and freely bendable blade for endoscopic sphincterotomy in patients with surgically altered anatomy (a case series with video)DEN Open 20245 e 7001939386274 10.1002/deo 2.70019 PMC 11461899 · doi ↗ · pubmed ↗
- 3Soga K Sakakibara K Soma Y Innovative sphincterotomy knife and indigo carmine strategy for bile duct stones in a patient with surgically altered anatomy Endoscopy 202557 E 508E 50940436405 10.1055/a-2599-7007 PMC 12119199 · doi ↗ · pubmed ↗
- 4Soga K Yamaguchi M Fujiwara T Endoscopic biliary drainage using a narrow-diameter endoscope in a patient with obstructive jaundice and pancreatic cancer Endoscopy 202456 E 853E 85539379057 10.1055/a-2418-1018 PMC 11461093 · doi ↗ · pubmed ↗