Identification of an intramuscular gastric subepithelial stromal tumor during endoscopic resection by using endoscopic ultrasound within the submucosal tunnel
Leandro Corradino, Dario Biasutto, Benedetto Neri, Serena Stigliano, Cristina Lucidi, Valeria DʼOvidio, Francesco Maria Di Matteo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
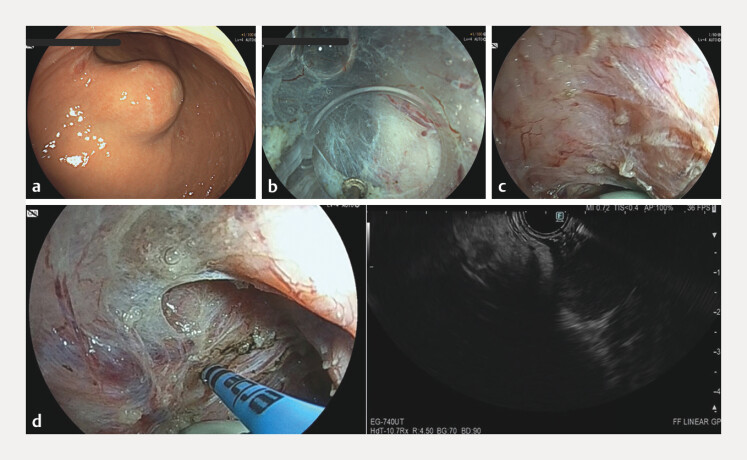 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastrointestinal disorders and treatments · Gastrointestinal Bleeding Diagnosis and Treatment
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors of the gastrointestinal tract 1 . The management includes endoscopic resection (ER), surgery and oncological medical treatment 2 .
We report the case of an 80-year-old woman with a subepithelial lesion of the greater gastric curve ( Video 1 ). During endoscopic ultrasound (EUS), it appeared as an oval, hypoechoic homogeneous 29 mm lesion with hypervascularization on contrast-enhanced-EUS, originating from the muscular layer 3 . Fine needle biopsy histology revealed a G1 GIST 4 .
An endoscopic image showing marking of the gastrointestinal stromal tumor by using a linear echoendoscope advanced through the submucosal tunnel with an argon plasma coagulation probe during submucosal tunnel endoscopic resection.Video 1
The GIST was treated by using a submucosal tunnel endoscopic resection (STER) technique with an operative gastroscope (EG-760CT, Fujifilm corp. Tokyo, Japan) and a HybridKnife T-type I-jet (ERBE Elektromedizin, Tuebingen, Germany).
Initially, the lesion was visible as subepithelial bulging. After submucosal tunneling, the lesion was not clearly detectable both from inside and outside the tunnel, as it was located within the muscular layer and covered by muscular fibers. Thus, to identify the GIST, we performed an EUS by advancing a linear echoendoscope (EG-740UT, Fujifilm corp. Tokyo, Japan) through the submucosal tunnel. The GIST was then identified, marked with argon plasma coagulation 30W on the muscular layer ( Fig. 1 , panels a–d ) and removed after the selective dissection of the muscular fibers covering the lesion. At the end of the procedure, the tunnel was intact, and the access was completely closed with through-the-scope clips. Histology confirmed the G1 GIST.
(Panels a–d ): Panel a : A subepithelial lesion of the lesser curve of the stomach, previously diagnosed as a low-grade GIST, was planned for endoscopic removal with submucosal tunnelling endoscopic resection (STER). Panel b : During the creation of the submucosal tunnel, it was difficult to identify the lesion. Panel c : To overcome this unexpected issue, an echoendoscope was advanced through the submucosal tunnel to allow the lesion’s identification. Panel d : Combined endoscopic and endoscopic ultrasound images of the marking of the lesion’s margins with an argon plasma coagulation probe.
To our knowledge, this is the first report of a GIST of the muscular gastric layer treated with STER, requiring intraprocedural identification with EUS performed from within the submucosal tunnel. Lesions originating from the deep gastric wall layer may be at a higher risk of ER failure, also due to possible difficulties in their identification during the procedure 5 . This approach could minimize this risk and ease the procedure, avoiding the need for more invasive treatments such as laparoscopy and endoscopic cooperative surgery.
Endoscopy_UCTN_Code_CCL_1AB_2AC_3AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gupta P Tewari M Shukla HS Gastrointestinal stromal tumor Surg Oncol 20081712913810.1016/j.suronc.2007.12.00218234489 · doi ↗ · pubmed ↗
- 2Yue L Sun Y Wang X Advances of endoscopic and surgical management in gastrointestinal stromal tumors Front Surg 2023101.092997 E 610.3389/fsurg.2023.1092997 PMC 1013046037123546 · doi ↗ · pubmed ↗
- 3Deprez PH Moons LMGOʼToole D Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20225441242910.1055/a-1751-574235180797 · doi ↗ · pubmed ↗
- 4Nagtegaal ID Odze RD Klimstra D The 2019 WHO classification of tumours of the digestive system Histopathology 20207618218810.1111/his.1397531433515 PMC 7003895 · doi ↗ · pubmed ↗
- 5Yuan Y Sun L Zhou X Risk factors for the failure of endoscopic resection of gastric submucosal tumors: a long-term retrospective case-control study Gastric Cancer 20222592994235752993 10.1007/s 10120-022-01306-9 · doi ↗ · pubmed ↗