Indomethacin Fails to Increase Intestinal Permeability in Healthy Volunteers
Michael Camilleri, Irene Busciglio, Paula Carlson, Saam Dilmaghani, Camille Lupianez-Merly, David Y. Yang, Michael Ryks, Monique Ferber, Dounia Houamel, Stéphanie Perot, François Montestruc

TL;DR
Indomethacin did not increase gut permeability in healthy people, challenging its use as a model for studying gut barrier function.
Contribution
This study shows that indomethacin may not reliably induce intestinal hyperpermeability in healthy volunteers.
Findings
Indomethacin did not increase 13C-mannitol excretion in participants.
No significant changes in biomarkers like zonulin or calprotectin were observed.
The expected increase in intestinal permeability was not consistently observed.
Abstract
Indomethacin is often used experimentally to induce intestinal hyperpermeability, enabling evaluation of interventions targeting barrier function. We conducted a randomized, double-blind, placebo-controlled study (NCT05538247) in healthy volunteers to assess whether a supplement could mitigate indomethacin-induced hyperpermeability. Participants received 150 mg/d of indomethacin for 6 days, either before or during placebo/supplement administration. Permeability was measured using 13C-mannitol and lactulose urinary excretion. Contrary to expectations, indomethacin failed to increase 13C-mannitol excretion in either group. No meaningful elevations in serum (zonulin, claudins) or fecal (calprotectin) biomarkers were observed. Our findings suggest that the expected increase in intestinal permeability after indomethacin administration may not be consistently observed in healthy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
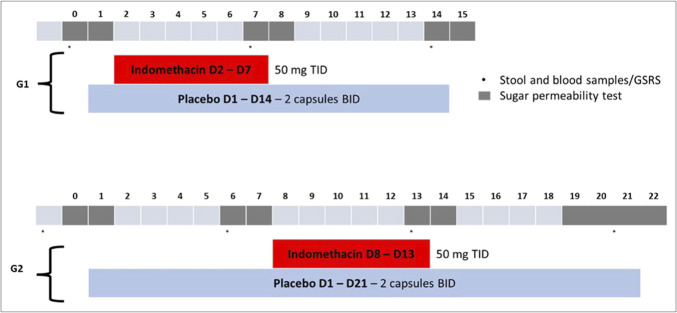 Figure 1
Figure 1| GROUP 1: 7 d indomethacin with concurrent placebo | |||
| Baseline | Day 7 indomethacin | Change from baseline to Day 7 | |
| 13C-Mannitol at 2–24 hr (mg) | |||
| N | 13 | 13 | 13 |
| Mean (SD); [95% CI of mean] | 7.0 (4.8); [4.1; 9.9] | 6.6 (3.4); [4.5; 8.7] | −0.4 (4.9); [−3.3; 2.6] |
| Median | 5.2 | 6.1 | 1.2 |
| Lactulose at 2–24 hr (mg) | |||
| N | 13 | 13 | 13 |
| Mean (SD); [95% CI of mean] | 1.8 (1.2) [1.1; 2.5] | 2.6 (2.0) [1.4; 3.9] | 0.8 (1.6); [−0.1; 1.8] |
| Median | 1.4 | 1.6 | 0.0 |
- —Biocodex
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBarrier Structure and Function Studies · Gut microbiota and health · Drug Transport and Resistance Mechanisms
INTRODUCTION
Inducing intestinal barrier dysfunction with nonsteroidal anti-inflammatory drugs (NSAIDs) such as indomethacin has been a common approach to explore intestinal permeability (1,2) and assess interventions designed to restore barrier integrity. The aim of our study was to investigate whether an oral supplement could strengthen the intestinal barrier function and counteract the acute hyperpermeability induced by the NSAID, indomethacin, in healthy human volunteers. In this report, we have assessed the effects of exogenous administration of indomethacin in healthy human volunteers.
METHODS
This was a randomized, double-blind, placebo-controlled, parallel-arm clinical study (NCT05538247) in healthy adult volunteers. The study was divided into 2 separate substudies referred to as Group 1 and Group 2, in which the initiation and duration of the study products differed according to the group. Subjects could freely choose to participate in Group 1 or Group 2 at the screening visit, according to their availability. At the inclusion visit, in each group, eligible subjects were randomized (1:1) in a double-blind manner to receive either experimental therapy or placebo. All Group 1 and Group 2 subjects received an open-label, short-term (6 days) indomethacin challenge (150 mg/d) to increase intestinal permeability: For Group 1 subjects, treatment was started with indomethacin and lasted 14 days; for Group 2 subjects, treatment was started 7 days before indomethacin and lasted 20(±1) days (Figure 1).
Experimental protocol showing days of administration of placebo and indomethacin. bid, twice a day; tid, 3 times a day; D, day; G1, Group 1; G2, Group 2; GSRS, gastrointestinal symptoms rating scale.
Measurement of intestinal permeability and endpoints
The permeability test was based on the excretion of ingested sugar probes (1,000 mg lactulose and 100 mg ^13^C-mannitol) in accordance with a previously validated assay (3) in distinct urine collection intervals to selectively characterize the permeability of different parts of the gastrointestinal tract: The 0–2-hour urine collection was a marker of small intestinal permeability, the 2–8-hour urine collection was a marker of both small intestinal and colonic permeability, and the 8–24-hour urine collection was a marker of colonic permeability. The primary permeability end point in the analysis was ^13^C-mannitol excretion 2–24 hours (mg) expressed as the change from baseline to the end of treatment with indomethacin, that was day 7 in Group 1 and day 13 in Group 2.
Additional secondary observations included fecal and serum biomarkers of barrier function and intestinal injury [calprotectin (4), zonulin (5), claudin 1 (6), C-reactive protein (CRP) (7)] and symptoms scores (gastrointestinal symptom rating scale [GSRS]).
Gastrointestinal symptom response scale
The GSRS is a validated questionnaire to evaluate gastrointestinal symptoms in gastrointestinal disorders (8).
Statistical analysis
The primary end point was absolute change from baseline of ^13^C-mannitol 2–24 hours (mg) assessed with an analysis of covariance model which included terms to adjust for the baseline value and treatment arm. The average of the adjusted difference in the mean absolute change from baseline was reported with SEs of the mean, 2-sided 95% confidence interval (CI), and P value. Multiple imputation using the fully conditional specification method was used for missing data.
RESULTS
Supplement Table 1 (http://links.lww.com/CTG/B415) presents demographics, participant habits, bowel function, significant medical history at baseline, and compliance with protocol treatment of all participants in group 1 and group 2 of study. There were no significant differences among the 2 groups.
Table 1 summarizes the permeability end point analyses, based on the primary urinary excretion of ^13^C-mannitol 2–24 hours (mg) and secondary end points of urinary excretion of lactulose 2–24 hours (mg), as well as serum biomarkers of intestinal injury and intestinal permeability. None of these changes were statistically significant at the 5% level.
Change in 13C-mannitol 2–24 hours from baseline to day 7 in Group 1 and to day 13 in Group 2
In the placebo arm, mean values of ^13^C-mannitol 2–24 hours were similar between baseline and day 7, with an adjusted mean change from baseline (95% CI) of −0.5 mg [−4.9; 3.8]. Similarly, in the placebo arm, mean values of ^13^C-mannitol 2–24 hours were similar between baseline and day 13, with an adjusted mean change from baseline (95% CI) of −3.7 mg [−7.6; 0.1]. The lack of increase in excretion of ^13^C-mannitol 2–24 hours suggests that indomethacin did not increase intestinal permeability in subjects treated with placebo in either group.
Changes in secondary endpoints
No meaningful changes were observed in serum zonulin or claudins, nor in fecal calprotectin. GSRS total scores increased modestly, without corresponding biomarker shifts.
Gastrointestinal symptoms
Based on the total score and abdominal pain score on the GSRS, there was a significant increase in total score and abdominal pain score in subjects in Group 1 but not in Group 2. Note also the increase in diarrhea score in Group 2, which was associated with large variance and did not reach statistical significance.
DISCUSSION
Although indomethacin was associated with adverse effects, it is worth noting that several biomarkers used to assess changes in intestinal permeability using oral sugar probe molecules, and using serum and fecal measurements did not identify such effects of indomethacin on intestinal permeability. These results do not support a consistent increase in intestinal permeability after indomethacin administration. Despite its frequent use, our findings indicate that indomethacin may not consistently provoke intestinal hyperpermeability in healthy individuals, as measured by sugar probe excretion or biomarker analysis. It is important to keep this in perspective in relation with future studies addressing the potential effects on intestinal barrier function of novel experimental therapeutic approaches. Future research may consider higher NSAID dose, longer exposure periods, or study populations exhibiting preexisting gut barrier alteration.
CONFLICTS OF INTEREST
Guarantor of the article: Michael Camilleri, MD, DSc, MACG.
Specific author contributions: M.C.: PI, senior author, conception of project, writing and revising manuscript. I.B.: laboratory supervisor. P.C.: study coordinator. S.D., C.L.-M., and D.Y.Y.: participant care, revising manuscript. M.R.: laboratory technician. M.F.: study coordinator. D.H.: study protocol development, revising manuscript. S.P., and F.M.: statistician, revising manuscript.
Financial support: This study was funded by a research grant from Biocodex, 7 avenue Gallieni, 94250 Gentilly, France.
Potential competing interests: Dounia Houamel is an employee of Biocodex. The other authors have no conflicts of interest.
Trial registry: ClinicalTrials.gov #NCT05538247.
Supplementary Material
**
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Edogawa S Peters SA Jenkins GD Sex differences in NSAID-induced perturbation of human intestinal barrier function and microbiota. FASEB J 2018;32(12):fj 201800560 R.10.1096/fj.201800560 RPMC 621982529897814 · doi ↗ · pubmed ↗
- 2Goldstein J Cryer B. Gastrointestinal injury associated with NSAID use: A case study and review of risk factors and preventative strategies. Drug Healthc Patient Saf 2015;7:31–41.25653559 10.2147/DHPS.S 71976 PMC 4310346 · doi ↗ · pubmed ↗
- 3Khoshbin K Khanna L Maselli D Development and validation of test for “leaky gut” small intestinal and colonic permeability using sugars in healthy adults. Gastroenterology 2021;161(2):463–75.e 13.33865841 10.1053/j.gastro.2021.04.020PMC 8328885 · doi ↗ · pubmed ↗
- 4Damms A Bischoff SC. Validation and clinical significance of a new calprotectin rapid test for the diagnosis of gastrointestinal diseases. Int J Colorec Dis 2008;23(10):985–92.10.1007/s 00384-008-0506-018629518 · doi ↗ · pubmed ↗
- 5Fasano A. All disease begins in the (leaky) gut. Role of zonulin-mediated gut permeability in the pathogenesis of some chronic inflammatory diseases. F 1000 Res 2020;9:F 1000 Faculty Rev-69.10.12688/f 1000 research.20510.1PMC 699652832051759 · doi ↗ · pubmed ↗
- 6Weber CR Nalle SC Tretiakova M Claudin-1 and claudin-2 expression is elevated in inflammatory bowel disease and may contribute to early neoplastic transformation. Lab Invest 2008;88(10):1110–20.18711353 10.1038/labinvest.2008.78PMC 2586671 · doi ↗ · pubmed ↗
- 7Hoshiko H Feskens EJM Oosterink E Identification of leaky gut-related markers as indicators of metabolic health in Dutch adults: The Nutrition Questionnaires plus (N Qplus) study. P Lo S One 2021;16(6):e 0252936.34086828 10.1371/journal.pone.0252936 PMC 8177645 · doi ↗ · pubmed ↗
- 8Svedlund J Sjödin I Dotevall G. GSRS — A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig Dis Sci 1988;33(2):129–34.3123181 10.1007/BF 01535722 · doi ↗ · pubmed ↗