Evaluating the safety of prenatal HIV PrEP use: Perinatal outcomes from three cohort studies in Western Kenya
Ben Odhiambo, Joshua Stern, John Kinuthia, Felix Abuna, Eunita Akim, Tessa Concepcion, Julia C. Dettinger, Laurén Gómez, Anna Larsen, Mary Marwa, Jerusha Mogaka, Nancy Ngumbau, Emmaculate Nzove, Barbra A. Richardson, Salphine Watoyi, Grace John-Stewart, Jillian Pintye

TL;DR
This study confirms that using HIV PrEP during pregnancy is safe and may even reduce the risk of low birthweight in Western Kenya.
Contribution
The study provides new evidence on the safety and potential benefits of TDF-based HIV PrEP use during pregnancy in a real-world setting.
Findings
HIV PrEP-exposed pregnancies had lower rates of low birthweight compared to non-exposed pregnancies.
Preterm birth was less frequent in pregnancies with HIV PrEP use in the first and third trimesters.
No significant differences were found in most perinatal outcomes between HIV PrEP-exposed and non-exposed pregnancies.
Abstract
Existing data support the safety of daily oral tenofovir disoproxil fumarate (TDF)-based HIV pre-exposure prophylaxis (PrEP) use in pregnancy, yet ongoing monitoring is needed. We analyzed data from three recently completed HIV PrEP safety and implementation studies (PrIMA, PrIMA-X, and mWACh-PrEP) that enrolled women who were offered and/or initiated TDF-based HIV PrEP at routine health clinics in Western Kenya to summarize perinatal outcomes following HIV PrEP use in pregnancy. Data were included in the analysis from participants who were ≥ 15 years, HIV-negative, enrolled ≤32 weeks gestation and remained pregnant until at least 24 weeks gestation. We summarized the frequency of each pregnancy outcome (stillbirth, preterm birth, low birthweight, neonatal death, congenital anomalies) by study cohort, HIV PrEP exposure status (any vs. none), and timing of first HIV PrEP exposure (first,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
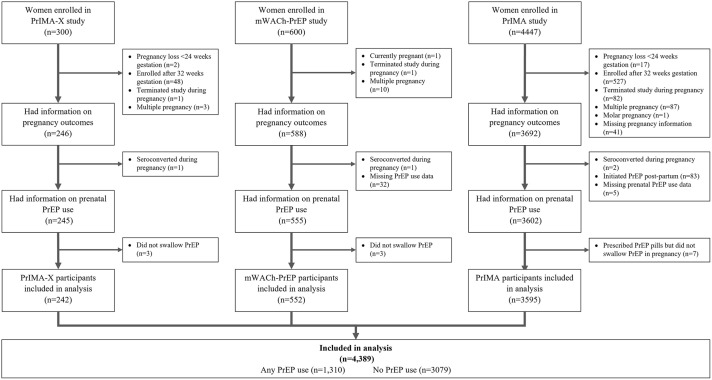 Fig 1
Fig 1- —http://dx.doi.org/10.13039/100015691Division of Microbiology and Infectious Diseases, National Institute of Allergy and Infectious Diseases
- —http://dx.doi.org/10.13039/100009633Eunice Kennedy Shriver National Institute of Child Health and Human Development
- —http://dx.doi.org/10.13039/100000056National Institute of Nursing Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · HIV/AIDS drug development and treatment · HIV-related health complications and treatments
Introduction
High HIV incidence among cisgender women of childbearing age remains a public health challenge in HIV high burden countries, including Kenya [1–4]. HIV acquisition risk doubles during pregnancy and postpartum compared to non-pregnant periods [5] due to biological alterations and social and behavioral factors [2,3,5,6]. The World Health Organization (WHO) and Kenya’s Ministry of Health recommend offering daily oral tenofovir disoproxil fumarate (TDF)-based pre-exposure prophylaxis (PrEP) for HIV prevention to pregnant and lactating women at substantial ongoing risk for HIV acquisition, based on a large body of safety data on TDF use for HIV treatment among women living with HIV [7–11]. Existing safety data of prenatal HIV PrEP use among women without HIV are reassuring, finding no association between adverse perinatal outcomes and prenatal HIV PrEP use [12]. Yet, safety studies to date focus on women who initiate HIV PrEP during pregnancy, mostly in the second and third trimesters only [13–18], and do not evaluate gestational timing or duration of exposure. As oral TDF-based PrEP is scaling up among pregnant and breastfeeding women in East Africa with notable implementation successes in Kenya [12,16], WHO emphasizes the need for further safety data, especially among women who initiate HIV PrEP outside of research settings. Data from recent HIV PrEP implementation studies among pregnant women could fill remaining safety evidence gaps, especially studies with participants who initiated HIV PrEP in routine settings and prior to pregnancy.
Our team recently conducted three large HIV PrEP safety and/or implementation studies among pregnant women in Western Kenya. The PrIMA Study (PrEP Implementation for Mothers in Antenatal Care; NCT03070600) enrolled n = 4447 pregnant participants at any time gestational age and offered HIV PrEP (16.2%% initiated PrEP in pregnancy as part of study procedures) [19]. In addition to prior PrIMA enrollees, the PrIMA Extension Study (PrIMA-X) included a novel observational cohort of n = 300 pregnant participants who initiated HIV PrEP before or during pregnancy, yet prior to study enrollment. The mWACh (Mobile Women Adolescent and Child Health; NCT04472884) HIV PrEP Study enrolled n = 600 participants who all initiated HIV PrEP between 24–32 weeks gestation within routine antenatal care. We conducted a descriptive prospective analysis using existing data from these studies to summarize the frequency of adverse perinatal outcomes following HIV PrEP exposure and to evaluate timing of HIV PrEP exposure in pregnancy and perinatal outcomes among women in Kenya with and without HIV PrEP exposure.
Methods
Study design and participants
This secondary analysis utilized data from participants enrolled in the PrIMA study (http://clinicaltrials.gov/show/NCT03070600) who did and did not initiate HIV PrEP in pregnancy, novel ANC clients enrolled in the PrIMA-X (PrIMA Extension) study, which was not a clinical trial, who initiated PrEP prior to or during pregnancy, and the mWACh-PrEP study (NCT04472884; all participants-initiated PrEP at 24–32 weeks gestation). We combined cohort data to summarize frequency distributions of adverse perinatal outcomes across cohorts and HIV PrEP exposure statuses. We utilized data collected from all studies up to April 2024 following the inclusion and exclusion criteria for the parent studies with additional criteria (Table 1).
Table 1: Inclusion and exclusion criteria by study cohort.
The PrIMA Study was a cluster randomized trial of HIV PrEP counseling strategies conducted between January 2018 and July 2021 in 20 mother and child health clinics in Homa Bay and Siaya counties, Kenya. The study protocol has been described in detail previously [20]. Briefly, antenatal care attendees were eligible for enrollment if they were: currently pregnant, HIV negative, not currently using HIV PrEP, ≥ 15 years old, tuberculosis negative, planned to reside in the region for at least 1-year postpartum, planned to receive postnatal and infant care at the study facility, and were not currently enrolled in any other studies. Following enrollment, pregnant women were counseled on PrEP as part of routine ANC, either universally (universal arm) or after undergoing HIV risk screening and identified as at risk (targeted arm). Women enrolled at any gestational age during pregnancy and were followed monthly until 9 months postpartum, regardless of HIV PrEP use. For the current analysis, we used data from PrIMA participants who had no history of PrEP use, enrolled in the study at ≤32 weeks gestation and remained pregnant until at least 24 weeks gestation, in order to allow for a non-exposure comparison group of birth outcomes for our other studies.
The PrIMA-X Study is an ongoing longitudinal observational extension cohort study that evaluates safety of oral HIV PrEP use during pregnancy and postpartum at four clinics in Western Kenya. PrIMA-X study follows mother-child pairs up to 60 months post-birth. Women were recruited and enrolled into PrIMA-X study if they were at least 15 years old, HIV negative, and receiving maternal and child health (MCH) services at the participating study sites. The PrIMA-X study population consists of n = 1191 study participants, of whom n = 891 are mother-infant pairs rolled over from the PrIMA study. HIV PrEP safety outcome results from the original PrIMA cohort with PrEP exposure have previously been published [19]. The PrIMA-X study newly enrolled n = 300 pregnant women who initiated HIV PrEP prior to pregnancy or during pregnancy, enrolled at any gestational age, specifically to augment the number of participants with HIV PrEP exposure during pregnancy. For the current analysis, we used data from these n = 300 newly enrolled PrIMA-X participants who enrolled in the study at ≤32 weeks gestation, initiated HIV PrEP prior to pregnancy or during the first trimester, and remained pregnant until at least 24 weeks gestation.
The mWACh-PrEP study is an ongoing randomized trial conducted at five MCH clinics in Siaya and Kisumu, Kenya, that seeks to improve HIV PrEP adherence using mobile health strategies among women at risk for HIV who initiate HIV PrEP during routine antenatal care. Pregnant women were eligible for enrollment if they were between 24–32 weeks gestation, aged ≥18 years, HIV negative, had an HIV risk score ≥6 (translating to HIV incidence 7.3 per 100 person-years) [21], initiated HIV PrEP that day during ANC, planned to reside in the area for at least one year postpartum, and receive postnatal and infant care at the study clinic. Women who had previously used HIV PrEP were not eligible for enrollment in the study [22]. mWACh-PrEP enrolled n = 600 women who initiated HIV PrEP during pregnancy.
Data collection
At enrollment and during study visits, study nurses administered questionnaires using a tablet-based Research Electronic Data Capture (REDCap) [23] in English, Swahili or Dholuo languages as per the woman’s preference. Questionnaires include assessment of sociodemographic characteristics, HIV PrEP use information, and obstetric information. Participants self-reported male partner characteristics. Syphilis test results were abstracted from the participant’s medical records. The duration of pregnancy was estimated between the first day of the last menstrual period to the date of delivery or pregnancy loss. Evaluation of peripartum outcomes was collected at the first study visit after birth (≤6 weeks) or end of pregnancy for each study participant. All perinatal outcomes (pregnancy loss, stillbirth, preterm birth, low birthweight, congenital anomalies, and neonatal death) were abstracted from clinical records or ascertained by study nurses who are trained in the collection of peripartum outcomes.
Study measures
Timing of first HIV PrEP exposure in pregnancy was categorized as no HIV PrEP exposure, first trimester (initiated PrEP prior to pregnancy or during the first trimester), second trimester, or third-trimester exposure. Among mWACh-PrEP participants, HIV PrEP initiation date corresponded to the study enrollment date as all participants initiated HIV PrEP same day during ANC as part of the parent study’s inclusion criteria. All mWACh-PrEP participants who met the analysis’ inclusion criteria were categorized as having second or third-trimester HIV PrEP initiation. Among PrIMA and PrIMA-X participants, HIV PrEP initiation date was ascertained at enrollment and/or follow-up, and timing of HIV PrEP initiation in relation to pregnancy was calculated by subtracting the HIV PrEP initiation date from the estimated pregnancy start date. Outcomes included preterm birth (<37 weeks) determined by last menstrual period, low birth weight (<2500g), stillbirth (pregnancy loss ≥24 weeks), WHO growth indicators (weight-for age Z-score, height-for-age Z-score) [24], congenital malformations, and neonatal death (death of a live-born infant within the first 28 days of life). We did not evaluate small-for-gestational-age due to >50% missingness of birth length. We evaluated each individual outcome in separate models.
Statistical analysis
Descriptive statistics were used to summarize frequency distributions of adverse pregnancy outcomes. We analyzed and compared each adverse pregnancy outcomes by study cohort, HIV PrEP exposure status, and timing of HIV PrEP exposure (no HIV PrEP exposure, first, second, or third-trimester exposure) using Fisher’s exact test for categorical variables (stillbirth, neonatal death, congenital anomalies) and Wilcoxon rank-sum tests to compare the distribution of continuous variables (gestational age, weight at birth) to detect differences between exposure groups since we expect rare outcomes to occur in <5 cases in some groups.
In an exploratory analysis, we used separate Poisson regression models for each individual perinatal outcome to test whether the timing of first HIV PrEP exposure in pregnancy (no HIV PrEP exposure vs. first, second, or third-trimester exposure) was associated with preterm birth, low birth weight, or stillbirth). All models were adjusted for study cohort a priori. We also conducted separate exploratory analyses to test whether timing of HIV PrEP initiation (prior to pregnancy vs. during pregnancy) and duration of exposure (time from first PrEP exposure in pregnancy to discontinuation or birth/end of pregnancy) were associated with any adverse outcome. In each model, we accounted for maternal age at enrollment, primigravida, and clustered by study cohort as a random effect. Mode of delivery and infant sex were not included as adjustment variables due to the differential missingness of these variables across cohorts.
Ethical considerations
Before commencement, the PrIMA, PrIMA-X, and mWACh-PrEP studies received approval from both the University of Washington Institutional Review Board (IRB) and the Kenyatta National Hospital and University of Nairobi Ethics and Research Committee (KNH-UoN ERC): PrIMA (P73/02/2017), PrIMA-X (P921/11/2019), mWACh-PrEP (P319/05/2021). Recruitment occurred from 15 Jan 2018–31 July 2019 for the PrIMA study; 26 Oct 2020–6 June 2023 for the PrIMA-X study; and 14 Feb 2022–13 July 2023 for the mWACh-PrEP study. All women who were interested in participating and met the eligibility criteria, provided written informed consent for their enrollment.
Results
In total, 4,389 women across the three cohorts met inclusion criteria and were included in the current analysis (82% of the overall combined study population) (Fig 1). The median overall age was 24.1 years (IQR: 21.0,28.6), and the median gestational age at enrollment was 24 weeks (IQR: 20, 28). Most women (83.4%) were married with a median of 10 years of education (IQR: 8.0,12.0). There were differences in the frequency of being primigravida, having a partner known to be living with HIV, and self-reported HIV PrEP adherence across studies (Table 2).
Table 2: Characteristics of participants included in the analysis (n = 4389).
Flow diagram of enrollment into studies and participant inclusion in combined analyses.
Among women with HIV PrEP exposure during pregnancy (n = 1310), most initiated HIV PrEP in the second trimester (56.2%), followed by the third trimester (35.5%), first trimester (5.9%), and prior to pregnancy at 2.4%. The median duration of HIV PrEP use during pregnancy was 12.4 weeks (IQR: 8.1,17.0), with participants from the PrIMA-X study reporting the highest median cumulative PrEP use at 20.2 weeks (IQR: 14.4, 27.7). Compared to PrIMA-X (97.9%) and mWACh PrEP (90.4%), the proportion of women in PrIMA still on PrEP at their last pregnancy visit was slightly lower at 84.5%.
Across all cohorts, rates ranged from 1.5-2.7% for stillbirth, 15.1-16.9% for preterm birth, 1.4-3.1% for low birthweight, 9.6-10.1% for low height-for-age Z-score, 2.2-4.6% for low weight-for-age Z-score, 0.4-0.8% for any congenital anomalies, and 1.6-1.7% for neonatal death. Furthermore, there were no significant differences in adverse perinatal outcomes between women without HIV PrEP exposure and any cohort with HIV PrEP exposure (Table 3). Similarly, there were no appreciable differences in the frequency of adverse outcomes by timing of HIV PrEP exposure in pregnancy (Table 4).
Table 3: Birth and neonatal outcomes by HIV PrEP exposure in pregnancy and cohort (n = 3595 from PrIMA; n = 552 from mWACh-PrEP; n = 242 from PrIMA-X).
Table 4: Birth and neonatal outcomes by timing of first HIV PrEP exposure in pregnancy (PrIMA n = 3595; mWACh-PrEP n = 552; PrIMA-X n = 242).
In exploratory analyses, there was no statistically significant association between stillbirth occurrence and the timing of first HIV PrEP exposure (p = 0.976 for the second trimester and p = 0.956 for the third trimester), cumulative HIV PrEP use (p = 0.883), or any HIV PrEP exposure during pregnancy (p = 0.617), compared to no HIV PrEP exposure. Similarly, there was no statistically significant association between the frequency of preterm birth with cumulative HIV PrEP use (p = 0.082) or PrEP exposure in the second trimester (p = 0.930). However, preterm birth was less frequent among those with HIV PrEP exposure in the first trimester (adjusted prevalence ratio[aPR]=0.49, 95% CI 0.42-0.57, p < 0.001) and third trimester (aPR = 0.74, 95% CI 0.61-0.88, p = 0.001), compared to those without any PrEP exposure in pregnancy. Compared to women without HIV PrEP exposure in pregnancy, the frequency of low birthweight was lower among those with any HIV PrEP exposure in pregnancy (aPR = 0.77, 95% CI 0.61-0.97, p = 0.027) and those with HIV PrEP exposure in the third trimester (aPR = 0.74, 95% CI 0.61-0.88, p = 0.001). We did not detect associations between perinatal outcomes and any other HIV PrEP exposure category (Table 5).
Table 5: Association between timing of first HIV PrEP exposure in pregnancy and adverse perinatal outcomes.
Discussion
Our study summarizes safety data for prenatal daily oral HIV PrEP use in ongoing and recently completed studies which include characterization of the timing and duration of HIV PrEP exposure during pregnancy among women in Kenya. Our evaluation contributes novel data from over n = 1300 HIV PrEP-exposed pregnancies across three large studies and found no appreciable differences in the frequency of adverse perinatal outcomes between women with and without HIV PrEP exposure. Specifically, rates of stillbirth, congenital malformations, and neonatal death were comparable across HIV PrEP exposure statuses, with less frequent preterm birth and low birth weight among women with HIV PrEP exposure during pregnancy. These findings are consistent with existing safety data, [3,12,15] and extends the evidence base by including data from women who initiated HIV PrEP prior to pregnancy and during the first trimester. Our findings contribute to the growing body of evidence supporting that prenatal HIV PrEP use appears safe among women initiating HIV PrEP outside of research settings, further solidifying that daily oral HIV PrEP is a safe and effective HIV prevention option for pregnant women.
Most safety studies to date categorize prenatal HIV PrEP exposure as ‘any’ PrEP exposure during pregnancy versus none, without characterizing variance in timing of exposure. Early discontinuation among women who initiate HIV PrEP during pregnancy and sub-optimal HIV PrEP adherence are well-documented in existing HIV PrEP in pregnancy studies, mainly from Kenya and South Africa [25], signaling that true prenatal exposure is likely highly variable. We did not detect differences in adverse perinatal outcomes by any HIV PrEP exposure status or by timing or duration of HIV PrEP exposure. A recent randomized trial in South Africa comparing immediate HIV oral PrEP initiation among pregnant women at 14–28 weeks gestation to women who deferred initiation of HIV PrEP until breastfeeding cessation found no association between HIV PrEP exposure and preterm birth or small for gestational age [3]. Similarly, two recent studies, one from Kenya and one from South Africa, also found that prenatal HIV PrEP exposure confirmed with quantified tenofovir metabolites in dried blood spots was not associated with adverse pregnancy outcomes, [26,27] though the number of confirmed HIV PrEP-exposed pregnancies was limited in both studies. Our findings add to the limited data on perinatal outcomes following well-characterized timing and duration of HIV PrEP exposure. More studies with sample sizes large enough to compare pregnancy outcomes following different timing and duration of HIV PrEP use in pregnancy, ideally with quantified HIV PrEP exposure, would help complete the profile of prenatal HIV PrEP use.
We did not detect differences in most perinatal outcomes among women with periconception or first-trimester HIV PrEP exposure compared to those with no exposure or with exposure at later gestational ages. Few data exist on women who became pregnant while on HIV PrEP and are mostly from early HIV PrEP clinical trials in which participants discontinued HIV PrEP upon becoming pregnant [13], therefore limiting HIV PrEP exposure to a very short period near periconception. One small study (n = 35) of women on HIV PrEP who continued use throughout pregnancy found no association between HIV PrEP and adverse perinatal outcomes [15]. To our knowledge, no prior studies to date compare perinatal outcomes among women who initiate HIV PrEP prior to and during pregnancy. The first trimester is a critical window when substantial fetal growth and development occur [25,28], though limited data are available on pregnancy outcomes following first-trimester HIV PrEP exposure. In contrast to safety evaluations of other antiretroviral drugs which suggested that first-trimester exposure might be linked to adverse outcomes compared to exposure later in pregnancy [29,30], our study found no association between HIV PrEP exposure before pregnancy or during the first trimester and adverse perinatal outcomes. Indeed, we found, among women who initiated PrEP early in pregnancy, lower rates of pre-term birth. This observed association may reflect strong health-seeking behaviors and consistent engagement in antenatal care, which could contribute to improved monitoring and better birth outcomes[31,32]. Similarly, women initiating PrEP in late pregnancy (third trimester) were likely to be highly engaged in care during a critical period for fetal growth and preterm birth prevention. Our results provide reassuring evidence regarding the safety of HIV PrEP use during pregnancy.
Our study has some limitations. The mWACh-PrEP study enrolled pregnant women from 24 weeks gestation and subsequently data from the study cannot evaluate the effect of early HIV PrEP exposure on pregnancy losses prior to 24 weeks. To prevent immortal time bias among PrIMA and PrIMA-X participants and to create a comparable cohort, we only included PrIMA and PrIMA-X participants who had a study visit while still pregnant that occurred 24–32 weeks. Therefore, our sample may have a survivorship bias and we could not evaluate early pregnancy loss across cohorts. Additionally, some variables related to perinatal outcomes (e.g., infant sex, birth length, mode of delivery) were incomplete with differential missingness across studies, which limited the outcomes and adjustment variables available for analysis in the dataset. However, data were mostly complete (<10% missingness) for the primary outcomes included. Furthermore, despite the small number of women initiating PrEP in the first trimester or before pregnancy, we found a relatively high prevalence of preterm birth (~20%) in the study population, which yielded 85% power to detect a 10–percentage point difference in preterm birth between women with first-trimester PrEP exposure and those without PrEP exposure. Lastly, the reliance on self-reported data for HIV PrEP adherence may introduce reporting biases. Despite these limitations, our study contributes descriptive data from a large population of HIV PrEP-exposed pregnancies. Although these findings come from research settings, PrEP delivery in these cohorts occurred within routine antenatal care settings where services followed national Ministry of Health guidelines and were integrated into existing clinical workflows. PrEP initiation, adherence, and discontinuation rates observed were comparable to those in the general pregnant population, supporting the real-world relevance and applicability of our findings for broader implementation. At the time of our evaluation, only daily HIV oral PrEP was available outside of research settings in Kenya and therefore we are unable to describe impact of exposure to other HIV PrEP methods. The prospective design and the inclusion of multiple cohorts also strengthen the validity of our results, adding to a growing pool of safety evidence.
Conclusion
In conclusion, our study found that the frequency of adverse perinatal outcomes was similar among women with and without HIV PrEP exposure during pregnancy, regardless of the timing of HIV PrEP exposure, with lower rates of preterm birth and low birth weight among HIV PrEP-exposed pregnancies. These findings provide reassurance regarding the safety of HIV PrEP use throughout pregnancy and support current guidelines recommending HIV PrEP for pregnant and lactating women at risk of HIV.
Supporting information
S1 FileDe-identified supporting data file for PrIMA, PrIMA-X and mWACh-PrEP.(XLSX)
S2 FileDe-identified supporting data dictionary for PrIMA, PrIMA-X and mWACh-PrEP.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Graybill LA, Kasaro M, Freeborn K, Walker JS, Poole C, Powers KA. Incident HIV among pregnant and breast-feeding women in sub-Saharan Africa: a systematic review and meta-analysis. AIDS. 2020;34(5):761–76.32167990 10.1097/QAD.0000000000002487 PMC 7275092 · doi ↗ · pubmed ↗
- 2Drake AL, Wagner A, Richardson B, John-Stewart G. Incident HIV during pregnancy and postpartum and risk of mother-to-child HIV transmission: a systematic review and meta-analysis. P Lo S Med. 2014;11(2):e 1001608. doi: 10.1371/journal.pmed.1001608 24586123 PMC 3934828 · doi ↗ · pubmed ↗
- 3Moodley D, Lombard C, Govender V, Naidoo M, Desmond AC, Naidoo K, et al. Pregnancy and neonatal safety outcomes of timing of initiation of daily oral tenofovir disoproxil fumarate and emtricitabine pre-exposure prophylaxis for HIV prevention (CAP 016): an open-label, randomised, non-inferiority trial. Lancet HIV. 2023;10(3):e 154–63. doi: 10.1016/S 2352-3018(22)00369-1 36746169 · doi ↗ · pubmed ↗
- 4Birdthistle I, Tanton C, Tomita A, de Graaf K, Schaffnit SB, Tanser F, et al. Recent levels and trends in HIV incidence rates among adolescent girls and young women in ten high-prevalence African countries: a systematic review and meta-analysis. Lancet Glob Health. 2019;7(11):e 1521–40. doi: 10.1016/S 2214-109X(19)30410-3 31607465 PMC 7025003 · doi ↗ · pubmed ↗
- 5Thomson KA, Hughes J, Baeten JM, John-Stewart G, Celum C, Cohen CR. Increased risk of HIV acquisition among women throughout pregnancy and during the postpartum period: a prospective per-coital-act analysis among women with HIV-infected partners. J Infect Dis. 2018;218(1):16–25.29514254 10.1093/infdis/jiy 113PMC 5989601 · doi ↗ · pubmed ↗
- 6Marston M, Risher K, Mahy MI. HIV acquisition in pregnancy: implications for mother-to-child transmission at the population level in sub-Saharan Africa. J Int AIDS Soc. 2021;24(Suppl 5):e 25783. doi: 10.1002/jia 2.25783 34546647 PMC 8454677 · doi ↗ · pubmed ↗
- 7Bekker L-G, Brown B, Joseph-Davey D, Gill K, Moorhouse M, Delany-Moretlwe S, et al. Southern African guidelines on the safe, easy and effective use of pre-exposure prophylaxis: 2020. South Afr J HIV Med. 2020;21(1):1152. doi: 10.4102/sajhivmed.v 21i 1.1152 33354364 PMC 7736681 · doi ↗ · pubmed ↗
- 8Kinuthia J, Pintye J, Abuna F, Mugwanya KK, Lagat H, Onyango D, et al. Pre-exposure prophylaxis uptake and early continuation among pregnant and post-partum women within maternal and child health clinics in Kenya: results from an implementation programme. Lancet HIV. 2020;7(1):e 38–48. doi: 10.1016/S 2352-3018(19)30335-2 31813837 PMC 11498332 · doi ↗ · pubmed ↗