Gallstone Ileus: A Rare Case of Intestinal Obstruction
Joana Rodrigues Ferreira, Tomás Matos Nunes, Madalena Costa, Rafael Carvalho, José Guilherme Cardoso

TL;DR
Gallstone ileus is a rare intestinal blockage caused by gallstones, often in elderly patients, and this case highlights successful treatment through less invasive methods.
Contribution
This paper presents a clinical case emphasizing the effectiveness of less invasive surgical approaches in frail patients with gallstone ileus.
Findings
A longitudinal enterolithotomy and electrohydraulic lithotripsy led to favorable patient outcomes.
Conservative therapy failed in this case, necessitating surgical intervention.
Frail patients can benefit from less invasive procedures with good long-term results.
Abstract
Gallstone ileus is a rare mechanical bowel obstruction caused by the impaction of a gallstone in the GI tract, most frequently in the terminal ileum and the ileocecal valve, secondary to a cholecystoenteric fistula. It predominantly affects elderly women with multiple comorbidities, which, together with non-specific and intermittent symptoms, delay the diagnosis. Imaging studies play a crucial role in diagnosis. Despite that, gallstone ileus continues to be associated with relatively high rates of morbidity and mortality. The optimal management of acute gallstone ileus remains controversial. The selection of a surgical procedure is primarily influenced by the clinical condition. Currently, enterolithotomy remains the most common and safest surgical method, with spontaneous closure of the fistulous tract. One-stage procedure is time-consuming, technically demanding, and is independently…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
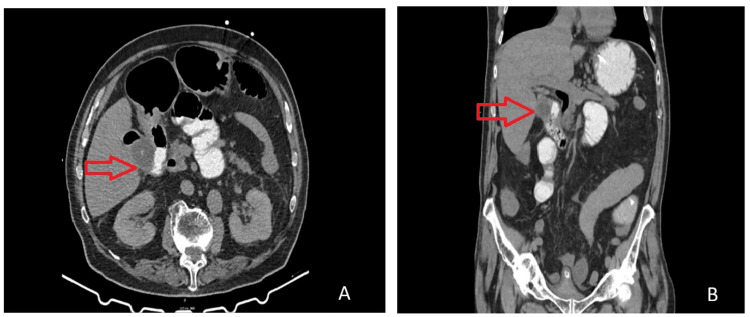 Figure 1
Figure 1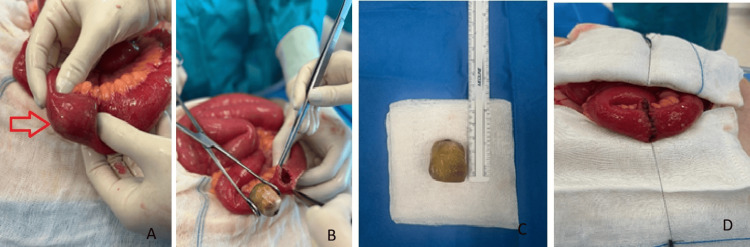 Figure 2
Figure 2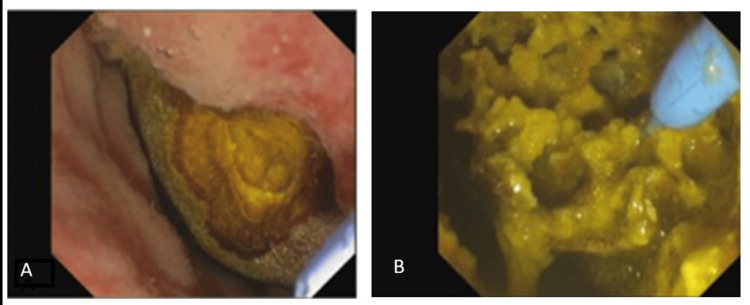 Figure 3
Figure 3| Parameters | Patient values at admission | Patient values in ICU | Reference range |
| Red blood cell count | 5.01 | 4.97 | 4.3-5.9 x 1012/L |
| Hemoglobin | 13.6 | 14.1 | 13.5-17.5 g/dL |
| Hematocrit | 0.413 | 0.456 | 0.406-0.504 |
| Mean corpuscular volume | 82.4 | 80.7 | 80-96 fL |
| Mean corpuscular hemoglobin | 27.1 | 26.7 | 27.3-33.7 pg |
| Mean corpuscular hemoglobin concentration | 329 | 320 | 328-354 g/dL |
| Red cell distribution width | 15.4 | 15 | 11.5-14.5% |
| Platelet count | 148 | 145 | 150-400x 109/L |
| Complete white blood cells | 12.9 | 16.1 | 4-10x109/L |
| Neutrophils | 70.4 | 71 | 40-80% |
| Lymphocytes | 17.9 | 18.2 | 20-40% |
| Monocyte | 11.5 | 11 | 2-11.7% |
| Eosinophils | 0.1 | 1 | 1-6% |
| Basophils | 0.1 | 0.2 | 0-2% |
| Urea | 204 | 196 | 17-49 mg/dL |
| Creatinine | 5.53 | 6.68 | 0.7-1.2 mg/dL |
| Albumin | 3.2 | 2.9 | 3.5-5.2 g/dL |
| Bilirubin total | 0.4 | 0.42 | <1.4 mg/dL |
| Sodium | 132 | 130 | 136-145 mmol/L |
| Potassium | 4.8 | 5.38 | 3.5-5.1 mmol/L |
| Chloride | 90 | 101 | 98-107 mmol/L |
| Calcium | 7.8 | 7.9 | 8.8-10.2 mg/dL |
| Phosphorus | 5.4 | 4.4 | 2.5-4.5 mg/dL |
| Magnesium | 2.5 | 2.1 | 1.6-2.4 mg/dL |
| C-reactive protein | 21.5 | 29.7 | <0.5 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiliary and Gastrointestinal Fistulas · Gallbladder and Bile Duct Disorders · Diverticular Disease and Complications
Introduction
Gallstone ileus refers to a mechanical obstruction of the bowel resulting from the entrapment of a gallstone in the GI tract, secondary to a cholecystoenteric fistula [1,2]. It is an uncommon yet significant complication of cholelithiasis, representing 1-4% of all causes of intestinal obstruction [1,3]. Gallstone ileus is more common in elderly women with multiple comorbidities, which, together with non-specific and intermittent symptoms, delays the diagnosis [3,4]. As a consequence, gallstone ileus is still correlated with relatively high levels of morbidity and mortality [3,4]. The optimal management of gallstone ileus remains controversial [5]. We report a rare case of gallstone ileus, without symptom recurrence after a successful surgical treatment with enterolithotomy alone.
Case presentation
An 84-year-old male patient, partially dependent, with hypertension, previously submitted to bilateral inguinal hernioplasty and radical prostatectomy, was brought to the ER due to a four-day history of vomiting with fecaloid content, food intolerance, and epigastric abdominal pain, with no changes in his bowel habits.
On physical examination, he demonstrated hemodynamic stability, exhibiting signs of dehydration. The abdomen was distended, presenting diffuse pain upon deep palpation, without signs of peritoneal irritation on percussion. Digital rectal examination was unremarkable. Laboratory tests revealed leukocytosis, acute kidney injury of probable prerenal etiology, electrolyte disturbances (hyponatremia and hyperkalemia), and elevated C-reactive protein (Table 1).
Abdominal X-ray showed air-fluid levels. He underwent a non-contrast computed tomography (CT) of the abdomen that showed a diffuse dilation of the small bowel with a non-obstructive hyperdense image in the lumen of the third duodenal portion. A 5-mm cholecystoenteric fistula between the gallbladder fundus and the second portion of the duodenum was identified. Additionally, it was associated with extensive pneumobilia and a transition point in the mesentery with an abrupt reduction of bowel caliber.
The patient underwent gastrografin, with apparent progression of the contrast agent without evident stoppage. Initially, conservative therapy was chosen, and empirical antibiotic therapy was initiated. He remained under surveillance in the ICU, presenting continuous biliary drainage of approximately 1000 mL/24 hours and progressive worsening of inflammatory markers on Day 2 (Table 1). A repeat abdominal CT scan with oral contrast revealed the absence of contrast progression, consistent with mechanical small bowel obstruction due to gallstone ileus and possible ischemic involvement (Figure 1).
Axial and coronal section of simple abdominal CTRepeat CT shows diffuse dilation of the small bowel with a cholecystoenteric fistula between the gallbladder fundus and the second duodenal portion (red arrow)
During the exploratory laparotomy, dilated intestinal loops were found 100 cm from the ileocecal valve, without signs of ischemia. An inflammatory mass was visible in the region of the hepatic and gallbladder hilum, so, given the clinical condition, it was decided not to approach the area. A longitudinal enterotomy in the antimesenteric border was performed, leading to the extraction of an approximately 2.5 cm stone that occluded the intestinal lumen entirely, without vascular compromise (Figures 2A-2C). Subsequently, a two-layer closure with absorbable sutures was performed (Figure 2D). Further investigation of the intestine and colon was conducted, yet no further stones were identified.
Intraoperative findings(A) Dilated bowel loop with stone inside (red arrow), with no signs of ischemia. (B) Longitudinal enterotomy with stone extraction. (C) 2.9 x 2.6 cm stone. (D) Enterorrhaphy with absorbable suture in two planes
During hospitalization, an upper gastrointestinal endoscopy was performed, revealing a cholecystoduodenal fistula in the proximal second portion of the duodenum, with a large stone protruding into the duodenal lumen and reducing its size (Figure 3). Electrohydraulic lithotripsy was tried, which allowed the fragmentation of the 3 cm stone (two-thirds of the total volume by visual estimation).
Upper gastrointestinal endoscopy and electrohydraulic lithotherapyUpper gastrointestinal endoscopy that revealed the cholecystoduodenal fistula with a large stone protruding into the duodenal lumen (A), and electrohydraulic lithotherapy (B) was performed which allowed the fragmentation of the stone
The patient progressed favorably, tolerated diet progression while maintaining intestinal transit, and was discharged home on the seventh postoperative day. At the medical consultation, he tolerated a low-fat diet, without any new episodes of biliary colic or intestinal obstruction. Six months postoperatively, he underwent a reassessment CT abdominal scan that highlighted persistent parietal hyperemia of the bile ducts associated with pneumobilia, suggesting a persistent fistula, without associated gallstones or changes in caliber or uptake in the small intestine or colon.
Discussion
Gallstone ileus is a rare but serious complication of cholelithiasis, often preceded by an episode of cholecystitis, in which the inflammation leads to the formation of a fistula to the adjacent GI tract. Gallstone ileus can also arise as a complication of an endoscopic retrograde cholangiopancreatography or an endoscopic sphincterotomy [6], and the consequence of loose stones in the abdominal cavity after a laparoscopic cholecystectomy [5]. The gallstone must be superior to 2-2.5 cm in diameter to cause obstruction, typically found in the terminal ileum and the ileocecal valve as a result of their constricted lumen and potentially diminished peristalsis activity (60.5% of cases) [7,8].
Presentation is typically non-specific, with vague, intermittent symptoms, generally associated with an advanced age and several comorbidities, and may be the result of a delay in diagnosis [8]. Without early treatment, the patient will progress with ischemia and subsequent perforation and peritonitis, with a mortality of 12-27% [5]. Imaging studies have a crucial role in diagnosis, especially with the widespread use of CT. Plain radiographic findings, such as pneumobilia, dilated loops, and ectopic stone (Rigler’s triad) are only observed in 15% of cases [9,10].
There is no consensus on the best approach and surgical procedure, and the management of gallstone ileus remains controversial. There are several approaches described in the literature: (i) conservative treatment with nasogastric decompression; (ii) enterolithotomy or bowel resection alone; (iii) one-stage surgery: enterolithotomy, cholecystectomy, and fistula closure; (iv) two-stage surgery: delayed cholecystectomy and fistula closure four to six weeks after enterolithotomy [7,11,12]. In over 50% of cases, the fistulous tract undergoes spontaneous closure [11].
The determination of the surgical procedure is predominantly based on the clinical status, usually prioritizing techniques that are less invasive. Currently, enterolithotomy remains the most common and safest surgical method, with a low incidence of complications and low morbidity and mortality [11,13]. In the presence of residual stones, 5% of patients go on to develop biliary symptoms within six months of the index presentation, and there is a potential risk of patent fistula reflux resulting in biliary malignancy [8,11,14]. Laparoscopy-assisted methods have been described; however, they are technically more demanding [15]. Additionally, there are cases reported in the literature of endoscopic extraction, like in Bouveret’s syndrome [16]. One-stage procedure is time-consuming, technically demanding, and was independently associated with a higher prevalence of mortality [17]. Delayed cholecystectomy should be reserved only in cases of symptom persistence.
Conclusions
Gallstone ileus is a rare entity that exhibits a gradual onset with unclear signs and symptoms. For that reason, accurate diagnosis is crucial, and a significant clinical suspicion is needed when there is a documented history of acute or recurring cholecystitis. Taking into account the advanced age and comorbidities of most patients, relief of obstruction by enterolithotomy alone in the emergency setting is recommended. One-stage procedure has a number taking more time, being more technically challenging, and being associated with a higher prevalence of mortality. Delayed cholecystectomy should be reserved only in cases of symptom persistence. This case highlights the importance of opting for less invasive approaches in frail patients with good long-term results.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gallstone ileus: management and clinical outcomes Medicina (Kaunas) Jakubauskas M Luksaite R Sileikis A Strupas K Poskus T 5985520193153329510.3390/medicina 55090598 PMC 6780297 · doi ↗ · pubmed ↗
- 2Gallstone ileus analysis of radiological findings in 27 patients Eur J Radiol Lassandro F Gagliardi N Scuderi M Pinto A Gatta G Mazzeo R 23295020041509323210.1016/j.ejrad.2003.11.011 · doi ↗ · pubmed ↗
- 3Gallstone ileus of the sigmoid colon caused by cholecystocolonic fistula: a case report Ann Med Surg (Lond) Mauricio GU David Eugenio HG Enrique QF 25283120182992246410.1016/j.amsu.2018.06.001PMC 6004734 · doi ↗ · pubmed ↗
- 4Gallstone ileus 1 year after cholecystectomy J Surg Case Rep Teelucksingh S Boppana LK Goli S Naraynsingh V 02018201810.1093/jscr/rjy 153PMC 603101029992006 · doi ↗ · pubmed ↗
- 5Gallstone ileus: a review BMJ Open Gastroenterol Inukai K 06201910.1136/bmjgast-2019-000344 PMC 690416931875141 · doi ↗ · pubmed ↗
- 6Gallstone ileus following endoscopic stone extraction Case Rep Gastrointest Med Yamauchi Y Wakui N Asai Y 271571201420142532872510.1155/2014/271571 PMC 4195353 · doi ↗ · pubmed ↗
- 7Gallstone ileus. Review of 112 patients in the Japanese literature Am J Surg Kasahara Y Umemura H Shiraha S 4374401401980742522010.1016/0002-9610(80)90185-3 · doi ↗ · pubmed ↗
- 8Gallstone ileus: a review of 1001 reported cases Am Surg Reisner RM Cohen JR 441446601994 https://pubmed.ncbi.nlm.nih.gov/8198337/8198337 · pubmed ↗