Antimicrobial susceptibility testing of Aggregatibacter Actinomycetemcomitans can be performed using the EUCAST medium for anaerobic bacteria
Anne Birkeholm Jensen, Erika Matuschek, Gunnar Kahlmeter, Niels Nørskov-Lauritsen

TL;DR
This study shows that EUCAST guidelines can be used to test antibiotic susceptibility of Aggregatibacter actinomycetemcomitans using FAA-HB agar and 20-hour incubation in 5% CO₂.
Contribution
The study demonstrates that EUCAST methods can be adapted for AST of A. actinomycetemcomitans, supporting future standardization.
Findings
FAA-HB agar supports sufficient Aa growth after 20 hours in 5% CO₂.
Incubation in 5% CO₂ yields better results than anaerobic conditions.
20-hour incubation provides reproducible results for AST.
Abstract
The oral bacterium Aggregatibacter actinomycetemcomitans (Aa) is associated with infectious diseases treated with antibiotics, but specific recommendations for antimicrobial susceptibility testing (AST) of the species do not yet exist. Objective To evaluate the possibility to perform AST of Aa following EUCAST guidelines using FAA-HB and 20 h incubation. Twenty-nine Aa strains were analysed using disk diffusion on FAA-HB media from three manufacturers. Plates with with ampicillin and azithromycin disks were incubated in 5% CO2 and anaerobic conditions and examined after 20 and 44 h. Strains were additionally tested with the agar dilution method, and inhibition zone diameters (IZD) were correlated to the minimal inhibitory concentrations. FAA-HB agar supported sufficient growth of Aa after 20 h incubation in 5% CO₂. No significant differences in IZD were found between the three media…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
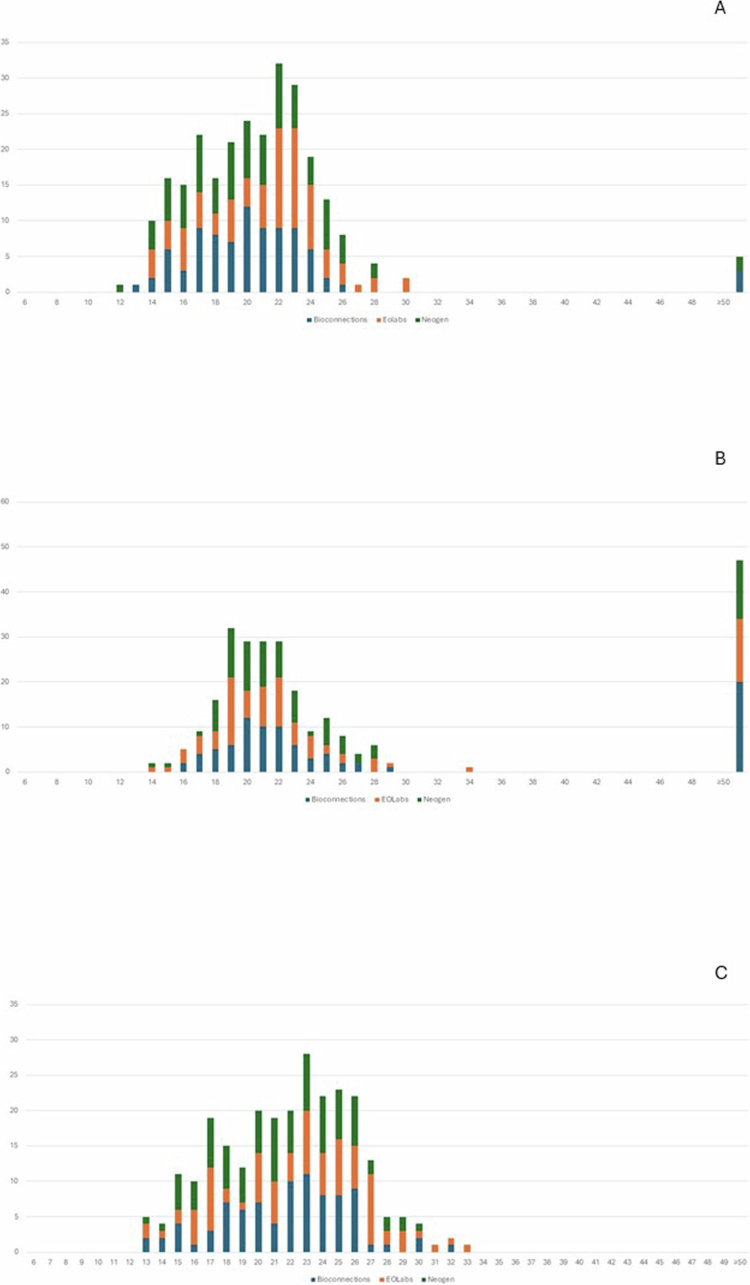 Figure 1
Figure 1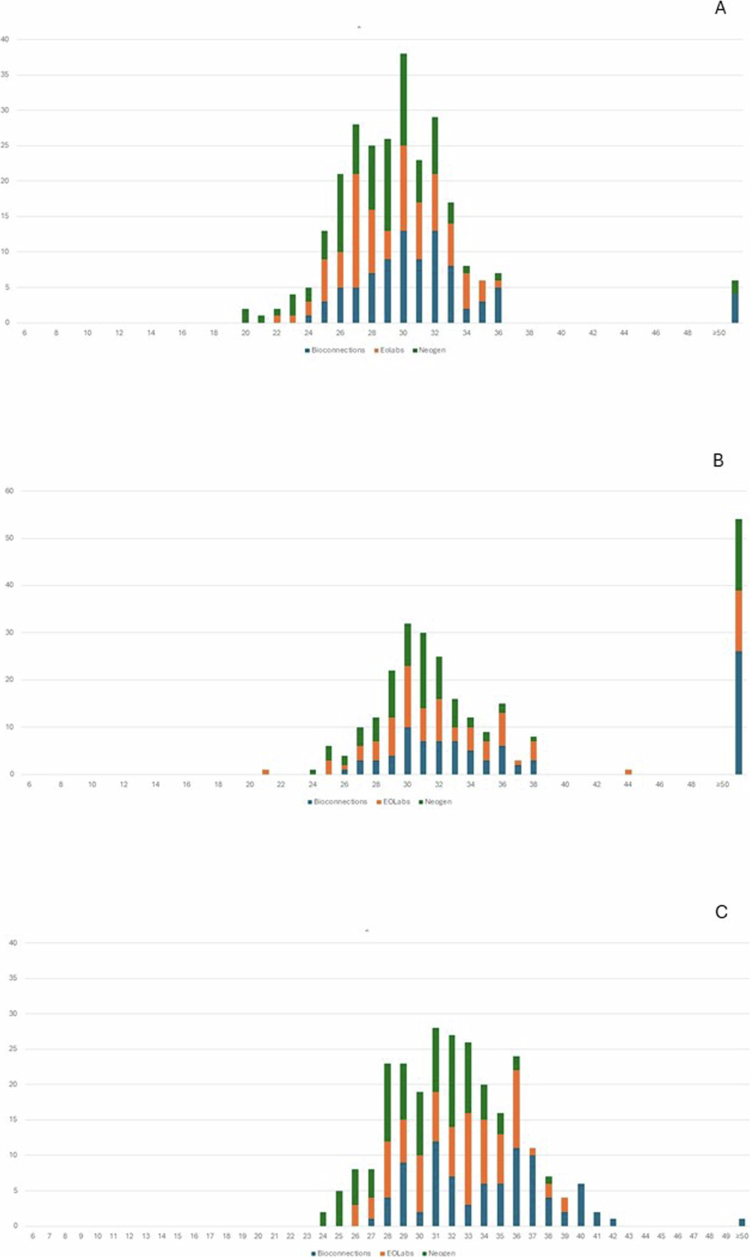 Figure 2
Figure 2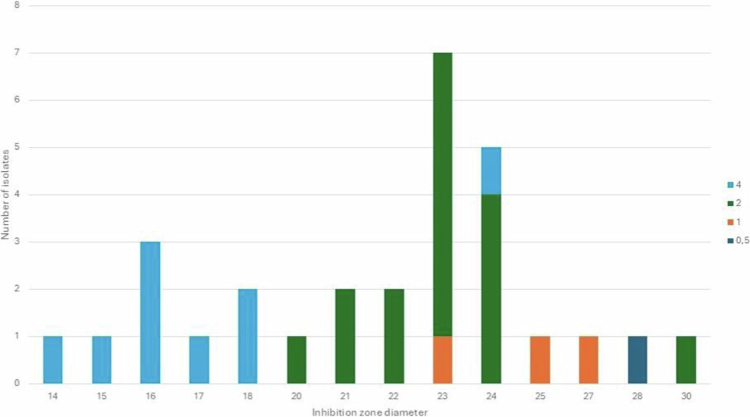 Figure 3
Figure 3| Isolate | Origin | Reference (year) |
|---|---|---|
| ATCC 33384T | Oral abscess | Klinger (1912) |
| ATCC 43718/HK 975/Y4 | Subgingival plaque | Klinger (1912) |
| ATCC700685/CCUG 56173/HK 1651 | Periodontitis | J. Westergård, Denmark (1996) |
| CCUG 51668/HK 929 | Dental plaque | S. Asikainen, Finland (before 1992) |
| CCUG 51667/HK 928 | Dental plaque | S. Asikainen, Finland (before 1992) |
| CCUG 56172/HK 921/JP2 | Periodontitis | C.C. Tsai, USA (1984) |
| C100 | Unknown | R. Clasesson, Sweden |
| Unknown | R. Claesson, Sweden | |
| D7ss | Oral isolates | Y. Wang, USA (-) |
| HK 907 | Periodontitis | T.M.J van Steenbergen, the Netherlands |
| HK 909, HG1080 | Unknown | Denmark (1990s) |
| HK 1613 | Periodontitis | DiRienzo, USA (1990s) |
| HK 1615 | Periodontitis | DiRienzo, USA (1990s) |
| PN604 | Periodontitis | A.J. van Winkelhoff, the Netherlands (2000s) |
| PN603 | Periodontitis | A.J. van Winkelhoff, the Netherlands (2000s) |
| PN385 | Unknown | N. Nørskov-Lauritsen, Denmark (-) |
| RRI 700 541/UK11 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 542/UK7 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 543/UK42 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 544/UK21 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 545/UK44 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 546/UK48 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 547/UK4 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 548/UK46 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 549/UK14 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 550/UK1 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 551/UK17 | Periodontitis | D. Ready, UK (before 2017) |
| RRI 700 552/UK12 | Periodontitis | D. Ready, UK (before 2017) |
| 524 G | Oral isolate | D. Haubek/A. Johansson, Ghana (2009) |
| Antibiotic disk | Bioconnection | Neogen | EO Labs |
|---|---|---|---|
| Ampicillin | 19.8 (3) | 20.1 (3.8) | 21.1 (3.5) |
| Azithromycin | 30.4 (2.9) | 28.3 (3.1) | 29.3 (3.2) |
| Antibiotic disk | 5% CO2, 20 h | 5% CO2, 44 h | Anaerobic, 20 h | Anaerobic, 44 h |
|---|---|---|---|---|
| Ampicillin | 20.32 (3.5) | 21.9 (4.2) | 21.3 (3.3) | 23.5 (3.8) |
| Azithromycin | 29.3 (3.2) | 32.3 (4.3) | 32.3 (12.3) | 34.8 (4.7) |
- —Riisfort Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Identification and Susceptibility Testing · Orthopedic Infections and Treatments · Actinomycetales infections and treatment
Introduction
is a Gram-negative, non-motile, facultative anaerobic bacterium that grows well on enriched media in ambient air supplemented with 5% CO_2_. A. actinomycetemcomitans appears as small, rough colonies 0.5 mm in diameter after approximately 24 h, although some strains may need 48 h for sufficient growth [1]. A. actinomycetemcomitans is a member of the oral microbiota but can cause severe infections when introduced in otherwise sterile compartments of the human body, e.g. brain abscess and infectious endocarditis [1–4]. A. actinomycetemcomitans is also associated with severe periodontitis in young individuals, currently categorised as Grade C Molar-Incisor pattern periodontitis [5–7]. Studies have reported difficulties in eliminating this bacterium from the periodontal pockets of periodontitis patients by debridement only, and treatment with antibiotics may be needed in some cases [5,8,9]. Based on clinical studies, the recommended antibiotic regimen in the treatment of periodontitis is amoxicillin plus metronidazole, which targets a broad spectrum of the oral microbiota. In the presence of β-lactam resistance or allergy to penicillin, azithromycin is the best choice [10].
Antimicrobial susceptibility testing (AST) of A. actinomycetemcomitans is important for guidance of treatment and for surveillance of antimicrobial resistance. Several studies have reported on the antimicrobial susceptibility of A. actinomycetemcomitans, but the studies differ in methodology, e.g. incubation (anaerobic vs. aerobic), timeframe for reading of plates, inoculum size, interpretation (breakpoints), and the media used [11–15]. Guidelines for determination of minimal inhibitory concentration (MIC) are available for the HACEK group (including A. actinomycetemcomitans) by CLSI (Clinical Laboratory Standard Institute), hitherto, the European Committee for Antimicrobial Susceptibility Testing (EUCAST) criteria for AST of A. actinomycetemcomitans have not been developed. EUCAST recommends Mueller Hinton agar supplemented with defibrinated horse blood and beta-NAD (MH-F) for disk diffusion of fastidious microorganisms [16,17], but A. actinomycetemcomitans grows insufficiently on MH-F with 5% horse blood for AST [12]. Also, MIC determination with broth microdilution in MH-F broth, as recommended by EUCAST for most fastidious organisms, does not support sufficient growth of A. actinomycetemcomitans (data not published).
Due to insufficient growth of anaerobes on MH-F agar, EUCAST investigated fastidious anaerobe agar supplemented with 5% mechanically defibrinated horse blood (FAA-HB) for AST of anaerobic bacteria [18,19], and currently recommends MIC method for anaerobic bacteria is agar dilution on FAA-HB [20,21]. The aim of this study was to evaluate if FAA-HB agar plates can support sufficient growth of A. actinomycetemcomitans in 20 h, which would suggest a possible use of this medium for AST of A. actinomycetemcomitans within mandatory EUCAST criteria. We addressed FAA-HB from three manufacturers (designated ‘biological replicates’), performed incubation in anaerobic and CO_2_-enriched atmospheres, and evaluated antimicrobial action of ampicillin and azithromycin with both disk diffusion and agar dilution.
Materials and methods
Study isolates and quality control strains
Twenty-nine A. actinomycetemcomitans strains were selected for AST (Table 1). All strains were identified to species level with MALDI-TOF [12]. The strains were subcultured in 5% CO_2_ at 35 ± 1 °C twice before being used for AST, and the strains were used for AST after 48 h of incubation. A. actinomycetemcomitans (ATCC 43718), Clostridium perfringens (ATCC 13124), and Bacteroides fragilis (ATCC 25285) were used for quality control.
AST by disk diffusion
The disk diffusion method was carried out according to EUCAST guidelines and the 15-15-15 rule [16,22] on in-house prepared FAA-HB using FAA from three manufacturers (Bioconnections (BioConnections, Brindley Court Knypersley, UK), Neogen (NEOGEN, Heywood, BL9 7JJ, UK), and EO Labs (E&O Laboratories Ltd., Burnhouse, Bonnybridge, Scotland). Antibiotic disks with 2 µg ampicillin (Oxoid/Thermo Fischer Scientific, Basingstoke, UK) and 15 µg azithromycin (Oxoid/Thermo Fischer Scientific, Basingstoke, UK) were tested. Plates were incubated in 5% CO_2_ at 35 ± 1 °C and anaerobically (80% N_2_, 10% CO_2_, 10% H_2_) (Whitley A35 anaerobic workstation, West Yorkshire, UK) at 35 ± 1 °C and visually inspected after 16–20 h and after 40–44 h. The quality (paleness and richness of growth) and confluence of growth, the appearance of zone edges, and the ease with which the zone diameter could be measured were evaluated according to EUCAST criteria [23]. The tests were performed in triplicate.
MIC determination by the agar dilution method
Stock solutions of ampicillin and azithromycin (European Pharmacopoiea Reference Standard, Sigma-Aldrich, Germany) were prepared at a concentration of 1000 mg/L. Ampicillin stock solution was prepared in 0.1 M phosphate buffer, pH 8.0, and azithromycin in 95% ethanol [20,24]. Agar dilution plates were prepared as described by EUCAST [20]. Briefly, medium for FAA-HB plates (E&O Laboratories Ltd., Burnhouse, Bonnybridge, Scotland) was supplemented with 5% defibrinated horse blood and various concentrations of antibiotics. McFarland suspensions of 0.5 were prepared in sterile saline (0.9%) from plates with bacteria cultured for 48 h. The suspensions were diluted 10 times, equivalent to a concentration of 10^7^ colony-forming units (CFU) per ml. One microliter (approximately 10^4^ CFU) was inoculated onto the agar plates using a Denley Multipoint Inoculator.
Each assessment was composed of nine plates with two-fold dilutions of antibiotic (range 0.0625–16.0 mg/L) plus two control plates without added antibiotic. Plates were incubated in 5% CO_2_ at 35 ± 1 °C and visually inspected after 20 h. MIC values were defined as the lowest concentrations of the antimicrobial agent that inhibited visible growth, disregarding a single colony or a thin haze at the inoculated spot (EUCAST & ESCMID, 2000). All tests were performed in triplicate, and the median MIC were used for further analysis.
Data analysis
Data analysis was performed using Excel and GraphPad Prisms 10.4.0 (621). Media comparison under the different incubation forms and interval was done by use of a two-way ANOVA. The difference in mean inhibition zone diameter from the different incubation forms and intervals was calculated using the Wilcoxon matched pairs signed rank test for non-parametric data and a non-paired t-test for parametric data. The correlation between inhibition zone diameter and MIC was calculated by use of a simple linear regression model.
Results
Disk diffusion
FAA-HB media from the three manufacturers resulted in confluent growth for 259 of 261 measurements (99%) of the 29 study strains after 20 h incubation in 5% CO_2_, and for all investigated organisms after 44 h in 5% CO_2_ (Table S1). Under anaerobic incubation, 235 (90%) measurements showed confluent growth after 20 h and 253 (97%) after 44 h. The mean difference of the inhibition zone diameter obtained on the three media was not statistically significant (p > 0.05), and the zone diameters were similar (Figures 1 and 2 and Table 2). The difference in mean inhibition zone diameters obtained on FAA-HB from three manufactures were under 2 mm, except for Bioconnection and Neogen on the azithromycin disk where the difference reached 2.1 mm (Table 2). By visual inspection of Figures 1 and 2, media from EOlabs performed superior to the other two media after 20 h incubation in 5% CO_2_, since all strains exhibited visible growth. The media from Bioconnection resulted in more growth failures after 20 h in anaerobic incubation (Table S1). However, the difference between the media was not statistically significant (p > 0.05).
Overall, the strains grew sufficiently after 20 h of incubation in 5% CO_2_ for reproducible interpretation of inhibition zone diameters (Table S1). More specifically, all strains showed confluent growth on EOLabs, whereas one strain resulted in semi-confluent growth on Bioconnection and Neogen. Under anaerobic incubation, a considerable number of strains needed prolonged incubation for 44 h to reach confluent growth ([Figures 1B–2B](#f0001 f0002) and Table S1). Prolonged incubation for 44 h in 5% CO_2_ resulted in confluent growth of all strains, but with a statistically significant larger mean inhibition zone diameters compared to incubation for 20 h only (p < 0.05) ([Figures 1C–2C](#f0001 f0002) and Table 3). Prolonged incubation in the anaerobic chamber also showed a tendency of increased inhibition zone diameters, especially for azithromycin (Table 3).
Inhibition zone diameters for ampicillin and A. actinomycetemcomitans on FAA-HB from Bioconnection, Neogen and EOLabs (261 readings). A) 5% CO2, 20 h incubation B) Anaerobic chamber, 20 h incubation C) 5% CO2, 44 h incubation. Number of isolates (y-axis) with a certain inhibition zone diameter (x-axis) obtained on media prepared from FAA from three different manufacturers. No significant difference was observed among the FAA-HB manufacturers. The different FAA media are represented by colours. Blue columns: Bionnections; orange columns: EOLabs; green columns: Neogen. The last column to the right shows strains showing no growth (failure).
Inhibition zone diameters for azithromycin and A. actinomycetemcomitans on FAA-HB from Bioconnection, Neogen and EOLabs (261 readings). A) 5% CO2, 20 h incubation B) Anaerobic chamber, 20 h incubation C) 5% CO2, 44 h incubation. Number of isolates (y-axis) with a certain inhibition zone diameter (x-axis) obtained on media prepared with FAA from three different manufacturers. No significant difference was observed among the FAA-HB manufacturers. The different FAA media are represented by colours. Blue columns: Bionnections; orange columns: EOLabs; green columns: Neogen. The last column to the right shows strains showing no growth (failure).
The quality of the growth, determined by the confluence and richness of the growth and the number of strains readable after 20 h, was superior with incubation in 5% CO_2_compared to incubation in anaerobic chamber (Table S2).
Based on the overall summary of the results, incubation in 5% CO_2_ and reading after 20 h resulted in the best correlation between the three different media.
Correlation between inhibition zone diameters and MICs
Figure 3 shows the distribution of MIC in relation to the correlating inhibition zone diameter. Based on the linear regression analysis, the correlation between the MIC and inhibition zone diameters with ampicillin and 20 h incubation in 5% CO_2_ was acceptable demonstrated by a r^2^ of 0.66 (p < 0.001). For the azithromycin disk, the correlation was poor with an r^2^ 0.36 (p < 0.0056). With some exceptions, Figure 3 shows that strains determined with an MIC of 4 mg/L were more likely to have smaller inhibition zone diameters, and strains determined with an MIC of 1 or 0.5 mg/L had inhibition zone diameters above 22 mm. More specifically, eight of nine isolates with a MIC of 4 mg/L exhibited zones ≤ 19 mm, while all isolates with a MIC ≤ 2 mg/L exhibited zones > 19 mm.
Correlation of inhibition zone diameters for ampicillin and MICs. Inhibition zone diameter distribution for A. actinomycetemcomitans and ampicillin 2 µg with corresponding MIC values as coloured bars. Results from incubation in 5% CO2 for 20 h. Number of isolates (y-axis) with an inhibition zone diameter (x axis; mm) and correlating MIC (colour-coded columns). The correlation observed between the MIC and inhibition zone diameters was acceptable. Blue columns: isolates with an MIC of 4 mg/L; green columns: isolates with an MIC of 2 mg/L; orange columns: isolates with an MIC of 1 mg/L; dark blue columns: isolates with an MIC of 0.5 mg/L.
Discussion
We have demonstrated that the anaerobic FAA-HB agar is useful for AST with the disk diffusion method of A. actinomycetemcomitans and incubation in 5% CO_2_. Only 5 of 261 (2%) measurements failed to sustain sufficient growth for visible evaluation, in contrast to 18% failures after anaerobic incubation on the same media. This medium consistently yielded confluent growth with similar inhibition zone diameters after 20 h incubation in air with 5% CO_2_, providing a robust and dependable method for AST of A. actinomycetemcomitans.
The strains showed excellent growth on FAA-HB from three manufacturers, and the difference in inhibition zone diameters obtained with the different FAA-HB was acceptable because the mean difference in inhibition zone diameters were two millimetres or less and did not reach statistical significance. The capnophilic species, A. actinomycetemcomitans, grows well in air with 5% CO_2_, but we additionally tested the species with anaerobic incubation because FAA-HB is a media developed for testing of anaerobic species and performs well under anaerobic conditions [18].
The results obtained for this species, and the disk diffusion method were most promising with the use of ampicillin compared to azithromycin. Clinical studies recommend the use of amoxicillin and metronidazole for the treatment of A. actinomycetemcomitans-associated periodontitis, and the acceptable correlation between the MIC and the inhibition zone diameter on the ampicillin disk makes our results promising for future treatment planning [10].
We need additional data to establish epidemiological cut-off values (ECOFFs) for A. actinomycetemcomitans, which will be an important part of the breakpoint setting procedure by EUCAST [25]. ECOFFs apply to individual species only. Applying ECOFFs or clinical breakpoints for systemic pathogens to oral species may yield unreliable antibiotic susceptibility interpretations. Therefore, developing ECOFFs or clinical breakpoints for relevant oral species will improve antibiotic selection for the treatment of oral infections. Our strain population showed a reasonable distribution of inhibition zone diameters and MICs, and considering Aggregatibacter to be resistant to ampicillin goes against clinical guidelines and empirical use of ampicillin/amoxicillin in the treatment of Aggregatibacter-associated diseases [10]. Previously, 27 of the 29 study strains examined in the present study were categorised with a one two-fold dilution step lower amoxicillin MICs using blood agar and 44 h incubation. Precisely the media and incubation time may be a plausible explanation for the difference between the results. However, our results emphasise the importance of following the criteria and guidelines provided by, e.g. EUCAST, to get reliable results, and the correlation between inhibition zone diameter and MIC should be tested on a larger strain collection.
Previous studies have reported difficulties with haze zones within the inhibition zones [12]. In the present study, we did not experience such haze zones, and overall, the inhibition zone diameters were easy to interpret with clear edges. However, the recommendation by EUCAST concerning the handling of plates, e.g. using over-night dried plates with room temperature, was strictly followed in the present study, which may have eliminated haze zones due to humidity.
Some limitations of the present study should be acknowledged. We cannot categorise any of the study strains as resistant or susceptible due to the lack of clinical breakpoint for this species. In addition, the small strain collection calls for future studies testing the method on a larger strain collection that includes resistant strains and additional antimicrobial agents.
The disk diffusion method is considered a reproducible and sustainable method for AST [16]. Standardising the method for A. actinomycetemcomitans would improve the differentiation between wild-type strains (strains without phenotypically detectable resistance mechanisms) and non-wild-type strains (strains with phenotypically detectable resistance mechanisms) within this species in clinical settings [26]. There is a need for reproducible, easy, and available methods for AST of oral pathogens that cause disease both intra- and extra-orally [27]. Standardised AST of oral strains will ensure reproducible and comparable results that clinically benefit patients, clinicians, and society both concerning treatment planning and surveillance of the development of antimicrobial resistant in members of the oral microbiota. The lack of reproducibility of previous published results emphasises the importance of establishing criteria and guidelines for AST of oral pathogens like A. actinomycetemcomitans. The EUCAST disk diffusion method and FAA-HB is feasible for this purpose, and the results of the present study prepare the ground for further standardising the disk diffusion method for A. actinomycetemcomitans and encourage future studies aiming at developing clinical breakpoints.
Supplementary Material
Table_Suppl.docxSupplemental Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nørskov-Lauritsen N, Claesson R, Birkeholm Jensen A, et al. Aggregatibacter actinomycetemcomitans: clinical significance of a pathobiont subjected to ample changes in classification and nomenclature. Pathogens. 2019;8(4):243. doi: 10.3390/pathogens 804024331752205 PMC 6963667 · doi ↗ · pubmed ↗
- 2Rahamat-Langendoen JC, van Vonderen MG, Engström LJ, et al. Brain abscess associated with Aggregatibacter actinomycetemcomitans: case report and review of literature. J Clin Periodontol. 2011;38(8):702–706. doi: 10.1111/j.1600-051X.2011.01737.x 21539594 · doi ↗ · pubmed ↗
- 3Khaledi M, Sameni F, Afkhami H, et al. Infective endocarditis by HACEK: a review. J Cardiothorac Surg. 2022;17(1):185. doi: 10.1186/s 13019-022-01932-535986339 PMC 9389832 · doi ↗ · pubmed ↗
- 4Goeteyn E, Taylor SL, Dicker A, et al. Aggregatibacter is inversely associated with inflammatory mediators in sputa of patients with chronic airway diseases and reduces inflammation in vitro. Respir Res. 2024;25(1):368. doi: 10.1186/s 12931-024-02983-z 39395980 PMC 11471032 · doi ↗ · pubmed ↗
- 5Miguel MMV, Shaddox LM. Grade C molar-incisor pattern periodontitis in young adults: what have we learned so far?. Pathogens. 2024;13(7):580. doi: 10.3390/pathogens 1307058039057807 PMC 11279578 · doi ↗ · pubmed ↗
- 6Dahlén G, Claesson R, Aberg CH, et al. Subgingival bacteria in Ghanaian adolescents with or without progression of attachment loss. J Oral Microbiol. 2014;6:23977. doi: 10.3402/jom.v 6.23977 PMC 401348924834145 · doi ↗ · pubmed ↗
- 7Haubek D, Ennibi OK, Poulsen K, et al. Risk of aggressive periodontitis in adolescent carriers of the JP 2 clone of Aggregatibacter (Actinobacillus) actinomycetemcomitans in Morocco: a prospective longitudinal cohort study. Lancet. 2008;371(9608):237–242. doi: 10.1016/S 0140-6736(08)60135-X 18207019 · doi ↗ · pubmed ↗
- 8Burgess DK, Huang H, Harrison P, et al. Non-surgical therapy reduces presence of JP 2 Clone in localized aggressive periodontitis. J Periodontol. 2017;88(12):1263–1270. doi: 10.1902/jop.2017.17028528820321 PMC 5700858 · doi ↗ · pubmed ↗