Functional capacity in sickle cell disease: A pilot study with 1-minute sit-to-stand test
Michele Barroso Thomaz, Lucas Fernandes Suassuna, Júlia Campos Fabri, Isabela de Oliveira Araújo, Júlia Carneiro Almeida, Daniela de Oliveira Werneck Rodrigues

TL;DR
This study explores how a simple one-minute sit-to-stand test can assess functional capacity in sickle cell disease patients, linking it to quality of life.
Contribution
The study introduces the one-minute sit-to-stand test as a practical tool for evaluating functional capacity in sickle cell disease.
Findings
The one-minute sit-to-stand test correlates with quality of life in sickle cell disease patients.
Most participants were Black or mixed race, and the majority had hemoglobin SS genotype.
Hydroxyurea was the most common treatment among participants.
Abstract
Sickle cell disease, the most prevalent monogenic recessive genetic disorder in the world, is characterized by two main pathogenic mechanisms: vaso-occlusion and hemolysis. These characteristics lead to reduced tolerance to physical exertion and, consequently, a reduced functional capacity which can be assessed using the one-minute sit-to-stand test. Complications from sickle cell disease result in poor quality of life, increased absenteeism from school and work, and impaired social interaction. Between January 2023 and April 2024, a pilot cross-sectional study was conducted with sickle cell disease patients aged from 18 to 60 years. The one-minute sit-to-stand test, Borg's perceived exertion scale, and the SF-36 quality of life questionnaire were utilized. Patients were monitored during the test. The sample was dichotomized based on test performance and SF-36 scores. Furthermore,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
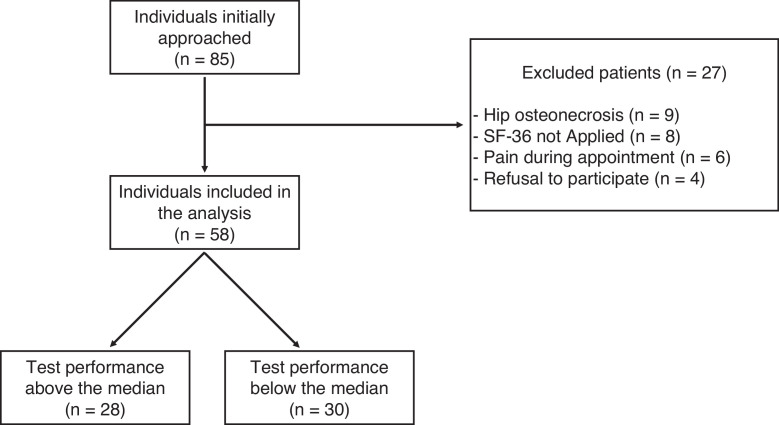 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemoglobinopathies and Related Disorders · Medical Case Reports and Studies · Iron Metabolism and Disorders
Introduction
Sickle cell disease (SCD), resulting from a mutation in the hemoglobin (Hb) gene that leads to the formation of Hb S, is the most prevalent recessive monogenic disease in the world. There are multiple genotypes that cause SCD including the severe homozygous form, Hb SS, or as heterozygous forms with other hemoglobin variants, such as Hb C or Hb β-thalassemia [1].
When deoxygenated, Hb S polymerizes and modifies the morphology of red blood cells making their membrane rigid and into a sickle shape. This modified state favors the occurrence of vaso-occlusive crises (VOC), endothelial dysfunction, hemolysis, and activation of inflammatory responses through the release of cytokines and reactive oxygen species. VOC lead to ischemia and are the main factor responsible for pain crises in SCD as well as other complications, such as acute chest syndrome and osteonecrosis. Endothelial dysfunction is associated with intravascular hemolysis, nitric oxide depletion and hypercoagulability, and is the underlying mechanism of complications such as strokes, pulmonary hypertension and organ damage, especially of the kidneys and heart [1,2].
The complex physiopathology of SCD reduces tolerance to physical exertion, which is seen by a reduced functional capacity (FC). The acute complications of SCD result in school and work absenteeism, negative impacts on socialization and a low quality of life. Therapeutic exercise is an important tool for rehabilitation in SCD, recovering cardiorespiratory capacity and autonomy, and improving socialization. However, the prescription of exercise in SCD is a highly complex topic and may cause VOC if excessively intense [2].
Assessing FC is crucial for developing an appropriate exercise prescription, as a wide array of functional assessment tools, ranging from simple field tests to sophisticated laboratory procedures, is available. The cardiopulmonary exercise test (CPET) is the gold standard; however, it requires specific, costly equipment that limits its availability [3]. Other methods for functional assessment consist in field tests, which include the ergometric test, Bruce protocol, 6-Minute Walk Test (6MWT), and the 1-Minute Sit-to-Stand test (1-MSTST) [4,5]. The 1-MSTST is a submaximal test validated for assessing FC, postural control, proprioception, and lower limb strength. It is a well-tolerated, low-cost test that can be applied domestically, at the bedside and in small rooms as it only requires an armless chair, a stopwatch and minimal floor space [6,7]. To the present moment, there are no studies assessing FC in SCD patients utilizing the 1-MSTST.
Objective
The objective of this study is to assess FC in adult SCD patients using the 1-MSTST test, and to evaluate possible associations between the FC, quality of life, and clinical and demographic variables.
Method
This cross-sectional pilot study to assess FC in SCD patients using the 1-MSTST was carried out between January and April 2024. Participants were active patients in a secondary care facility specialized in hematology and hemotherapy. Adults aged between 18 and 60 years, diagnosed with SCD, who signed an informed consent form, participated in the study. Exclusion criteria were: refusal to participate; clinical events during the 1-MSTST; a drop in oxygen saturation >4 % during the 1-MSTST; systolic blood pressure >180 mmHg or diastolic blood pressure >110 mmHg; unstable angina; resting heart rate >120 bpm; and orthopedic conditions that limited performance in the 1-MSTST.
The instruments utilized for this study were: the 1-MSTST test, the Borg rate of perceived exertion scale for the assessment of work of breathing, [8] and the Short Form 36 Health Survey Questionnaire, [9] which is divided in eight domains (Physical functioning; physical role limitations; bodily pain; general health perceptions; energy/vitality; social functioning; emotional role limitations; and mental health) and two summary measures (physical component summary and mental component summary). All anthropometric and clinical data were collected with standardized equipment and all tests were performed supervised by trained research staff. A brochure containing information about lifestyle changes and possible physical activities was created by the research staff and handed to the study participants.
Initially, a descriptive analysis was performed utilizing the adequate frequency and central tendency measures. The study by Strassman et al. was utilized to obtain the age-corrected target repetitions for the 1-MSTST [10] by which our sample was standardized. For the comparative analysis, the sample was divided in two groups based on the median 1-MSTST performance, and analyzed with Student’s t-test and Pearson’s chi-squared test. The variables included in the analysis were age, gender, ethnicity, SCD genotype, use of hydroxyurea, 1-MSTST performance, baseline and post-intervention heart rate, baseline and post-intervention peripheral oxygen saturation, and baseline and post-intervention Borg scale. The software IBM SPSS Statistics 25® was utilized for the statistical analysis. This study was registered and approved by the institution’s research ethics committee under the number CAAE 63,424,422.9.0000.5118.
Results
In total, 85 individuals met the inclusion criteria of the study; however, 27 were later excluded, as nine had a diagnosis of hip osteonecrosis, eight did not complete the SF-36 health survey questionnaire, six presented with lower body pain during the clinical assessment and four refused to participate. After the 58 participants performed the 1-MSTST, the sample was divided in two groups based on the median performance (20.75 repetitions): 28 patients had an above median performance and 30 patients had a below median performance (Figure 1).Figure 1. Study flowchart.Figure 1
Of the 58 participants, the average age was 29.84 ± 11.20 years with ages ranging between 18 and 59 years, 55.1 % were male, and 79.3 % identified themselves as Black. The most frequent genotype was Hb SS (n = 39; 67.2 %) and 77.5 % of the sample was taking hydroxyurea. In the comparative analysis, the group with the best 1-MSTST performance had a statistical tendency to be younger (p-value = 0.08), and had a higher post-intervention heart rate (p-value = 0.001). The other analyzed variables were not statistically significant, such as use of hydroxyurea and disease genotype (Table 1).Table 1. Demographic and clinical variables of the sample categorized by 1-MSTST performance.Table 1. VariableTotalMedian performancep-value<20.75 repetitions (n = 30)>20.75 repetitions (n = 28)Age (mean)29.84 ± 11.2032.27 ± 11.9527.25 ± 9.890.08Gender, male – n (%)32 (55.1)15 (50)17 (60.7)0.41Race, black – n (%)46 (79.3)24 (80)22 (78.6)0.57Genotype – n (%)0.75Hb SS39 (67.2)20 (66.7)19 (67.9)Hb Sβ^+^9 (15.5)5 (16.7)4 (14.3)Hb SC9 (15.5)4 (13.3)5 (17.9)Hb Sβ^0^1 (1.7)1 (3.3)0 (0)MedicationHydroxyurea use45 (77.5 %)23 (76.7 %)22 (78.6 %)0.86Average dosage (mg)1130.16 ± 360.571133.70 ± 400.361126.45 ± 323.190.941-MSTSTRepetitions20.44 ± 5.8815.96 ± 3.8625.25 ± 3.29<0.001Target/real performance ratio (%)43.86 ± 11.7934.94 ± 7.5153.42 ± 7.07<0.001Baseline heart rate (bpm)78.69 ± 13.1076.66 ± 11.2880.87 ± 14.700.22Post intervention heart rate (bpm)121.05 ± 20.42112.73 ± 20.84129.96 ± 15.950.001*Baseline O_2_ saturation (%)93.68 ± 4.0193.43 ± 4.5793.96 ± 3.360.61Post intervention O_2_ saturation (%)92.81 ± 4.3992.70 ± 5.2292.94 ± 3.370.83Baseline Borg1.61 (0 - 2.12)1.851.350.36Post intervention Borg5 ± 2.135.1 ± 2.374.89 ± 1.880.711-MSTST: 1-minute sit-to-stand test.
The data regarding the results of the SF-36 health survey analysis are found in Table 2. The group with a worse performance in the 1-MSTST had statistically significant lower scores in the physical component summary (p-value = 0.05), mental health (p-value = 0.01) and general health perceptions (p-value = 0.02). Other SF-36 health survey dimensions, such as physical role limitations (p-value = 0.07) and physical functioning (p-value = 0.09) approached statistical significance for a worse score in the group with the worst performance.Table 2. Results of SF-36 health survey analysis categorized by 1-MSTST performance.Table 2SF-36TotalMedian performancep-value<20.75 repetitions (n = 30)>20.75 repetitions (n = 28)PCS44.45 ± 9.7442.12 ± 9.2746.95 ± 9.760.05MCS47.97 ± 12.3845.39 ± 13.2350.73 ± 10.960.10Physical functioning72.98 ± 20.8268.16 ± 20.1177.50 ± 21.010.09Physical role limitations60.52 ± 44.3052.50 ± 45.6573.21 ± 39.630.07Emotional role limitations68.41 ± 38.0360.00 ± 40.4973.80 ± 37.790.18Energy/vitality59.91 ± 28.3054.33 ± 25.6863.39 ± 29.440.21Mental health68.70 ± 25.5161.86 ± 25.7076.71 ± 20.070.01Social functioning79.60 ± 29.3776.66 ± 30.2183.48 ± 28.060.37Bodily pain76.57 ± 30.2366.30 ± 33.5278.78 ± 29.300.13General health perceptions50.70 ± 25.1644.86 ± 20.5359.32 ± 26.270.02SF-36: SF-36 health survey questionnaire; PCS: Physical component summary; MCS: Mental component summary.
Discussion
SCD is one the most epidemiologically relevant hematological conditions in the world. In Brazil it represents an important health burden, affecting an estimated 60,000–100,000 people [11]. Between 2014 and 2020, an annual average of 1087 people were born with the disease in Brazil, with an incidence of 3.75 cases per 10,000 newborns [12]. SCD represents a challenge for the Brazilian public health system due to its complex pathophysiology, need for interdisciplinary care, and socioeconomic impact. Historically, newborn screening and continued health education, in addition to regular medical care, have been effective strategies for reducing complications and increasing quality of life for SCD patients in Brazil [1].
Patients were not included in the analysis of this study if they presented with conditions that could interfere with their performance in the 1-MSTST, the most prevalent of which was hip osteonecrosis, with a frequency of 10.58 %. Osteonecrosis is a frequent complication of SCD that occurs due to VOC with the most frequent sites being the hips, vertebrae and shoulders [13]. The prevalence of osteoarticular involvement increases with age. Ouederni et al. found a prevalence of hip osteonecrosis of 18.3 % in 20-year-old SCD patients, compared to a 2.3 % hip osteonecrosis prevalence in 10-year-olds [14,15]. Daltro et al. reported a prevalence of osteonecrosis in 11.1 % of SCD patients in Brazil, most frequently of the hip joint (74.6 %), [15] a result similar to the current findings.
Regarding the SCD genotype, 67.1 % of the present sample had the Hb SS genotype, a proportion similar to other Brazilian studies, such as Silva et al., whose group identified a slightly greater prevalence of Hb SS, at 75 % [16]. Souza et al. identified a lower prevalence of 60 % in their sample with Hb SS [17]. These variations are common and reflect differences in recruiting methods and populations. Cardoso et al. found a median age of 28.6 ± 9.9 years and a 65 % prevalence of Hb SS, very similar results to this study [18]. These findings reinforce the representativeness of the current sample. The different genotypes of SCD correlate to disease severity and symptomatology: Hb Sβ^+^-thalassemia and Hb SC are considered of mild severity, while Hb SS and Hb Sβ^0^-thalassemia present a greater clinical relevance and severity [19]. In this study, the SCD genotype was not significantly associated with worse 1-MSTST performance, possibly due to the high proportion of Hb SS in the sample (n = 39; 67.2 %).
A worse performance in the 1-MSTST was observed among older participants (p-value = 0.08), which may be explained by the buildup of osteoarticular and inflammatory damage caused by SCD and aging. Other sociodemographic variables, such as gender and ethnicity, were not statistically significant in this study. Hydroxyurea is the most efficient pharmacological therapy for SCD available in Brazil; its use is associated with a lower rate of degenerative damage [19,20]. In the present study, 77.5 % of the participants were in continuous use of hydroxyurea; however, its use was not associated with a better performance in the 1-MSTST (p-value = 0.86). The authors did not find any literature regarding 1-MSTST performance and use of hydroxyurea, or other drugs, among SCD patients.
No participants of this study were capable of reaching their age-corrected performance target for the 1-MSTST. Studies utilizing other methods to assess FC in SCD patients present with similar results. Cardoso et al. assessing the FC in an adult population with sickle cell anemia utilizing the 6MWT found that the average distance covered by study participants was less than the expected target distance for the Brazilian population (335.3 ± 70.6 m versus 504.7 ± 5.5 m; p-value <0.001) [21]. The 1-MSTST is a low-cost, simple assessment that can be applied in domestic and bedside environments; it provides a similar hemodynamic and ventilatory response to the 6MWT, which is considered the gold-standard field FC assessment tool. There are no studies utilizing the 1-MSTST to assess FC in SCD, which is a limiting factor of the present discussion.
The association between quality of life and FC is evident in several health conditions, including SCD, in which individuals present with decreased tolerance to physical exertion, resulting in loss of muscle mass and adverse psychosocial effects. In addition, it is common for SCD patients to be advised to avoid physical activities, leading to a sedentary lifestyle and increasing adverse psychosocial and body composition effects [22, 23, 24]. A study with SCD patients implemented an eight-week exercise program, with results showing increases in both the FC and quality of life assessed by the SF-36 health survey [23]. The present study found that a worse performance in the 1-MSTST was associated with a worse quality of life assessed by the SF-36 health survey questionnaire. Therefore, in patients with physical disabilities caused by SCD, an approach focused on mental health, in addition to physical training, is of utmost importance, as anxiety and depressive symptoms are very common in this population [24].
Conclusion
In this study, a better performance in the 1-MSTST was associated with a better quality of life assessed using the SF-36 health survey, however there was no statistical association with any of the clinical and demographic variables. The 1-MSTST, a low cost and easily applicable tool for FC assessment, could be a useful addition to the physical evaluation of SCD patients. The multidisciplinary team could use this test for triage during routine follow-ups and stimulate early physical health interventions for the purpose of reducing morbidity associated with SCD.
Conflicts of interest
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kavanagh P.L.Fasipe T.A.Wun T.Sickle cell disease: a review JAMA 3281202257683578879010.1001/jama.2022.10233 · doi ↗ · pubmed ↗
- 2Pinto D.M.R.Physical exercise in sickle cell anemia: a systematic review Hematol Transfus Cell Ther 43320213243313303295210.1016/j.htct.2020.06.018PMC 8446247 · doi ↗ · pubmed ↗
- 3Smith K.N.Baynard T.Fischbach P.A.Hankins J.S.Hsu L.L.Murphy P.M.Safety of maximal cardiopulmonary exercise testing in individuals with sickle cell disease: a systematic review Br J Sports Med 56132022 Jul 7647693428505410.1136/bjsports-2021-104450 PMC 8770664 · doi ↗ · pubmed ↗
- 4JÁAraujo Junior DAA Rossi Valadão T.F.C.Mattos J.C.M.Catai A.M.Sato T.O.Cardiovascular benefits of a home-based exercise program in patients with sickle cell disease Plos One 165202102501281210.1371/journal.pone.0250128 PMC 811577933979369 · doi ↗ · pubmed ↗
- 5American Thoracic Society ATS statement: guidelines for the six-minute walk test Am J of Respir Crit Care Med 166200211111710.1164/rccm.166/1/11112091180 · doi ↗ · pubmed ↗
- 6Pereira M.C.Lima L.N.G.Moreira M.M.Mendes F.A.R One minute sit-to-stand test as an alternative to measure functional capacity in patients with pulmonary arterial hypertension J Bras Pneumol 48320222021048310.36416/1806-3756/e 20210483 PMC 906462135508068 · doi ↗ · pubmed ↗
- 7Reychler G.Pincin L.Audag N.Poncin W.Caty G.One-minute sit-to-stand test as an alternative tool to assess the quadriceps muscle strength in children Respir Med Res 78202010077710.1016/j.resmer.2020.10077732623309 · doi ↗ · pubmed ↗
- 8Loss L.C.Born P.L.Wolf R.Stefanello J.M.F.Pereira G.A systematic review of cross-cultural adaptation and validation of Borg’s Rating of perceived exertion scale J Phys Educ 282017 e 285310.4025/jphyseduc.v 28i 1.2853 · doi ↗