Synovial fluid α-defensin might be false positive in early stages after major total arthroplasty revision surgery
Sankalp Mrutyunjaya, Wade A. Banta, Joseph R. B. Espiritu, Derek F. Amanatullah

TL;DR
A patient had repeated false positive results from a synovial α-defensin test for years after a knee surgery, suggesting the test may be unreliable in early post-surgery stages.
Contribution
This case highlights potential false positives in synovial α-defensin testing after revision arthroplasty, raising concerns about its reliability in early recovery phases.
Findings
A patient received multiple false positive synovial α-defensin test results over nearly three years post-surgery.
The findings suggest the test may not be reliable in the early stages following revision total knee arthroplasty.
Abstract
Generalizability is critical when evaluating the performance of a diagnostic test to ensure variations in the patient population are represented. We report a case of a patient receiving multiple false positive results from the synovial α -defensin test observed over close to a 3-year period following revision total knee arthroplasty.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
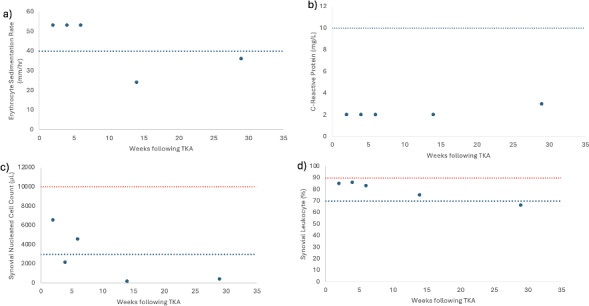 Figure 1
Figure 1| 2 weeks | 4 weeks | 6 weeks | 14 weeks | 29 weeks | 143 weeks | |
|---|---|---|---|---|---|---|
| S | Positive | Positive | Positive | Negative | Negative | Negative |
| Synovial CRP | 1.9 mg L−1 | 1.1 mg L−1 | 0.8 mg L−1 |
|
|
|
| Culture | Negative | Negative | Negative | Negative | Negative | Negative |
| MSIS score | 1* | 1* | 1* | 2 | 0 | 0 |
| Synovial nucleated cell count | 6533 | 2139 | 4556 | 178 | 416 | |
| Synovial leukocyte (%) | 85 | 86 | 83 | 75 | 66 |
| Authors | Year | Concern for false positive S |
|---|---|---|
| Partridge et al. (2017) | 2017 | Gout after total knee arthroplasty |
| Plate et al. (2018) | 2018 | Inflammatory arthritis |
| Cooper et al. (2021) | 2021 | Native knee joint infection |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Peptides and Activities · Osteoarthritis Treatment and Mechanisms · Orthopedic Infections and Treatments
Introduction
1
Generalizability is the ability to infer results from one set of circumstances from a clinical trial and apply them to other settings (Davis, 1994). This concept is critical when evaluating the performance of a diagnostic test. Clinical trials used to evaluate diagnostic tests typically involve small subsets of patients which may not encompass the diversity represented by the target clinical demographic (Davis, 1994). The effect of generalizability is usually applied to variations in the patient population.
Generalizability can also include healthcare provider acceptance and the proper application of a diagnostic test (Uy, 2022). Overgeneralization may skew pre-test probability having an impact on the final diagnosis. Hence, a mismatch between the provider's perceived pre-test probability and the revised probability after receiving the test results can potentially extend the cost and duration of care. Therefore, it is important that clinicians using diagnostic tests consider pre-test probability while maintaining high accuracy in diagnosis to optimize the use of healthcare resources to treat patients (Uy, 2022).
Here we look at a case where pre-test probability can affect the use of a diagnostic test, synovial -defensin (S D), designed for detection for periprosthetic joint infections (PJIs) (Rycyk-Bojarzyńska et al., 2024; Stone et al., 2019). The diagnosis of periprosthetic joint infection typically involves monitoring serum erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels, along with intra-articular recruitment of polymorphonuclear cells by bacteria (Stone et al., 2019). S D is an immunoassay that measures the intra-articular concentration of the -defensin peptide released during the presence of a pathogen (Rycyk-Bojarzyńskaet al., 2024). In 2018, S D was added to the Musculoskeletal Infection Society (MSIS) criteria; our case report shows a false positive S D result and serves as an example of how overgeneralization of any highly specific tests has the potential to influence patient care (Kim and Cho, 2021).
Case history
2
A 55-year-old male presented with a history of type II diabetes mellitus, obesity (body mass index: 35.3 kg m^−2^), hypertension, and multiple orthopedic procedures – including right shoulder arthroplasty, left Achilles tendon debridement, right multi-ligamentous knee reconstruction, patellar tendon lengthening with patellectomy, and an eventual total knee arthroplasty (TKA) – in December 2016. The patient was involved in a motor vehicle accident in November 2020, resulting in progressive pain, swelling, instability, and extensor lag ( 30°) of his right TKA. He underwent revision TKA for global instability with extensor mechanism reconstruction in March 2021.
(a) ESR levels, (b) CRP levels, (c) synovial leukocyte count, and (d) percentage of synovial leukocytes reported based on the postoperative week tested. The dotted blue line indicates 2018 MSIS thresholds for each laboratory value (Prince et al., 2020). The dotted red line in panels (c) and (d) indicates the threshold for PJI within 6 weeks (Prince et al., 2020; Rycyk-Bojarzyńska et al., 2024).
Given the patient's numerous knee incisions from his prior multi-ligamentous knee reconstruction, the distal aspect of his midline incision over the tibial tubercle exhibited poor incisional healing 2 weeks after revision surgery, with a skin bridge of 7 cm from a more lateral incision. This was treated with dry dressings, and oral antibiotics were not started. At this time, serum markers and a synovial aspiration were drawn to evaluate for an infection (Fig. 1, Table 1). All tissue and synovial aspirations are routinely held for 14 d to evaluate for fastidious organisms, like Cutibacterium acnes, and, in patients with risk factors for immunosuppression, any fungal cultures are held for 30 d.
The patient was readmitted 4 weeks after surgery with cellulitis at the right shin and new blistering at the distal aspect of the incision. A synovial aspiration revealed negative aerobic and anaerobic cultures, improving aspirate with respect to synovial nucleated cell count, and a second positive S D test (Fig. 1c and d, Table 1). He was subsequently diagnosed with cellulitis in the distal tibia, together with congestive heart and liver failure (e.g., hepatosplenomegaly and hepatic steatosis). Infectious disease consultation recommended monitoring the patient off antibiotics and repeat testing at 6 weeks (Fig. 1, Table 1). Given the early interval, acute thresholds for PJI were applied (Bingham et al., 2014).
For 3 months after surgery, the patient continued with bilateral pitting edema and an elevated jugular venous pressure, necessitating urgent diuresis in the emergency department. Repeat serologies and synovial fluid aspiration then showed improvement and a negative S D test in correlation with wound healing (Fig. 1, Table 1). At this time, the patient no longer met the MSIS infection criteria. Testing for CRP and ESR was performed 143 weeks after surgery, and the patient remained infection free (ESR: 16 mm h^−1^; CRP: 2.9 mg L^−1^; Table 1).
Discussion
3
TKA is one of the most common surgeries performed in the United States (Weinstein et al., 2023). PJI is one of the most common reasons for revision arthroplasty (Heckmann et al., 2023). PJIs occur in about 2.4 % of total joint replacements and represent a burden to patients and the healthcare system (Suen et al., 2018). PJIs are diagnosed in accordance with MSIS criteria which look at serum and synovial biomarkers (Heckmann et al., 2023). However, S D testing looks specifically for the -defensin peptide present in the synovial fluid (Suen et al., 2018). In the patient case presented above, we observe S D showing a false positive result for PJI.
In observing the patient's laboratory results, the S D test performed prior to postoperative week 6 consistently showed positive results. Although this result would appear to be indicative of a PJI, other laboratory results for CRP and synovial leukocyte count show less consistency with the S D test, making the diagnosis less clear. CRP trends throughout the postoperative period show no abnormal values, while synovial leukocyte cell count shows initial fluctuation through weeks 2 and 6. These inconsistencies follow when observing calculated MSIS scores in which weeks 2 and 6 in the postoperative period would be indicative of PJI, while week 4 would not be indicative of PJI. PJI in an acute setting ( 90 d post-operation) would show a synovial leukocyte cell count greater than 10 000 and a synovial leukocyte percentage greater than 90 % (Kim and Cho, 2021). However, weeks 2 through 6, which are within 90 d of the postoperative period, consistently show values below this threshold for acute PJI (Fig. 1). Ultimately, all laboratory measurements trend below the abnormal threshold by week 29 of the postoperative period. With the patient's aspirated synovial fluid also being negative for aerobic and anaerobic bacterial cultures in all instances, it is more likely that the patient never had PJI and that the presence of -defensin peptide can be potentially attributed to other causes unrelated to a PJI that stimulated the innate immune system.
The S D results in this case are likely false positives. The effects of both the surgical wound (acute postsurgical insult of a TKA and the presence of an allograft extensor mechanism reconstruction) and the circumstances of the patient (liver failure and congestive heart failure) on S D have not been formally evaluated (Kumar et al., 2023). Hence, S D, in the context of evaluating PJI, may not be used exclusively as an MSIS minor criterion to diagnose PJI because of multiple confounding factors that may lead to variation in the -defensin levels. This variation in -defensin levels only strengthens the mismatch between the provider's pre-test probability and revised probability after S D due to the inconsistency between a positive S D and negative culture result and downward trend in the levels of multiple biomarkers. Although the qualitative synovial -defensin test (e.g., positive/negative) has a sensitivity of 97 %, a specificity of 95 %, a positive predictive value of 88 %, a negative predictive value 99 %, and an area under the curve of 0.99, we can see that despite the high sensitivity and specificity, S D may add little to or even limit the traditional serological and synovial data work-up used to diagnose a PJI (Bingham et al., 2014). As such, this highlights the importance of critically evaluating different tests involved in the potential diagnosis of a failed arthroplasty. Other studies have noted issues of false positive results with S D results due to non-infectious inflammatory disease, such as acute gout, or the inability to reliably distinguish between septic and inflammatory arthritis (Table 2) (Partridge et al., 2017; Plate et al., 2020; Cooper et al., 2021). With the clinical utility of S D in question, using -defensin to diagnose PJIs indiscriminately can easily increase the burden on the patient due to a lack of generalizability and falsely confirming a physician's pretest probability.
Table 2: Other studies reporting on false positive S α D results.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bingham J Clarke H Spangehl M Schwartz A Beauchamp C Goldberg B The Alpha Defensin-1 Biomarker Assay can be Used to Evaluate the Potentially Infected Total Joint Arthroplasty Clin Orthop Relat Res 4724006400910.1007/s 11999-014-3900-7201425256621 PMC 4397781 · doi ↗ · pubmed ↗
- 2Cooper KB Siegel ER Stambough JB Bumpass DB Mears SC The Alpha-Defensin Prosthetic Joint Infection Test Has Poor Validity for Native Knee Joint Infection J Arthroplasty 362957296110.1016/j.arth.2021.03.020202133896668 · doi ↗ · pubmed ↗
- 3Davis C Generalizing from clinical trials Controlled Clinical Trials 15111410.1016/0197-2456(94)90023-x 19948149768 · doi ↗ · pubmed ↗
- 4Heckmann ND Wang JC Liu KC Won P Chung BC Mayer LW Longjohn DB Oakes DA Christ AB Lieberman JR Refining the Role of Routine Synovial Alpha-Defensin in Periprosthetic Joint Infection Following Total Knee Arthroplasty: An Analysis of Limitations J Arthroplasty 382691269710.1016/j.arth.2023.05.095202337295619 · doi ↗ · pubmed ↗
- 5Kim S-J Cho YJ Current Guideline for Diagnosis of Periprosthetic Joint Infection: A Review Article Hip Pelvis 33111710.5371/hp.2021.33.1.11202133748021 PMC 7952269 · doi ↗ · pubmed ↗
- 6Kumar P Mittal A Bansal P Aggarwal S Rajnish RK Dadra A Sharma S Wound alpha defensin levels are significantly higher in patients with fracture related infection: A pilot, prospective cohort study Injury 5441642110.1016/j.injury.2022.12.014202336567156 · doi ↗ · pubmed ↗
- 7Partridge DG Gordon A Townsend R False-positive synovial fluid alpha-defensin test in a patient with acute gout affecting a prosthetic knee Eur J Orthop Surg Traumatol 2754955110.1007/s 00590-017-1942-8201728314986 · doi ↗ · pubmed ↗
- 8Plate A Stadler L Sutter R Anagnostopoulos A Frustaci D Zbinden R Fucentese SF Zinkernagel AS Zingg PO Achermann Y Inflammatory disorders mimicking periprosthetic joint infections may result in false-positive α -defensin Clin Microbiol Infect 241212.e 110.1016/j.cmi.2018.02.019202029496595 · doi ↗ · pubmed ↗