Coronavirus disease 2019 pneumonia with concomitant spontaneous pneumomediastinum, pneumothorax, and subcutaneous emphysema in a non-ventilated patient, complicated by pulmonary embolism: a case report
Qiuyu Martin Zhu, Amitosh K. Singh, Peter M. Huh, Sandeep Konka

TL;DR
A non-ventilated patient with COVID-19 developed rare complications including pneumomediastinum, pneumothorax, and subcutaneous emphysema, which were successfully treated with a novel therapy and anticoagulation.
Contribution
Presents a rare case of concurrent spontaneous pneumothorax, pneumomediastinum, and subcutaneous emphysema in a non-ventilated COVID-19 patient complicated by pulmonary embolism.
Findings
A 56-year-old non-ventilated patient with COVID-19 developed spontaneous pneumomediastinum, pneumothorax, and subcutaneous emphysema.
The patient was successfully treated with vacuum-assisted closure therapy and anticoagulation for pulmonary embolism.
The case emphasizes the importance of vigilance for these complications in non-intubated patients.
Abstract
Spontaneous pneumomediastinum, pneumothorax, and subcutaneous emphysema are life-threatening complications of coronavirus disease 2019. Concomitant presentation of all three with further complication by pulmonary embolism in non-intubated patients with coronavirus disease 2019 is exceedingly rare and can be devastating. We present a case of concurrent spontaneous pneumomediastinum, pneumothorax, and subcutaneous emphysema in a non-ventilated, 56-year-old Hispanic male with coronavirus disease 2019 pneumonia that was further complicated by extensive pulmonary embolism. In addition to treatment of coronavirus disease 2019 pneumonia, the patient was treated with an innovative strategy by creating a blowhole incision over the chest wall connected to vacuum-assisted closure therapy resulting in rapid clinical improvement. He was also started on systemic anticoagulation therapy for pulmonary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
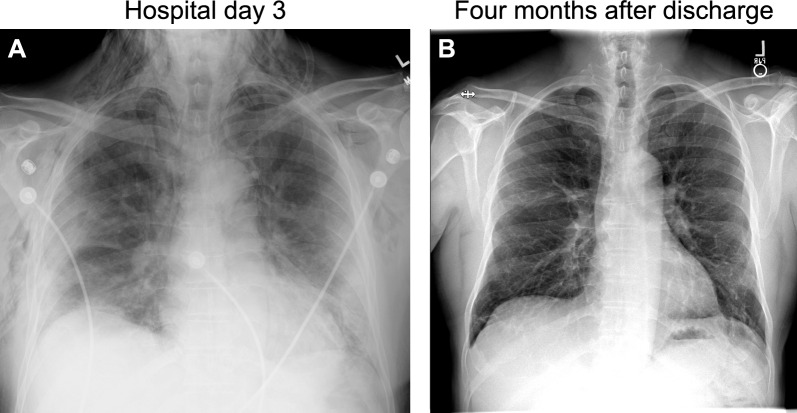 Figure 1
Figure 1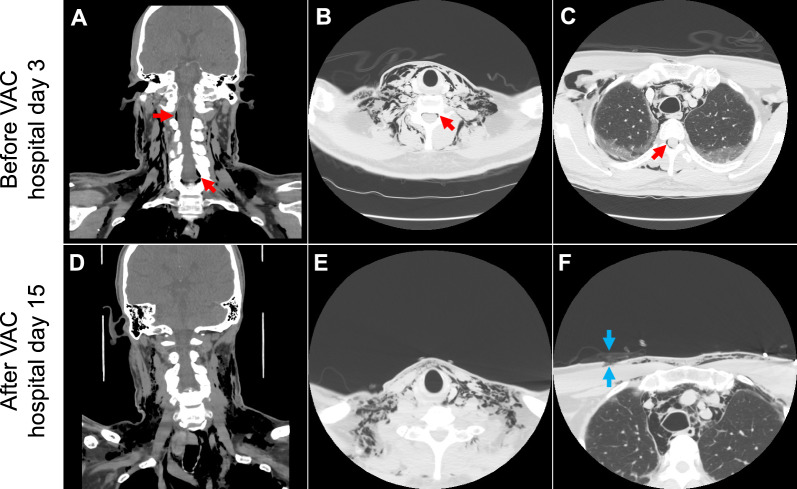 Figure 2
Figure 2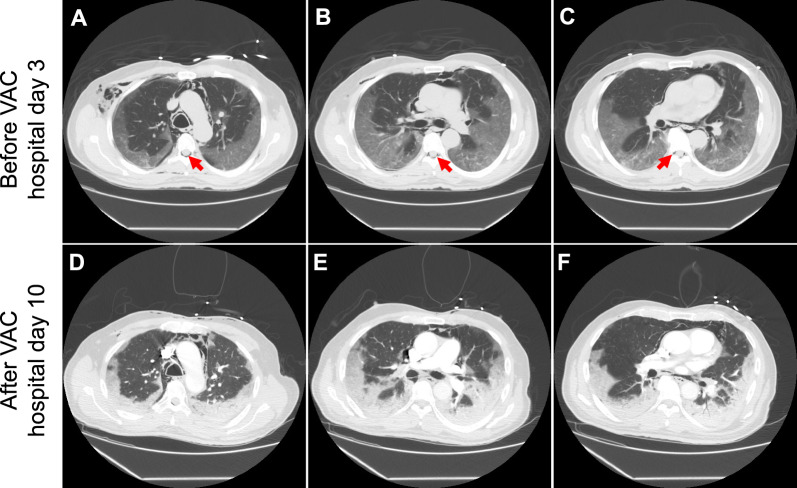 Figure 3
Figure 3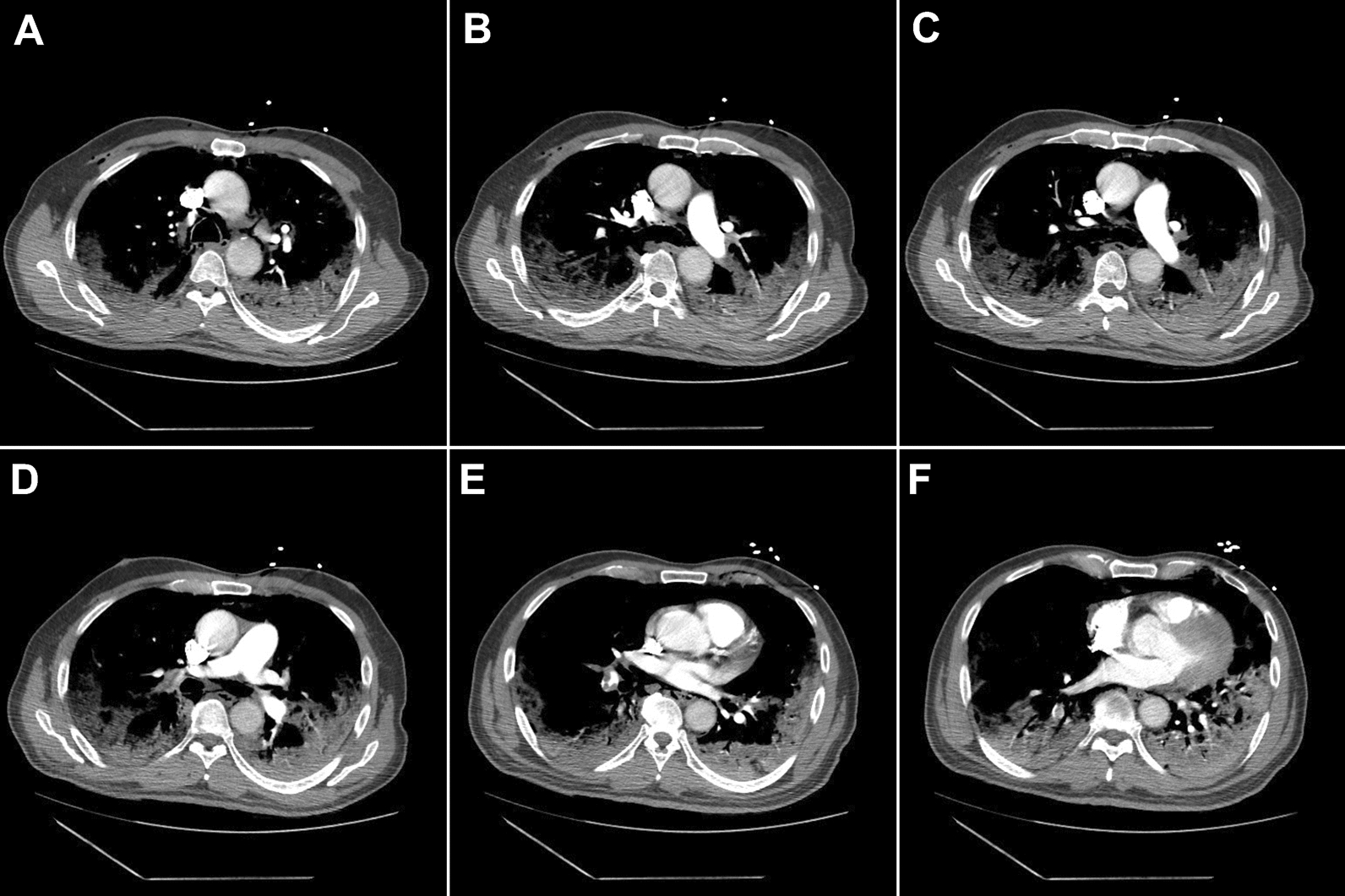 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumothorax, Barotrauma, Emphysema · Abdominal Surgery and Complications · Respiratory Support and Mechanisms
Background
At the end of 2019, a novel coronavirus was identified as the cause of a cluster of pneumonia cases in Wuhan, China, which was later designated as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). In February 2020, the World Health Organization designated the disease coronavirus disease 2019 (COVID-19) [1].
The pulmonary symptoms of COVID-19 range from asymptomatic infections, to mild disease (no pneumonia or mild pneumonia), to severe or critical disease (for example, with dyspnea, hypoxia, or more than 50% lung involvement on imaging) that may require mechanical ventilation, with an overall mortality of 5% [2].
Here, we present a rare case of concomitant spontaneous pneumomediastinum, pneumothorax, and subcutaneous emphysema in a non-ventilated patient with COVID-19 pneumonia, complicated by extensive pulmonary embolism (PE). The patient achieved a favorable outcome through prompt clinical recognition and innovative management using vacuum-assisted closure (VAC) therapy. Given the potentially high mortality rate associated with these complications, our case offers a practical example that can help guide the future management of similar cases.
Case presentation
A 56-year-old Hispanic male with a history of untreated type 2 diabetes (hemoglobin A1c 12.2%), hypertension, and dyslipidemia presented to the emergency department with progressive dyspnea and hypoxemia. He had been diagnosed with COVID-19 infection 4 days earlier and had been managing his symptoms of fever and sore throat at home. The patient received the Johnson and Johnson SARS-CoV-2 vaccine 4 months earlier. He had no prior lung pathology but was a former smoker (1.25 pack-years), who quit 11 years ago. He denied alcohol or recreational drug use.
On arrival, the patient complained of generalized weakness and intractable hiccups, stating he was so weak that he could not walk at home. His hiccups were persistent and sometimes caused dyspnea. He denied cough, nausea, vomiting, chest pain, or diarrhea. Physical examination revealed fatigue and discomfort due to hiccups. He was afebrile, with tachycardia (pulse 116 beats per minute), tachypnea (respiration 22 breaths per minute), and hypoxia (oxygen saturation of 86% on room air, improving to 93% on 3 L/minute oxygen by nasal cannula). Lung auscultation revealed bilateral rhonchi without wheezing or rales.
Given concern for diaphragmatic irritation secondary to PE causing hiccups, a chest computed tomography (CT) angiography was performed, showing bilateral peripheral ground-glass infiltrates but no evidence of PE. Electrocardiogram (EKG) showed sinus tachycardia of 108 beats per minute, left axis deviation, large P waves, T wave inversions in V1, and no acute ischemic changes. Laboratory studies revealed thrombocytopenia (88 × 10^9^/L), hyponatremia (128 mmol/L), and hyperglycemia (17.9 mmol/L). Remaining labs were otherwise normal, including white blood cell count (6.6 × 10^9^/L), hepatic function, and negative high-sensitivity troponin and creatine kinase. Inflammation markers were elevated, including erythrocyte sedimentation rate (63 mm/hour), ferritin (3118.20 ng/mL), high-sensitivity C-reactive protein (> 200.00 mg/dL), D-dimer (305 ng/mL DDU), and lactate (2.50 mmol/L). The patient received dexamethasone, remdesivir, and tocilizumab. His hiccups improved with chlorpromazine, famotidine, and sucralfate. He received supplemental oxygen via nasal cannula and never required positive-pressure devices.
On hospital day 3, the patient complained of sudden-onset neck and chest pain with a popping sensation in his right neck after a coughing spell. Physical examination showed mild swelling along the right neck border without crepitus or respiratory distress. A prompt chest radiography revealed diffuse bilateral lung infiltrates and extensive subcutaneous emphysema (Fig. 1A). CT of the neck and chest showed extensive pneumomediastinum, small right apical pneumothorax, bilateral subcutaneous emphysema extending into the neck, and epidural air (Figs. 2 and 3). Shortly after the imaging, the patient became tachycardic and tachypneic, requiring supplemental oxygen with a non-rebreather mask. Physical examination showed subcostal retractions and crepitus on the upper chest wall and neck. Emergency treatment was initiated by thoracic surgery and intensive care unit (ICU) teams at the bedside via a blowhole incision over the right anterior chest wall connected to a subcutaneous VAC device set at −125 mmHg negative pressure, resulting in immediate clinical improvement. The patient quickly transitioned back to nasal cannula and felt much better.Fig. 1. Chest radiography on hospital day 3 (A) and at 4 months after discharge (B). (A) The radiography was obtained on hospital day 3 after the patient developed a “popping sensation” in the neck, showing diffuse bilateral lung infiltrates and extensive subcutaneous emphysema. There was widening of the mediastinum consistent with pneumomediastinum, although it could have been positional. (B) At 4-month follow up, the radiography showed significant improvement of bilateral lung infiltrates and complete resolution of subcutaneous edemaFig. 2Computed tomography of the neck obtained before (A–C, on hospital day 3) and after vacuum-assisted closure therapy (D–F, on hospital day 15). (A–C) The images were obtained immediately after the patient developed a “popping sensation” in the neck, showing extensive subcutaneous emphysema tracking along the fat planes in the bilateral neck and chest. There was extensive pneumomediastinum and right apical pneumothorax. Air was also in the epidural space (red arrows). (D–F) After VAC therapy, the overall volume of superficial emphysema throughout the neck decreased. The right anterior chest blowhole incision is seen connected to topical vacuum-assisted closure dressing (blue arrows). (A and D), coronal section; (B, C, E, and F), axial sectionFig. 3Computed tomography of the chest obtained before (A–C, on hospital day 3) and after vacuum-assisted closure therapy (D–F, on hospital day 10). (A–C) The images were obtained on the day when the patient developed chest pain and a “popping sensation” in the neck, showing extensive subcutaneous emphysema and pneumomediastinum. Gas tracks along the right pleural space. Epidural gas is also seen within the thoracic spine (red arrows). (D–F) The images were obtained on hospital day 10 to rule out pulmonary embolism when the patient developed worsening hypoxia, while on vacuum-assisted closure therapy. The overall decrease in the volume of soft tissue emphysema can be appreciated compared with (A–C). Significant bilateral consolidation compatible with coronavirus disease 2019 infection appears similar on the two sets of images
On hospital day 10, the patient developed worsening hypoxia, requiring high-flow nasal cannula. CT angiography showed PE involving all proximal right lung fields and a few peripheral fields on the left (Fig. 4). He started anticoagulation therapy with subcutaneous enoxaparin.Fig. 4. Computed tomography angiography of the chest obtained on hospital day 10. Through (A–F), there are proximal and peripheral filling defects in pulmonary arteries supplying all three lung fields on the right and peripheral branches on the left. There was no evidence of right heart strain. Significant bilateral pneumonia and pneumomediastinum were better visualized in the lung window shown in Fig. 3
By hospital day 16, his oxygen requirement decreased to 3 L/minute by nasal cannula. The pneumomediastinum, pneumothorax, and subcutaneous emphysema reduced with the VAC therapy (Figs. 2 and 3) and remained stable after VAC removal. He was discharged with dabigatran, tapering steroids, and home oxygen.
The patient completed 3 months of dabigatran, underwent home physical rehabilitation, and showed significant clinical improvement. At the 3-month follow-up, he had weaned off supplemental oxygen, returned to normal activities and work, and could walk 10,000 steps daily. Repeat chest radiography showed complete resolution of the pneumothorax and significant improvement in lung opacity (Fig. 1B).
Discussion
The clinical presentation of COVID-19 is highly variable, and our understanding continues to evolve. Concomitant spontaneous pneumomediastinum, pneumothorax, and subcutaneous emphysema are rare, accounting for less than 1% of COVID-19 complications [3, 4]. However, their concurrent presentation results in a high mortality rate of up to 26% [5], necessitating high clinical vigilance even in patients who are not mechanically ventilated.
A spontaneous pneumothorax refers to gas in the pleural space without an external event. It is classified as primary (no underlying lung disease) and secondary (complication of existing lung disease). A large pneumothorax may be accompanied by subcutaneous emphysema. Nearly all lung diseases can lead to secondary spontaneous pneumothorax, with chronic obstructive pulmonary disease being the most common cause, followed by tuberculosis in endemic areas [6]. The first occurrence of spontaneous pneumothorax in patients with COVID-19 was reported in Wuhan, China, found in 5.9% of intubated patients [7]. Subsequent case series later reported varying incidences in patients with COVID-19 [8–10]. The presumed pathophysiological mechanism involves direct invasion and necrosis of lung tissue, including the pleura, by SARS-CoV-2, causing air leak due to extensive diffuse alveolar damage, followed by alveolar rupture [11]. The risk correlates with the severity of the infection [12–16].
Pneumomediastinum can occur with or without pneumothorax and is a marker of severe COVID-19 infection. A sevenfold increase in pneumomediastinum incidence has been associated with COVID-19 compared with non-SARS-CoV-2 infection [17]. In the UK, pneumomediastinum was identified in 0.64% of COVID-19 inpatients, with a 120-day mortality of 51.7% [18]. A Romanian study reported an incidence of 0.86% among COVID-19 inpatients [19]. About half of these cases were not associated with mechanical ventilation at the time of diagnosis [18–20].
The risk factors for spontaneous pneumothorax or pneumomediastinum in COVID-19 are not fully understood. Although more than half of these complications were not linked to positive-pressure ventilation, barotrauma was commonly attributed as the primary cause and a significant predictor of mortality [18]. The incidence of pneumothorax is higher in males [21]. High serum lactate dehydrogenase levels are associated with pneumomediastinum [5]. History of smoking, known pulmonary pathology, and viral load do not appear to increase the risk [4, 6].
Our patient initially presented with intractable hiccups, a known risk factor for spontaneous pneumomediastinum [22, 23] and an atypical presentation of COVID-19 [24, 25]. His pneumothorax and pneumomediastinum developed after a coughing spell. Severe and persistent hiccups, forceful coughing, vomiting, sneezing, excessive straining, or asthma exacerbation can elevate intrathoracic pressure, triggering pneumomediastinum by the Macklin effect. The co-occurrence of hiccups and acute hyponatremia, as seen in our patient, has been reported as a unique manifestation of COVID-19 [26, 27]. Intractable hiccups in COVID-19 should be promptly addressed to reduce the risk of pneumothorax or pneumomediastinum.
No guidelines exist for managing spontaneous pneumothorax or pneumomediastinum in patients with COVID-19. High clinical vigilance is crucial for early diagnosis in any patient with COVID-19 with sudden onset chest pain or respiratory distress. Management options, based on etiology, for spontaneous pneumothorax and pneumomediastinum in COVID-19 infection, have been recently reviewed elsewhere [28, 29]. Briefly, for unstable patients, needle decompression or emergent chest tube placement should be performed. For stable patients, supplemental oxygen and removal of air by chest tube or catheter thoracostomy are recommended. Conservative measures such as oxygen and observation may be reasonable for mildly symptomatic patients. It should be emphasized that high-flow nasal cannula and noninvasive ventilation should be avoided, since these therapies deliver positive pressure to the airway that could potentially perpetuate the air leak. Chlorpromazine has been effective in improving hiccups associated with COVID-19 in a period of 10 hours [30, 31].
Our patient benefited from a blowhole incision connected to VAC, resulting in rapid clinical improvement. This technique was first reported in 1992 for subcutaneous emphysema, where an infraclavicular blowhole incision was made under local anesthesia that could immediately decompress subcutaneous emphysema [32]. However, without negative-pressure therapy, blowholes can collapse owing to clots, tissue recoil, and scarring [33]. Later, negative-pressure wound therapy, known as VAC, introduced by Argenta and Morykwasin in 1997, was leveraged for its capacity to pull air and fluid out of wounds, enhancing healing. VAC placement for subcutaneous emphysema has several advantages. First, VAC is a rapid, minimally invasive therapy that can be performed at the bedside with local anesthesia. Second, VAC allows for constant air aspiration, lung expansion, and early apposition of the pleura surfaces, leading to rapid improvement of respiratory improvement. Previous cases showed subcutaneous emphysema can resolve within 2–4 days of VAC therapy [34] compared with several weeks with observation alone. Third, VAC also improves blood flow, reduces edema, promotes granulation tissue formation, and decreases inflammatory mediators.
Benefits of VAC therapy should be viewed cautiously owing to the paucity of reports, and adverse effects should be considered. Pain at the wound site is the most common complication of VAC therapy, which is usually controlled by adjusting the pressure [34]. Other less common adverse effects for VAC treatment, usually inappropriately managed system, include bleeding, infection, tissue damage, allergic reaction to materials, fistula formation, wound dehiscence, and reopening of the wound [35–37].
The bilateral PE in our patient was expected, given the hypercoagulable state associated with COVID-19 that can cause thromboembolism [38]. However, the concomitant occurrence of pneumomediastinum, pneumothorax, subcutaneous emphysema, and extensive PE in COVID-19 is exceedingly rare, with only one previously reported case, which was fatal [39].
The prognosis of concomitant spontaneous pneumothorax and pneumomediastinum in patients with COVID-19 is poor, with a mortality rate of up to 26% [5]. Factors associated with higher mortality include mechanical ventilation, older age, and diabetes mellitus [18, 21]. One study indicated a higher mortality among females, patients with body mass index ≥ 30 kg/m^2^, those who were intubated, and those with pre-existing lung disease [20].
Conclusion
This case highlights the risk for developing spontaneous pneumothorax and pneumomediastinum in patients with COVID-19 pneumonia, even in the absence of positive-pressure ventilation. Reversible risk factors, such as maneuvers that elevate intrathoracic pressure, should be closely monitored and promptly addressed to prevent severe respiratory complications. A high level of clinical vigilance and early imaging are essential for early diagnosis. Negative-pressure therapy, such as VAC, can be promptly implemented at bedside, leading to a favorable clinical outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.