Clip-assisted anchoring method to facilitate submucosal tunnel entry in peroral endoscopic myotomy for severe fibrosis
Kazuki Yamamoto, Yohei Nishikawa, Kohei Shigeta, Kei Ushikubo, Ippei Tanaka, Satoshi Abiko, Haruhiro Inoue

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
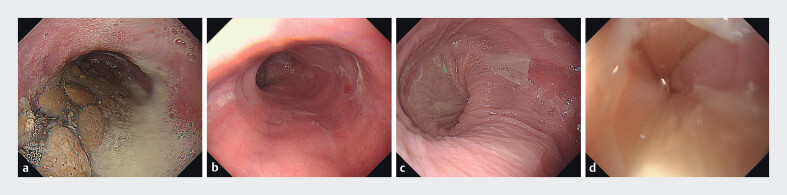 Fig. 1
Fig. 1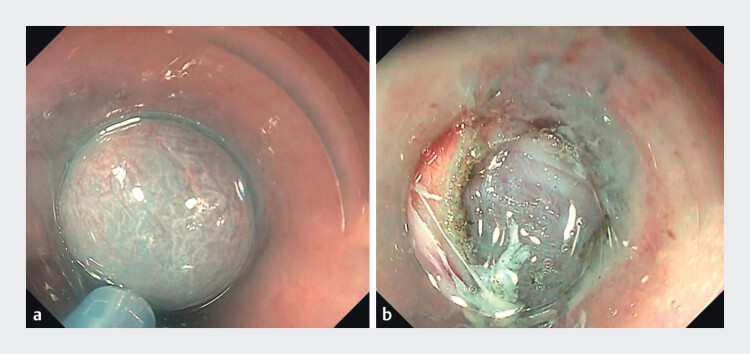 Fig. 2
Fig. 2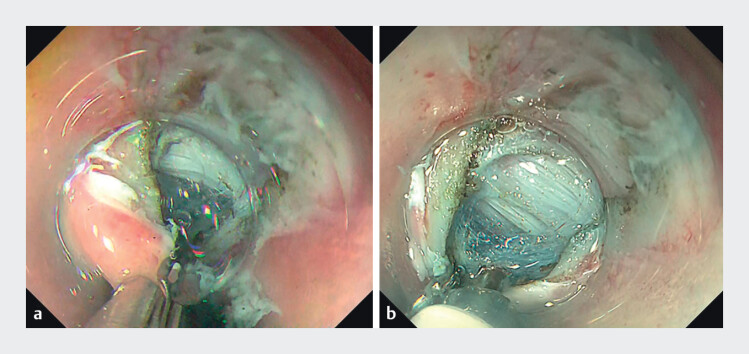 Fig. 3
Fig. 3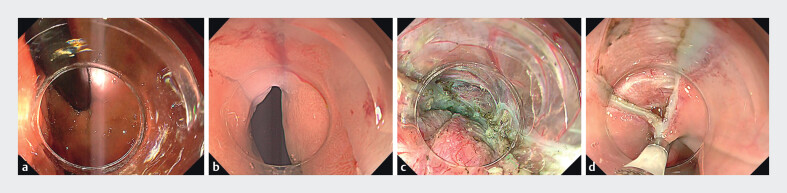 Fig. 4
Fig. 4 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDysphagia Assessment and Management · Cervical and Thoracic Myelopathy · Gastroesophageal reflux and treatments
Peroral endoscopic myotomy (POEM) is an established treatment for esophageal achalasia, with technical success rates of 90% to 100% 1 2 3 . However, severe submucosal fibrosis (SMF) can make submucosal tunnel entry challenging and may lead to procedure failure 4 . Therefore, we developed the Clip-assisted Anchoring Method to secure a stable foothold for the endoscope, improving tunnel entry in difficult SMF cases.
A 27-year-old woman with type I achalasia ( Fig. 1 a-d ) underwent POEM using a therapeutic endoscope (GIF-H290; Olympus) with a Triangle Tip Knife J (TTJ; Olympus) and an electrosurgical unit (VIO3; ERBE, Endocut I: 1–3-3). A submucosal injection and mucosal incision were made at the 2 o’clock position; however, severe SMF limited the lifting effect, causing the scope to slip and making tunnel entry challenging ( Fig. 2 a,b ). Applying a single endoclip (HX-610–090; Olympus) to the distal edge of the incision created a stable anchoring point, markedly improving stability, visualization, and allowing smooth, controlled entry ( Fig. 3 a,b ).
a Achalasia patient before peroral endoscopic myotomy (POEM) showing massive food residue in the esophagus. b Esophageal lumen after clearance of the food residue prior to POEM. c Inflamed esophageal mucosa with epithelial damage and peeling. d Rosette-like appearance of the lower esophagus.
a Submucosal injection showing limited lifting effect due to severe fibrosis. b Severe fibrosis caused the scope to slip, making tunnel entry difficult.
a single endoclip (HX-610–090; Olympus) was applied to the distal edge of the incision, creating a stable anchoring point. b Clip-assisted Anchoring Method improved stability and visualization and enabled smooth, controlled entry.
Once entry was achieved, submucosal dissection proceeded along the lesser curvature. The double-scope technique 5 was used to confirm tunnel length and orientation in both retroflexed and forward views. Myotomy was completed at the distal tunnel, and the entry site was fully closed with endoclips ( Fig. 4 a-d and Video 1 ).
a Submucosal dissection proceeded along the lesser curvature. The double-scope technique confirmed tunnel length and orientation in a retroflexed view. b Forward view using the double-scope technique showing the submucosal tunnel along the lesser curvature of the stomach. c Myotomy was completed at the distal end of the submucosal tunnel. d The entry site was completely closed with endoclips (HX-610–090; Olympus).
Clip-assisted Anchoring Method for Tunnel Entry in POEM.Video 1
The patient had an uneventful recovery. A postoperative barium swallow showed improved esophageal emptying at the lower esophageal sphincter ( Fig. 5 a,b ). Clear liquids were started on day 1, followed by gradual diet advancement. Symptoms resolved and she was discharged on day 4.
a Barium swallow before peroral endoscopic myotomy (POEM). b Barium swallow after POEM.
This case demonstrates that the Clip-assisted Anchoring Method, by placing a clip at the distal edge of the submucosal incision, provides a stable anchor for the endoscope and enables successful tunnel entry in POEM even with severe fibrosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Inoue H Minami H Kobayashi Y Peroral endoscopic myotomy (POEM) for esophageal achalasia Endoscopy 20104226527110.1055/s-0029-124408020354937 · doi ↗ · pubmed ↗
- 2Shiwaku H Inoue H Sato H Peroral endoscopic myotomy for achalasia: a prospective multicenter study in Japan Gastrointest Endosc 2020911037104410.1016/j.gie.2019.11.02031759035 · doi ↗ · pubmed ↗
- 3Tan S Zhong C Ren Y Efficacy and safety of peroral endoscopic myotomy in achalasia patients with failed previous intervention: A systematic review and meta-analysis Gut Liver 20211515316732616678 10.5009/gnl 19234 PMC 7960968 · doi ↗ · pubmed ↗
- 4Wu QN Xu XY Zhang XC Submucosal fibrosis in achalasia patients is a rare cause of aborted peroral endoscopic myotomy procedures Endoscopy 20174973674410.1055/s-0043-11344028658680 · doi ↗ · pubmed ↗
- 5Baldaque-Silva F Marques M Vilas-Boas F New transillumination auxiliary technique for peroral endoscopic myotomy Gastrointest Endosc 20147954454510.1016/j.gie.2013.10.02324268533 · doi ↗ · pubmed ↗