A matter arising: When should inflammatory and autoimmune rheumatic diseases be considered ‘early’?
Elvis Hysa, Emanuele Gotelli, Carmen Pizzorni, Sabrina Paolino, Alberto Sulli, Vanessa Smith, Rosanna Campitiello, Maurizio Cutolo

TL;DR
This review discusses how to identify early signs of inflammatory and autoimmune rheumatic diseases to improve diagnosis and prevent organ damage.
Contribution
The paper provides updated insights into early diagnostic strategies for rheumatoid arthritis, systemic sclerosis, and large-vessel vasculitis in polymyalgia rheumatica.
Findings
Musculoskeletal ultrasound and MRI can detect early synovitis and bone marrow edema in rheumatoid arthritis.
Raynaud's phenomenon and nailfold capillaroscopy help predict progression to systemic sclerosis.
Imaging reveals subclinical vasculitis in polymyalgia rheumatica, linked to higher relapse rates.
Abstract
Early diagnosis is pivotal for guiding the intensity of clinical monitoring, optimizing therapeutic strategies and preventing organ damage in inflammatory and autoimmune rheumatic diseases (IARDs). This review summarizes current evidence on early diagnostic and therapeutic approaches of some IARDs, including rheumatoid arthritis (RA), systemic sclerosis (SSc) and detection of large‐vessel vasculitis (LVV) in polymyalgia rheumatica (PMR), representing distinct pathophysiological mechanisms of joint synovitis, tissue fibrosis and vasculitis, respectively. A comprehensive narrative literature review was conducted focusing on early recognition strategies, searching PubMed and Scopus databases with emphasis on studies from the past 5 years and recent EULAR/ACR conference abstracts (2023–2025). In RA, clinically suspect arthralgia with seropositivity for rheumatoid factor and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
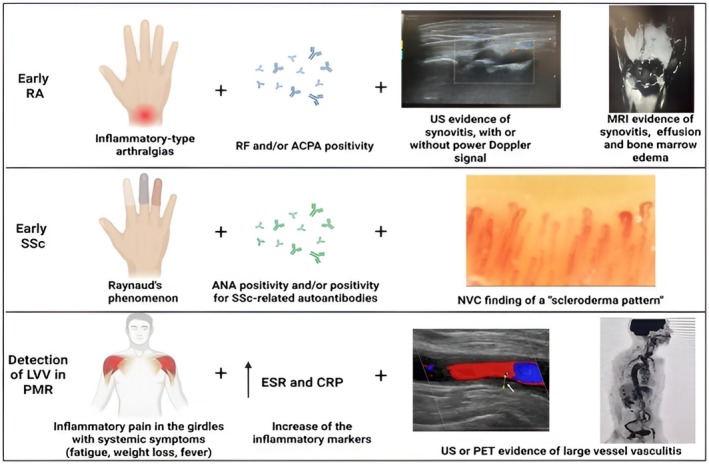 FIGURE 1
FIGURE 1| Finding | Main notes | |
|---|---|---|
| Elements for early diagnosis of RA | ||
| Clinical features | Joint pain | A primary symptom; higher intensity scores are reported in patients diagnosed within 3 months of onset. |
| Morning stiffness | Lasts ≥60 min in the clinically suspect arthralgia phase | |
| Joint swelling | Present in ~75% of cases at initial presentation, typically affecting the small joints of the hands. | |
| Systemic symptoms | Fatigue is a disabling early symptom, reported as severe by 59% of patients at baseline. | |
| Early extra‐articular manifestations | Most frequent include sicca symptoms (~28%) and Raynaud's phenomenon (~17%). Rheumatoid nodules can occur early in 7%–23% of patients. | |
| Laboratory markers | Autoantibodies |
Rheumatoid Factor (RF): Present in 50%–80% of patients ACPA: Present in 60%–80% of patients, with higher specificity (95%–98%) Anti‐CarP antibodies: Found in 20%–40%, but mainly used in research settings |
| Inflammatory markers | ESR and CRP are elevated at diagnosis in approximately 33%–56% of patients, but can be normal in up to 40% of cases | |
| Assessment for early joint involvement and damage | ||
| Imaging: musculoskeletal ultrasound (US) | Subclinical inflammation |
Detects subclinical synovitis in 44%–51% of seropositive individuals with arthralgia. Tenosynovitis: an important early indicator, detected in 63%–85% of early RA patients. |
| Imaging: magnetic resonance imaging (MRI) | Bone marrow edema (BME) | A key predictor of erosive progression, found in 41%–68% of patients in hand and wrist joints |
| Synovitis and tenosynovitis | MRI is highly sensitive, detecting synovitis in 83%–91% and tenosynovitis in 75%–85% of early RA patients | |
| Early erosions | Can be found in 47%–72% of early RA patients with comprehensive multi‐joint MRI protocols | |
| Finding | Main notes | |
|---|---|---|
| Elements for early diagnosis of SSc | ||
| Clinical features | Raynaud's phenomenon (RP) | Often the earliest clinical manifestation, present in over 95% of patients |
| Puffy fingers | A specific early clinical sign, however present in only 18%–39% of patients in VEDOSS cohorts | |
| Skin sclerosis | Skin thickening, the hallmark of SSc, is present in 75% of patients and can begin early, especially in the diffuse cutaneous subset. | |
| Digital ulcers | These painful sores on the fingertips or toes can be an early sign of more severe vascular disease, occurring in 34% of patients. | |
| Musculoskeletal symptoms | Arthralgias (joint pain) are quite common, affecting 40%–60% of patients. Frank arthritis (joint inflammation) can also be seen in up to 16% of cases. | |
| Gastrointestinal symptoms | Issues like reflux, difficulty swallowing, and bloating are very common, affecting up to 71% of patients, and can be an early indicator of internal organ involvement. | |
| Dyspnea | Shortness of breath is reported by 20%–50% of patients and is a critical symptom that may signal the presence of early interstitial lung disease (ILD) or pulmonary arterial hypertension (PAH). | |
| Laboratory markers | Autoantibodies |
Antinuclear antibodies (ANA): A key screening tool, positive in >90% of SSc patients |
| SSc‐specific Autoantibodies | ||
| ACA positive in 20%–35% of SSc patients: Associated with limited cutaneous SSc (lcSSc) and risk of pulmonary arterial hypertension (PAH). Sensitivity 29%–31%, Specificity 87%–97% | ||
| Anti‐Scl‐70 positive in 30%–40% of patients: linked to diffuse cutaneous SSc (dcSSc), frequent digital ulcers, and high risk of severe interstitial lung disease (ILD). Sensitivity 33%–58%, Specificity 95%–99% | ||
| Anti‐RNAPol3 positive in 10%–20% of patients: defines subset with rapidly progressive skin fibrosis, renal crisis, gastric vascular lesions, cancer risk near onset; ILD uncommon. Sensitivity 7%–13%, Specificity 97%–100% | ||
| Anti‐Th/To positive in 2%–5% of patients: associated to lcSSc with high risk of ILD and PAH; associated with shorter lag time between RP and SSc onset128. Sensitivity 2%–4%, Specificity 98%–99% | ||
| Anti‐U3‐RNP (fibrillarin) positive in 2%–8% of patients: frequently seen in Afro‐Caribbean men, associated with early age at onset, PAH, and GI involvement129 Sensitivity 1%–7%, Specificity 97%–100% | ||
| Anti‐PM/Scl positive in 3%–10%: typically seen in SSc–myositis overlap, associated with ILD, calcinosis, dermatomyositis‐like rash, and favourable ILD outcomes in the first decade130. Sensitivity 5%–11%, specificity 93%–98% | ||
| Anti‐Ku positive in 2%–7% of patients: hallmark of PM/SSc overlap syndrome, associated with myositis, ILD, and low prevalence of vascular complications131. Sensitivity 3%–5% and Specificity 96%–98% | ||
| Imaging | Nailfold videocapillaroscopy (NVC) |
The gold standard for assessing SSc‐related microangiopathy. The ‘scleroderma pattern’ is classified into ‘Early’, ‘Active’ and ‘Late’ stages according to disease progression New pre‐scleroderma ‘very early’ NVC changes recognized |
| Baseline assessment for organ involvement | ||
| Imaging and function: Lungs | High‐resolution CT (HRCT) | Mandatory at diagnosis to screen for interstitial lung disease (ILD), even in asymptomatic patients; detects subclinical ILD in ~40%–50% of cases. |
| Pulmonary function tests (PFTs) | Should be performed at baseline and serially for monitoring, but are not sensitive enough for initial screening alone | |
| Imaging: Heart | Transthoracic echocardiography (TTE) | The first‐line screening tool for pulmonary arterial hypertension (PAH) and cardiac involvement at diagnosis. |
| Cardiac MRI | Used in selected cases for a more detailed assessment of myocardial fibrosis or inflammation when echocardiography is inconclusive | |
| Imaging: Skin and peripheral microvasculature | High‐frequency skin US | Can detect early dermal changes (thickness, stiffness); remains a promising research tool requiring further validation. |
| Laser speckle contrast analysis (LASCA) | A research tool for assessing skin perfusion that correlates with NVC findings; not yet standardized for clinical use | |
| Other assessments | Gastrointestinal and renal screening | Tests such as oesophageal manometry or renal ultrasound are not performed routinely at baseline and are reserved for symptomatic patients or when there is clinical suspicion of involvement |
| Finding | Main notes | |
|---|---|---|
| Clinical and laboratory features suggesting underlying LVV in PMR patients | ||
| Clinical and laboratory features suggesting underlying LVV | Constitutional symptoms | Persistent fever, unexplained weight loss, and significant fatigue are present in 30%–50% of cases. |
| Atypical or refractory PMR | Polymyalgic symptoms that are resistant to standard doses of glucocorticoids (e.g. 12.5–15 mg of prednisone) may indicate underlying vascular involvement | |
| Vascular symptoms | Limb claudication, particularly in the upper extremities, can be seen in 10%–20% of patients with extracranial GCA | |
| Laboratory markers | Acute phase reactants | ESR and CRP are elevated in over 90% of patients, though they have limited specificity. |
| Other markers | Increased concentrations of angiopoietin‐2/1 ratios and matrix MMP‐3 might potentially identify GCA in PMR patients but not yet validated for routine clinical use | |
| Trial (intervention) | Population included | Intervention vs. Placebo | Primary outcome | Key results | Follow‐up | Level of evidence/key limitations |
|---|---|---|---|---|---|---|
| RA | ||||||
| APIPPRA | 213 ACPA+ and RF+ patients with inflammatory joint pain | Abatacept 125 mg weekly subcutaneous for 12 months vs. placebo | Time to clinical synovitis in ≥3 joints or RA (2010 criteria) | 6% vs. 29% developed arthritis at 12 months; 25% vs. 37% at 24 months. Sustained improvements in pain, function, and quality of life | 24 months | High (RCT): Strong evidence for prevention with sustained benefit, but the risk of overtreating individuals who would not progress is a key concern |
| ARIAA | 98 ACPA+ patients with arthralgia and inflammation at MRI | Abatacept 125 mg weekly subcutaneous for 6 months vs. placebo | Proportion with improved MRI inflammation at 6 months | 57% vs. 31% showed MRI improvement; 8% vs. 35% developed RA during treatment (HR 0.14) | 18 months | High (RCT): Reduced MRI inflammation and RA progression in a high‐risk group, but the smaller sample size and use of a surrogate primary endpoint are limitations |
| PRAIRI | 81 ACPA+ and RF+ patients with arthralgia | Single infusion of rituximab 1000 mg vs. placebo | Time to development of clinical arthritis | 55% risk reduction at 12 months (HR 0.45), 12‐month delay in arthritis development, but no sustained effect | 29 months mean | Moderate (RCT): The effect was temporary, suggesting the intervention postponed but did not permanently alter the disease course |
| TREAT EARLIER | 236 patients with arthralgia and MRI subclinical inflammation | Single glucocorticoid injection + methotrexate up to 25 mg/week for 1 year vs. placebo | Development of clinical arthritis (2010 RA criteria or ≥2 joints) persisting ≥2 weeks | No prevention of arthritis (19% vs. 18%, HR 0.81), but sustained improvement in pain, function, and MRI inflammation | 2 years | Moderate (RCT): Did not meet its primary prevention endpoint, but provides good evidence for modifying the disease burden rather than intercepting the disease |
| StopRA Trial | 142 anti‐CCP3+ individuals | Hydroxychloroquine 200‐400 mg daily vs. placebo for 1 year | Development of inflammatory arthritis classified as RA or IA with ≥1 erosion | No difference: 34% HCQ vs. 36% placebo developed RA at 3 years ( | 3 years | Low (RCT‐Halted): Findings are from an interim analysis that showed a clear lack of benefit, leading to the trial's termination |
| Bos et al | 83 ACPA+/RF+ patients with arthralgia | Two intramuscular dexamethasone injections (100 mg each) vs. placebo | 50% reduction or normalization of autoantibody levels at 6 months | ACPA reduced 22% and IgM‐RF 14% vs. placebo, but no difference in arthritis development (20% vs. 21%) | 26 months median | Low (RCT): A small trial with a very brief intervention that showed no impact on the clinical outcome of arthritis development. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Sclerosis and Related Diseases · Systemic Lupus Erythematosus Research · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
INTRODUCTION
1
Early, and when possible, very early, diagnosis of inflammatory and autoimmune rheumatic diseases (IARDs) is crucial to minimize the impact of recognized trigger factors and to allow for timely, appropriate management strategies. These may include close monitoring and/or early therapeutic intervention, with the goal of preventing progressive and irreversible organ damage.
Healthcare professionals involved in the management of these conditions should be familiar with the initial clinical manifestations, as well as laboratory markers and imaging findings, which can support prompt therapeutic decisions or closer monitoring to anticipate the evolution toward overt disease.
In this narrative review, we explore the current understanding of very early/early diagnosis of rheumatoid arthritis (RA), systemic sclerosis (SSc) and large vessel vasculitis (LVV) in patients with polymyalgia rheumatica (PMR).
These conditions were selected to represent inflammatory and ARDs with distinct pathophysiological mechanisms, namely synovial inflammation, tissue fibrosis, and vasculitis, respectively. This selection is also informed by the authors' clinical and research expertise in these specific areas. While we acknowledge that other important IARDs, such as systemic lupus erythematosus (SLE) and psoriatic arthritis (PsA), also have well‐characterized preclinical phases, involving the sequential development of autoantibodies or the transition from cutaneous psoriasis to joint inflammation, respectively1, 2, 3 our focused approach allows for an in‐depth discussion of these three core pathological processes.
A thorough narrative literature overview is provided with a major focus on the most recent findings, particularly studies published over the past 5 years, to highlight advances in early recognition and intervention strategies across these diverse conditions.
METHODS
2
This narrative review synthesizes the current evidence on early diagnostic strategies for RA, SSc, and LVV in patients with PMR. A comprehensive search of PubMed and Scopus databases was performed using relevant keywords, including ‘early diagnosis’, ‘rheumatoid arthritis”, ‘systemic sclerosis’, “large vessel vasculitis’, ‘polymyalgia rheumatica’, ‘biomarkers’ and ‘imaging’. While no date restrictions were applied to the database search to ensure an extensive review of the literature, particular emphasis was placed on studies published within the past 5 years to highlight recent advances. Additionally, abstracts presented at the annual congresses of the European Alliance of Associations for Rheumatology (EULAR) and the American College of Rheumatology (ACR) from 2023 to 2025 were screened to capture the most recent findings not yet published as full‐text manuscripts.
Reference lists of included studies were also examined to identify additional relevant publications that may not have appeared in the initial database search. All relevant articles and abstracts were critically appraised, and their contributions to understanding early diagnostic approaches across these distinct diseases were qualitatively synthesized.
The selection process prioritized studies providing high‐quality evidence and significant contributions to the field of early diagnosis and intervention across IARDs. Our inclusion principles favored systematic reviews, meta‐analyses, randomized controlled trials, large population‐based or registry studies, recent national or international guidelines and consensus statements. All relevant articles and abstracts were critically appraised by the authors based on their methodological rigor, relevance to the review's scope and the novelty and impact of their findings. The contributions of each study to the understanding of early diagnostic and therapeutic approaches across these distinct diseases were then qualitatively synthesized.
For interventional studies, a qualitative appraisal of the level of evidence was performed to guide the critical synthesis. This appraisal was based on different factors: the study design, with a strong preference for randomized controlled trials (RCTs); the study's primary outcome, where trials successfully meeting their primary endpoint with a sustained clinical benefit were considered to provide a high level of evidence; and the nature and durability of the effect. Accordingly, RCTs that failed to meet their primary endpoint, demonstrated only a temporary benefit, or were stopped early for futility were graded as providing moderate or low‐level evidence. This structured appraisal was used to contextualize the findings within our manuscript. Although not representing a formal systematic evidence‐grading score, this structured qualitative appraisal aligns with contemporary standards for high‐quality narrative reviews, which emphasize transparent and justified literature selection.4
Definitions of ‘early’ disease across the included IARDs
2.1
To provide a clear framework, the concept of ‘early disease’ is defined for each condition from both a pathophysiological ground and clinical perspectives.
For RA, the pathophysiological onset begins with detectable immune system dysregulation (seropositivity for rheumatoid factor and/or anti‐citrullinated peptide autoantibodies) and/or subclinical synovitis by imaging, potentially years before clinical symptoms.5 Clinical onset refers to the interval from the initial inflammatory joint symptoms up to fulfilment of criteria such as the 2010 ACR/EULAR,6 commonly within 3–12 months of onset, which is considered a critical window for intervention.
For SSc, the pathophysiological phase includes microvascular dysfunction, often presenting as Raynaud's phenomenon (RP) with evidence of a scleroderma‐pattern at nailfold capillaroscopy (NVC) and SSc‐specific serology, prior to skin or organ involvement, as described by the LeRoy/Medsger.7 Clinically, ‘early SSc’ applies to patients meeting these criteria before skin thickening or major organ involvement.
For patients with LVV manifesting with PMR symptoms, the concept of an early phase differs from the progressive models seen in RA and SSc. Unlike those conditions, PMR is not considered a preclinical stage that evolves into GCA; rather, both are viewed as concurrent manifestations of a single disease spectrum.8 Therefore, ‘early detection’ in this context refers to identifying co‐existing, subclinical vasculitis in a patient at or near the time of their PMR diagnosis.9 The pathophysiological onset is the phase where this vessel inflammation is present but clinically silent, detectable only by imaging.10 These patients, now recognized for their higher risk, represent a group potentially in need of tailored management.
RHEUMATOID ARTHRITIS
3
Rheumatoid arthritis (RA) is a chronic autoimmune disease causing persistent joint inflammation, damage, and disability.11 It affects women two to three times more than men when the disease emerges between the third and fifth decades of life.12, 13, 14, 15 Early detection and treatment, even before clinical arthritis appears, are crucial to prevent joint damage.16 In this context, a treat‐to‐target approach aiming for remission or low disease activity helps slow disease progression and reduce long‐term damage.17
While the developmental pathway can vary, RA is often understood to progress through distinct phases, particularly in seropositive individuals. This classic model begins with isolated autoantibody positivity (seropositivity) for rheumatoid factor (RF) or often much earlier anti‐citrullinated peptide antibodies (ACPA), followed by a transition to inflammatory‐type joint pain without visible synovitis (clinically suspect arthralgia) and finally the onset of clinically evident arthritis.16 In contrast, the preclinical cascade in ‘seronegative’ RA may not follow the same pattern and is thought to involve an early increase in pro‐inflammatory cytokines like TNF‐α and IL‐6.18 This phase of inflammatory joint pain without clinical synovitis is often termed ‘clinically suspect arthralgia’. The EULAR definition of ‘arthralgia suspicious for progression to RA’, published in 2017, provides a specific framework for identifying high‐risk individuals.19 This definition includes several clinical features that increase the risk of progression, such as: recent symptom onset, involvement of metacarpophalangeal (MCP) joints, morning stiffness lasting at least 60 min, a predominance of symptoms in the morning, difficulty making a fist and a positive MCP squeeze test. The presence of a family history of RA or RA‐specific autoantibodies further heightens this risk.19, 20
When clinical synovitis appears, the threshold for morning stiffness duration decreases to 30 min. The Early Rheumatoid Arthritis (ERA) criteria, requiring at least three of five items: morning stiffness ≥30 min, arthritis in ≥3 joint areas, hand joint arthritis, positive RF, positive ACPA and improve early diagnosis sensitivity (84.4% vs. 58% of older criteria), enabling timely treatment.21, 22
Articular, systemic and extra‐articular symptoms of early rheumatoid arthritis
3.1
Joint pain is typically the first symptom reported by patients with early RA. Recent data suggest that individuals diagnosed within 3 months of symptom onset experience higher pain intensity compared to those with longer diagnostic delays. This association is likely to reflect the fact that more severe pain and functional limitations prompt patients to seek medical care more promptly, leading to an earlier diagnosis23 (see Table 1).
Symmetrical joint swelling, especially involving the small joints of the hands, is present in approximately 75% of cases, although about 25% present with an asymmetrical pattern, which can complicate early recognition.23, 25
Night pain and sleep disturbances, linked to nocturnal inflammation and altered circadian rhythms, are also frequently reported in the early phase of RA.37
Among the systemic features, fatigue is one of the most disabling symptoms in early RA, reported as severe by 59% and moderate by 19% of patients at baseline.38 In about 25% of cases, it persists over 5 years despite good disease control.26 Indeed, improvement in fatigue often lags behind clinical remission by up to 6 months, suggesting mechanisms beyond synovial inflammation.38
Extra‐articular manifestations (ExRA) can be a key feature of early RA, affecting 23%–41% of patients at or near diagnosis.39
The most frequent early ExRA include sicca symptoms (28%), RP (17%) and rheumatoid nodules, which can affect up to 23% of patients, particularly seropositive smokers.28, 39, 40 While more severe manifestations can occur, they are less common at initial presentation; for instance, subclinical interstitial lung disease (ILD) may be detectable and rheumatoid vasculitis is rare (<1%) in early disease.28, 39, 41
Laboratory markers
3.2
Anti‐citrullinated peptide antibodies (ACPA) and RF are the most established serological biomarkers for early RA. ACPAs offer greater specificity (90%–96%) compared to RF (70%–80% sensitivity but lower specificity), and both can precede clinical onset by several years (up to 15 years).42
Their combined presence markedly increases the risk of progression, particularly in individuals carrying the HLA‐DRB1 shared epitope. This genetic motif, located within the major histocompatibility complex (MHC) class II region, enhances antigen presentation of citrullinated peptides to autoreactive T cells and represents the strongest known genetic risk factor for RA development.43
Inflammatory markers are variably elevated at diagnosis: erythrocyte sedimentation rate (ESR) is increased in about 53%–55% and CRP in approximately 42%–56% of early RA patients, but both can be normal in up to 40% of cases.30, 31 This highlights the limited sensitivity of acute‐phase reactants and the need for integrating clinical, serological and imaging findings in early diagnostic assessment.
Imaging Features
3.3
Imaging modalities such as ultrasound (US) and magnetic resonance imaging (MRI) enhance early RA diagnosis and monitoring by detecting subclinical inflammation and structural changes not evident on clinical examination.32
Compared to conventional radiography, US and MRI provide more sensitive information on inflammatory and soft tissue changes, including synovitis, joint effusion and early bone erosions (Figure 1). Baseline X‐rays of hands and feet are valuable for identifying pre‐existing structural damage and determining whether the disease is already erosive. However, their limited sensitivity in identifying active synovitis or early lesions makes US and in particular, MRI more suitable for capturing early inflammatory changes.32
Combination of clinical features, laboratory, and imaging findings in early RA, SSc, and in the detection of LVV in patients with PMR. Illustration created with www.biorender.com and Microsoft PowerPoint. All images, except the vascular ultrasound in the lower panel, are original and belong to the Academic Division of Clinical Rheumatology, University of Genova, Italy. The vascular ultrasound image is reproduced from Schäfer VS. Curr Rheumatol Rep. 2023; 25 (9):279–289, licensed under a Creative Commons Attribution 4.0 International Licence (CC BY 4.0). 44 CRP, C‐reactive protein; ESR, erythrocyte sedimentation rate; LVV, large vessel vasculitis; MRI, magnetic resonance imaging; PET, positron emission tomography; RA, rheumatoid arthritis; SSc, systemic sclerosis; US, ultrasound.
Applications of musculoskeletal ultrasound in early RA
3.3.1
Musculoskeletal ultrasound (US) plays a central role in early RA, improving diagnostic accuracy and supporting risk stratification in individuals with musculoskeletal symptoms. In seropositive patients without clinical arthritis, ultrasound abnormalities (grey scale synovitis, power Doppler signals, and erosions) can detect subclinical synovitis in 44%–51% of cases.
Notably, among ACPA‐positive individuals who later develop RA, approximately 80% have evidence of subclinical inflammation on imaging before the onset of inflammatory arthritis.45 A power Doppler score >2 (based on the semiquantitative OMERACT grading system) has been associated with an increased risk of progression to clinical arthritis, particularly in individuals who are double‐positive or at imminent risk of disease onset.32, 33, 46 Furthermore, recent studies have identified that the number of joints with subclinical inflammation is a key predictive factor, which, when combined with the presence of autoantibodies and an elevated ESR, is strongly associated with irreversible progression to RA.47
Recent studies underscore the critical role of musculoskeletal US in detecting subclinical inflammation and early structural changes among individuals at risk for RA, even before the clinical onset of overt synovitis. It has been demonstrated that power Doppler US not only detects subclinical synovitis but can also reveal bone erosions and loss of hyaline cartilage, which are critical markers of structural damage and predictors of persistent or progressive RA in patients with clinically suspect arthralgia. The presence of these US‐detected erosions, even in the absence of clinical arthritis, has been associated with a higher likelihood of disease progression, supporting US as a valuable tool for risk stratification and as an adjunct to serological and clinical assessment during the preclinical phase.48
Additionally, semiquantitative scoring systems, such as those developed by the OMERACT working groups, allow for standardized evaluation of both inflammation and early structural changes (cartilage loss, erosions) at sites most affected in early RA, particularly within the metacarpophalangeal joints. While bone erosions have historically been considered a late finding, emerging evidence confirms that US can detect subtle cortical breaks earlier than standard radiographs. Collectively, these findings emphasize the relevance and feasibility of US in both research and clinical practice for early detection, prognostication, and potential disease interception in preclinical RA.49
Additionally, the detection of tenosynovitis is becoming increasingly important in the assessment of patients with inflammatory joint pain.50 Compared to previous years, tenosynovitis is no longer considered merely an additional disease feature, but rather an early indicator that may even precede joint synovitis. Indeed, the identification of hand and foot tenosynovitis by MRI has been incorporated into the recent 2025 EULAR/ACR classification criteria for individuals with arthralgia at risk for RA.51
In patients with undifferentiated arthritis or equivocal clinical findings, US can confirm active synovitis and guide early therapeutic decisions. However, in the absence of clinical or serological inflammation, treatment should not be based solely on imaging findings to avoid overtreatment. Instead, US should be integrated with clinical and laboratory data, with a preference for close follow‐up and repeat imaging as needed.52
Applications of MRI in early RA
3.3.2
MRI offers greater sensitivity than ultrasound in detecting early inflammatory changes, particularly bone marrow edema, a hallmark of imminent erosive progression that cannot be visualized by ultrasound.53 It is especially useful in cases of diagnostic uncertainty, when clinical and ultrasound findings are discordant or limited by technical factors (e.g. deep joints, obesity, or poorly accessible areas).54 MRI can also assist in differentiating RA from other inflammatory arthritides through detailed evaluation of synovitis and tenosynovitis.31
Of note, a recent observational study highlighted the need for cautious interpretation of MRI‐detected erosions in patients with clinically suspect arthralgia, as these findings did not correspond with radiographic erosive disease or disease progression, unless accompanied by subclinical inflammation, which showed a stronger association (OR 6.29 [95% CI 2.94–13.48]).35
It is also important to recognize that these inflammatory findings, such as synovitis and bone marrow edema, are not static and may regress, particularly with therapeutic intervention as seen in prevention trials (for more details, see Section 3.5).
Indeed, due to high cost, limited accessibility and longer acquisition times, MRI is not routinely used in clinical practice and remains a second‐line tool in early RA, particularly when imaging findings are expected to impact diagnostic or therapeutic decisions.
Predictive models for the future development of RA
3.4
In response to the need for targeted prevention and early intervention, several predictive models and risk stratification tools have been developed worldwide to estimate the likelihood that individuals with preclinical features or undifferentiated arthritis will progress to RA.
The Leiden Prediction Rule, developed in the Netherlands, is one of the most widely validated clinical prediction tools. This model integrates clinical parameters (such as joint involvement, symptom duration, morning stiffness), serological markers (ACPA, RF) and acute phase reactants to generate a weighted score corresponding to the probability of developing RA within 1 year. In both Western and non‐Western populations, a score ≥8 confers a high risk (approaching 100% in some cohorts), while a low score (<5) is associated with an excellent prognosis. The rule has shown strong predictive accuracy, with area under the curve (AUC) values ranging from 0.85 to 0.90.55
UK Risk Algorithms and other multivariate models such as the Swedish Epidemiological Investigation in RA have also been validated, incorporating demographic, clinical and serological data to predict RA in referred patients with early or undifferentiated arthritis. Some models also consider genetic risk scores or incorporate environmental factors such as smoking status.56
The EULAR/ACR 2025 Risk Stratification Criteria, previously mentioned, represent the latest consensus approach, derived from a collaborative analysis of 10 major international arthralgia cohorts (n > 2500 at‐risk subjects). This model provides a stepwise scoring system using clinical factors (morning stiffness, self‐reported joint swelling, difficulty making a fist), laboratory variables (CRP, RF, ACPA) and, optionally, MRI findings (especially tenosynovitis) to stratify patients by their likelihood of developing RA within 1 year. The inclusion of MRI‐detected subclinical inflammation further improves predictive value, with models achieving AUCs as high as 0.93. The criteria are designed to be applied flexibly, depending on the availability of imaging and serological resources, and support the selection of homogeneous risk groups for clinical trials or early intervention programs.51
Early intervention in rheumatoid arthritis
3.5
There is growing interest in strategies to delay or prevent clinical RA in high‐risk individuals, particularly those with arthralgia, seropositivity and imaging signs of subclinical inflammation. Several randomized trials have explored pharmacological interventions in this preclinical phase (Table 4).
The most compelling evidence for prevention comes from high‐quality randomized controlled trials (RCTs) targeting T‐cell co‐stimulation with abatacept. The APIPPRA and ARIAA trials showed that abatacept significantly reduced progression to RA, with a sustained benefit observed even 1 year after treatment discontinuation.57, 58 This supports the concept that early targeting of T‐cell co‐stimulation is a key preventive strategy.59 However, these trials also highlight a critical challenge, as a substantial proportion of individuals in the placebo arms (ranging from 43% to 63%) did not develop RA, raising concerns about potential overtreatment.
It is also important to contextualize these promising results. Longer‐term follow‐up from the ALTO study, the open‐label extension of APIPPRA, suggests the intervention primarily delays rather than permanently prevents RA onset. After treatment cessation, the cumulative incidence of arthritis in the original abatacept group began to converge with the placebo arm over the following year. Furthermore, the most significant and sustained benefit was concentrated in a hyper‐seropositive subgroup with a high antigenic burden, defined by positivity for five distinct autoantibody specificities (IgG ACPA, IgA ACPA, IgM RF, anti‐CarP, anti‐PAD antibodies).60 Since this specific antibody profile is not assessed in routine clinical practice, the broad applicability of this preventive strategy remains a challenge. These findings underscore the need for refined stratification tools to identify individuals most likely to achieve a durable benefit from early intervention.
Other strategies have yielded more limited effects, providing moderate‐level evidence. In the PRAIRI trial, the B‐cell depleting agent rituximab only temporarily delayed the onset of RA by approximately 12 months but failed to prevent it in the long term, as the cumulative incidence eventually converged with the placebo group.61
Similarly, the TREAT EARLIER study failed to meet its primary endpoint, as methotrexate plus glucocorticoids did not prevent the incidence of clinical arthritis. However, the treatment did lead to sustained improvements in symptoms, function and MRI inflammation, suggesting a role in modifying the disease burden rather than intercepting the disease itself.62
Finally, some approaches have provided low‐level evidence with no clear preventive benefit. The StopRA trial investigating hydroxychloroquine was stopped prematurely for futility after an interim analysis showed it was no better than placebo.63, 64 A trial by Bos et al. showed that a brief intervention with intramuscular dexamethasone in a small cohort produced only transient immunological effects without impacting the rate of arthritis development.65
Despite encouraging signals for targeted immunomodulation, particularly with abatacept, important challenges remain. The role of environmental risk factors, such as diet, smoking, certain beverages and even exogenous hormone use (e.g. oestrogens or hormone replacement therapy), should be carefully evaluated and if possible, correctly addressed early as part of preventive management.
Many at‐risk individuals will never develop RA, raising concerns about overtreatment. Moreover, predictive tools to identify those who would benefit most from early therapy are still suboptimal, and long‐term safety and cost‐effectiveness remain to be established.
Therefore, early intervention in seropositive individuals with subclinical inflammation shows promise, but further research is needed to refine patient selection and optimize combined therapeutic strategies in RA.
SYSTEMIC SCLEROSIS
4
Systemic sclerosis (SSc) is a rare and progressive autoimmune disease mainly affecting young to middle‐aged women, marked by immune dysfunction, microvascular damage, and progressive fibrosis of skin and internal organs.66 Despite its low worldwide prevalence (approximately 18 per 100,000 people), it has the highest mortality among rheumatic diseases, with prognosis depending on organ involvement.67
Clinically, SSc is classified into limited (lcSSc) and diffuse (dcSSc) cutaneous forms, which differ in severity and timing of organ complications68: dcSSc often leads to early and faster lung, heart or kidney involvement, while lcSSc progresses more slowly, with later pulmonary and gastrointestinal manifestations.69, 70
Clinical Features of early systemic sclerosis
4.1
Raynaud's phenomenon (RP) is often the earliest clinical manifestation of systemic sclerosis (SSc) and is characterized by episodic vasospasm of the digital arteries, typically triggered by cold or emotional stress. Clinically, it presents with a triphasic sequence of colour changes in the digits: pallor (ischemic phase) due to arterial vasoconstriction, followed by cyanosis (hypoxic phase) as deoxygenated blood pools in the venous system, and finally rubor (reperfusion phase) upon rewarming and restoration of blood flow.71
Although RP affects approximately 3%–5% of the general population, the vast majority of these cases are primary (idiopathic) and non‐progressive. However, a small proportion of patients (almost 14.6%) with RP develop secondary forms, most commonly in association with autoimmune connective tissue diseases such as SSc, and/or overlap connective tissue diseases (CTDs). In SSc, RP is not merely functional but reflects underlying structural microvascular abnormalities, including endothelial dysfunction, intimal vessel proliferation, obliterative vasculopathy and capillary loss, which explain its severity, chronicity and progression.72
To distinguish primary from secondary RP, imaging analysis is obtained with nailfold videocapillaroscopy (NVC) that is a fundamental non‐invasive tool. The identification of a characteristic ‘scleroderma pattern’ on NVC is a cornerstone of early diagnosis and a key component of the 2013 ACR/EULAR classification criteria for SSc (see Section 4.3 for a detailed description of imaging patterns).73, 74
The pivotal criteria for early systemic sclerosis (2001) by LeRoy and Medsger represent a valuable clinical framework for identifying patients in the initial stages of the disease, particularly among those presenting with RP.7 By emphasizing the combination of RP, SSc‐specific autoantibodies, and abnormal nailfold capillaroscopy findings, these criteria enable clinicians to recognize systemic sclerosis before overt skin or internal organ involvement emerges.
The subsequent study by Koenig et al. followed 586 patients with RP over a 20‐year period and demonstrated that the presence of both SSc‐specific autoantibodies (e.g. anti‐CENP‐B, anti‐topoisomerase I, anti‐RNAP III, anti‐Th/To) and a scleroderma‐type NVC pattern significantly increased the risk of progression to definite SSc (79.5% developed SSc; median time to progression 4.6 years; HR 60.08 versus patients with neither predictor).75 This study validated the study of LeRoy and Medsger.
Building upon the conceptual groundwork laid by LeRoy and Medsger, the Very Early Diagnosis of Systemic Sclerosis (VEDOSS) initiative, launched by the European Scleroderma Trials and Research (EUSTAR) group in 2011, further expanded the previous framework to enable very early identification of SSc in patients with RP.76
Unlike earlier criteria, VEDOSS introduced puffy fingers as a specific early clinical sign, often preceding skin fibrosis and associated with a higher risk of dcSSc.77, 78 However, the diagnostic utility of puffy fingers may vary in clinical practice, especially in ANA‐negative individuals. For example, in the EUSTAR‐VEDOSS cohort, puffy fingers were reported only in 38.5% of ANA‐positive patients but only 23.3% of ANA‐negative patients with Raynaud's.79
Moreover, puffy fingers are not exclusive to SSc and may also appear in overlap syndromes such as undifferentiated connective tissue disease (UCTD) or mixed connective tissue disease (MCTD), for the latter disease being recognized as early and diagnostic clinical manifestations in validated criteria.80 This underscores the need for careful differential diagnosis in very early presentations.
Recent data from two large U.S. cohorts, GENISOS and CONQUER, challenge the idea that RP is the most common initial symptom of SSc. Between 31% and 44% of patients first showed non‐RP signs like puffy fingers or hand swelling, often linked to diffuse cutaneous SSc, joint contractures and RNA Polymerase III antibodies. This pattern was especially frequent in Black patients, where RP; however, can be harder to detect.81, 82
These results highlight the need to recognize non‐RP presentations as an early disease form in some populations (see Table 2). However, without systematic microvascular assessments such as NVC, early microvasculopathy may be missed and at least early diagnosis compromised; see 2013 ACR/EULAR classification criteria for SSc.73, 74 Genetic, environmental, and healthcare differences also limit applying these findings to other populations.
Recent NVC studies are starting to identify ‘very early’ pre‐scleroderma microvascular changes (‘very early’ and progressive capillary dilations up to giant validated capillaries) in SSc patients with RP, which may offer further insight.89
Laboratory Features
4.2
Serological evaluations are pivotal in the identification of early SSc, particularly among patients initially presenting with RP. ANA are present in over 90% of SSc patients and represent a key screening tool. However, a subset of patients with ANA‐negative SSc has also been described, often characterized by less vasculopathy but more severe gastrointestinal involvement and worse prognosis.97
Among disease‐specific autoantibodies, the most widely recognized and clinically useful are anti‐centromere (ACA), anti‐topoisomerase I (anti‐Scl70), and anti‐RNA polymerase III (anti‐RNAPol3).98 Not only do these antibodies aid the diagnosis, but they also enable clinical and prognostic stratification.
ACA is typically associated with the limited cutaneous subset (lcSSc) and a higher risk for future pulmonary arterial hypertension (PAH).99, 100
Anti‐Scl‐70 antibodies are highly specific for SSc and are linked to the diffuse cutaneous subset (dcSSc), with an increased risk of severe interstitial lung disease (ILD).69
Anti‐RNAPol3 antibodies also mark a diffuse cutaneous subset, often with rapid skin progression and a significant risk for developing scleroderma renal crisis.101
In addition to these classical markers, novel SSc‐related autoantibodies have been described such as anti‐eIF2B, anti‐RuvBL1/2, anti‐U11/U12 RNP (RNPC3) and anti‐BICD2 in up to 10% of so‐called ‘seronegative’ patients, often associated with aggressive or overlapping disease phenotypes, including ILD, myopathy, severe GI or myocardial involvement and, in the case of RNPC3 and eIF2B, possible paraneoplastic syndromes.87
The accurate detection of these autoantibodies requires appropriate methods. Indirect immunofluorescence (IIF) on HEp‐2 cells remains the standard for ANA screening, but many SSc‐specific antibodies require more refined techniques such as immunoblotting, multiplex line immunoassays, or immunoprecipitation (the latter more rarely applied) to be reliably identified.87
Imaging findings in early SSc
4.3
Imaging of the microvasculature and internal organs plays a central role in the early identification and monitoring of SSc. Among the morphological tools assessing peripheral microcirculation, NVC remains the gold standard for evaluating structural microvascular abnormalities in patients with RP102 (Figure 1).
The typical ‘scleroderma pattern’ observed in SSc has been classified and standardized by Cutolo et al. in 2000 into ‘early’, ‘active’ and ‘late’ stages following the pathophysiological evolution of SSc microangiopathy.88 The ‘early’ pattern is marked by a few giant capillaries and mild haemorrhages with preserved density; the ‘active’ pattern includes frequent haemorrhages and moderate capillary loss; and the ‘late’ pattern is defined by severe capillary loss, disorganized architecture and neoangiogenesis.103, 104 This structured classification allows both diagnostic and prognostic use of NVC in early SSc.
More recently, the detection of a capillary with a diameter >30 μm and <50 μm (at least two capillaries per linear mm at NVC) in patients with Raynaud's phenomenon, before the development of a full‐blown scleroderma pattern, has been proposed as a ‘pre‐scleroderma signature’, indicative of a ‘very early’ step of SSc.89 However, this finding is under further validation in prospective cohorts before it can be fully integrated into routine clinical assessment.
In addition to the morphological assessment, laser speckle contrast analysis (LASCA) offers a dynamic and non‐invasive method to evaluate peripheral blood perfusion. It provides high‐resolution, contact‐free imaging of skin microcirculation, with perfusion indices that correlate inversely with the severity of NVC abnormalities.94, 105 Currently, LASCA remains a research tool, and further studies are required to establish its clinical utility, reproducibility, and standardization across SSc cohorts.106 A more recent development in SSc vascular imaging is the DAVIX (Digital Artery Volume Index), an MRI‐based technique that quantifies digital artery volume as a marker of vascular fibrosis. Recent studies have shown that DAVIX can predict the future development of digital ulcers and correlates with pulmonary arterial hypertension risk and overall disease severity, positioning it as a promising new outcome measure for vascular involvement in SSc.107
Baseline screening for internal organ involvement
4.4
Skin involvement in SSc is traditionally assessed using the modified Rodnan skin score (mRSS) at 17 sites of the arms and trunk, but advanced imaging techniques like high‐frequency ultrasound and MRI are being investigated for more objective evaluation. High‐frequency skin ultrasound can detect early changes not visible on clinical exam and allows for quantifying dermal thickness, echogenicity and stiffness using elastography.108, 109, 110
While international guidelines support standardized protocols, skin ultrasound remains primarily a research tool pending further validation and standardization before widespread clinical use.93
High‐resolution computed tomography (HRCT) of the chest is recommended for the screening of ILD in all patients at the time of SSc diagnosis, regardless of symptoms. This is supported by the ACR and the American College of Chest Physicians, as well as by international consensus, due to the high prevalence and prognostic significance of subclinical ILD in early SSc detectable in 41%–50% of patients depending on the stratification of disease subset.111 Recent advancements in SSc imaging include the promising use of lung ultrasound (LUS) as a screening tool for ILD. Multiple studies demonstrate that LUS, by detecting B‐lines, can identify subclinical and established ILD with a high sensitivity and, crucially, a high negative predictive value (up to 100%), particularly in low‐risk ILD patients when compared to HRCT.112 This suggests that LUS may offer a practical, radiation‐free alternative to HRCT in excluding ILD, especially for initial screening or in settings where HRCT is impractical. However, major and further studies are needed to optimize the real specificity, standardize protocols and mainly to determine the best timing for LUS during disease monitoring.113
Pulmonary function tests (PFTs), including spirometry, lung volumes and DLCO, should also be performed at baseline and serially for monitoring, but PFTs alone are insufficient for initial screening because they may miss early or subclinical ILD.90
Transthoracic echocardiography is recommended at diagnosis to screen for pulmonary arterial hypertension (PAH) and cardiac involvement.114 Recently, however, cardiac MRI has gained increasing relevance in selected cases, offering a more detailed assessment of myocardial fibrosis, inflammation and function, particularly when echocardiographic findings are inconclusive or clinical suspicion of cardiac involvement persists.92
Barium swallow and oesophageal manometry are not recommended as routine screening tests in asymptomatic patients with early SSc; these studies should be reserved for patients who have symptoms of dysphagia, gastroesophageal reflux, or when there is clinical suspicion of gastrointestinal involvement, such as unexplained pulmonary symptoms and signs, including chronic cough, recurrent aspiration pneumonia, voice hoarseness or radiographic evidence of oesophageal dilation.95
Similarly, renal imaging (e.g. renal ultrasound) is not routinely recommended for screening in early SSc unless there are clinical or laboratory signs suggestive of scleroderma renal crisis or other renal pathology.96
Altogether, multimodal and multiorgan imaging in early SSc is necessary to promptly detect organ involvement, optimize risk stratification and guide early intervention.
Early Intervention in early systemic sclerosis
4.5
The rationale for early therapeutic intervention in SSc lies in the recognition that tissue fibrosis is preceded and perpetuated by early immune dysregulation and endothelial damage.66 While clinical data support early immunosuppressive treatment in patients with dcSSc or ILD, evidence of benefit in the very earliest stages, defined by Raynaud's phenomenon, SSc‐specific autoantibodies and abnormal NVC, remains limited and inconclusive.
Canadian registry data have shown an increased use of immunosuppressants, especially methotrexate and MMF since 2007, guided mainly by autoantibody profiles rather than skin severity.115
Supporting this approach, low‐level evidence from a single‐center retrospective study by Yomono et al. found that starting immunosuppressants within 18 months of SSc diagnosis reduced lung function decline, disease activity and improved event‐free survival116 (see more details in Table 4). Similarly, moderate‐level evidence from the prospective observational European Scleroderma Observational Study (ESOS) showed that methotrexate, MMF and cyclophosphamide improved skin thickness in early diffuse SSc, and untreated patients had worse survival117; however, the differences between treatment groups were not statistically significant, and the observational design is susceptible to confounding by indication.
Limited data in limited cutaneous SSc suggest early immunosuppression may reduce long‐term organ damage, but evidence on preventing lung disease is inconsistent. These findings underscore the need for controlled trials and tailored treatments, especially due to low biologic use and possible confounding factors.118
In this context, the ‘Hit Hard and Early’ trial, a small RCT, provided evidence against untargeted immunosuppression in the very earliest disease stages. This study explored whether prompt intervention in the earliest clinical phases of SSc, specifically in patients with puffy fingers and autoantibody positivity, could alter disease trajectory.119 However, very early initial high‐dose glucocorticoids alone did not improve capillary density, disease progression, or lung function at 1 year, discouraging their use in the absence of overt inflammatory organ involvement.
In addition to traditional immunosuppressants, antifibrotic therapies such as nintedanib have become valuable for treating SSc‐associated ILD, supported by high‐level evidence from a large RCT. Subgroup analyses from the SENSCIS trial showed that patients with early disease (<18 months from first non‐Raynaud symptom) experienced faster FVC decline (−167.8 mL/year vs. −93.3 mL/year in the overall population) and appeared to benefit more from nintedanib, highlighting the potential advantage of early antifibrotic intervention in rapidly progressive cases.120
As for vasodilators, calcium channel blockers, phosphodiesterase‐5 (PDE‐5) inhibitors, and endothelin receptor antagonists, they are effective for managing symptoms of Raynaud's phenomenon and digital ulcers, with bosentan reducing new ulcer formation.121 However, no data supports their role as disease‐modifying treatments in early or pre‐clinical SSc stages. A large French study found that only sildenafil may have cardioprotective effects in established SSc, improving diastolic function and ejection fraction, while bosentan, ACE inhibitors and iloprost showed no significant cardiac benefits.122
In summary, while early intervention in SSc is a compelling strategy, especially for patients at high risk of progression (i.e. male sex, anti‐Scl70 positivity and black ethnicity), the overall quality of evidence for broad immunosuppressive therapy remains low to moderate, largely derived from observational or retrospective studies that are prone to bias.123 The risk of overtreatment, including adverse effects from immunosuppressive or biologic agents, must be balanced against the uncertain benefit in preclinical disease stages.
Future research should prioritize longitudinal cohort studies and targeted randomized trials in early or at‐risk SSc populations, to better define when, who and how to treat and to move from symptom control to true disease modification.
EARLY DETECTION OF GIANT CELL ARTERITIS IN PATIENTS WITH POLYMYALGIA RHEUMATICA
5
Polymyalgia rheumatica (PMR) is quite a common inflammatory disease in elderly people with a peak of incidence at 70–75 years of age, causing pain and stiffness in the shoulders, neck and hips.124 It can occur alone or alongside giant cell arteritis (GCA), a vasculitis affecting large arteries, especially the temporal arteries and the aorta.8 These conditions are now seen as part of a shared spectrum (GCA‐PMR spectrum disease) due to overlapping mechanisms and treatment responses.8, 125
Clinical or imaging findings of GCA are detected in 16%–23% of patients initially diagnosed with PMR.126 However, the precise pathological meaning and optimal management for this subclinical vascular inflammation remain subjects of ongoing debate. Early recognition of large vessel vasculitis among PMR patients is crucial, given the potential for severe vascular complications such as vision loss, strokes and aortic aneurysms if left untreated.127
Clinical features
5.1
The clinical presentation of GCA in patients with PMR is heterogeneous. While some patients present with classic cranial symptoms such as new‐onset headache, jaw claudication or visual changes, many others have underlying subclinical GCA without these overt signs, posing a significant diagnostic challenge.127 In studies of GCA cohorts, PMR symptoms co‐occurred with cranial involvement in about 42% of patients (Table 3).135
However, these symptoms may be absent in many PMR patients who nonetheless harbor underlying subclinical GCA, posing significant diagnostic challenges.136 Indeed, a subset of patients initially presenting with isolated PMR shows subclinical large‐vessel GCA, involving extracranial arteries such as the aorta and its primary branches, including carotid, subclavian and axillary arteries.
The clinical features of extracranial involvement may be non‐specific, contributing to a diagnostic delay. These patients frequently experience systemic or constitutional symptoms, such as persistent fever of unknown origin, unexplained weight loss, night sweats, significant fatigue or malaise.126 Additionally, polymyalgic symptoms refractory to standard doses of glucocorticoids (typically 12.5–15 mg of prednisone equivalent daily sufficient in isolated PMR) may suggest underlying vascular involvement, warranting further investigation for GCA.129
Recent studies have also highlighted that the occurrence of limb claudication and pulse discrepancies between limbs can be early clinical markers of extracranial GCA, although these findings are often subtle and may go unnoticed without careful clinical examination.137 Furthermore, patients with subclinical large‐vessel GCA may present with isolated elevation of inflammatory markers without clear focal symptoms, which can lead to misinterpretation as isolated PMR.126, 136
Given these varied clinical presentations, recent guidelines recommend systematic assessment of potential GCA symptoms (cranial and extracranial) and routine physical examination (palpation of temporal arteries, assessment of peripheral pulses, blood pressure measurements in both arms) in all patients initially diagnosed with PMR, particularly those resistant to standard therapy or presenting with persistent systemic symptoms.127, 136, 137
Laboratory findings
5.2
Laboratory markers in GCA and PMR commonly include elevated acute phase reactants such as ESR and CRP, which, although useful for disease activity monitoring, have limited specificity for discriminating isolated PMR from associated GCA.128
A recent study has identified that a CRP cut‐off value of ⩾26.5 mg/L in PMR might help the identification of subclinical GCA, but these results warrant further validation in other cohorts.138 Specifically, an ESR >60 mm/h (positive LR 2.40, 95% CI 1.71–3.36) and CRP ≥2.5 mg/dL (negative LR 0.38, 95% CI 0.25–0.59) are informative, but neither marker alone is diagnostic, and both can be elevated in isolated PMR or other inflammatory conditions.134
Elevated platelet count (>400 × 10^3^/μL) is also associated with GCA and may aid in risk stratification. Recent biomarker studies have highlighted the potential of angiopoietin‐2 and matrix metalloproteinase‐3 (MMP‐3) as promising indicators of underlying GCA in PMR patients.131 These biomarkers, although preliminary, demonstrate higher specificity for vascular inflammation than traditional acute phase reactants and, despite being currently used in research settings, might be used in the future also in clinical practice.139
Imaging features of large vessel vasculitis in PMR patients
5.3
Imaging plays a central role in the early detection of subclinical GCA in patients with PMR. When large vessel vasculitis such as GCA is suspected in a patient, recent EULAR recommendations endorse Colour Doppler ultrasound (US) as the first‐line imaging modality. This is due to its high sensitivity and specificity for cranial GCA and its ability to detect the characteristic halo sign indicating vessel wall edema. The assessment of both temporal and axillary arteries is specifically recommended, as axillary involvement is common and contributes to diagnostic yield and disease monitoring. This reflects a conceptual shift toward viewing GCA as a single disease spectrum with overlapping cranial and extracranial manifestations.10
Recent large prospective and multicentre studies have shown that up to 23%–29% of patients with newly diagnosed PMR and no cranial symptoms display vascular abnormalities on imaging, particularly involving extracranial arteries such as the axillary, subclavian, and carotid branches.134 These abnormalities include non‐compressible arteries and increased intima‐media thickness or halo signs, more frequently detected in extracranial than cranial districts, indicating a predominant large‐vessel pattern of subclinical inflammation in this patient population.140
In patients presenting with overt GCA and visual symptoms, transorbital ultrasound has also emerged as a valuable adjunct. This technique can detect early biomarkers of ocular involvement, such as reduced blood flow in the central retinal artery, which helps identify patients at increased risk for vision loss.141
Positron emission tomography/computed tomography (PET/CT) offers whole‐body imaging and is particularly sensitive for detecting large‐vessel inflammation, especially in extracranial arteries such as the axillary, subclavian, and carotid arteries, which may be missed by US. However, cost, availability, and radiation exposure limit its use in routine screening.
Meta‐analyses and large prospective studies have shown that up to 23%–29% of newly diagnosed PMR patients without cranial symptoms have subclinical GCA detectable by imaging (Figure 1). Current evidence suggests that these patients may be at a higher risk of relapse and progression to overt GCA.134, 142 However, cost, availability and radiation exposure limit its routine use.
Several clinical and laboratory features have been proposed as predictive factors for the development of GCA in PMR patients. These include older age at onset, constitutional symptoms, hip or pelvic girdle pain (possibly reflecting limb claudication), lower back pain, night sweats, resistance to initial glucocorticoid treatment, and markedly elevated acute phase reactants.126 Due to the relatively frequent coexistence of subclinical GCA in PMR, routine imaging screening in PMR patients at high risk (persistent symptoms, elevated inflammatory markers despite therapy, older age at disease onset) is increasingly suggested.127
Early intervention and clinical outcomes of PMR patients with large vessel vasculitis
5.4
Timely initiation of glucocorticoid therapy remains the cornerstone in managing GCA, but the optimal treatment approach for subclinical large‐vessel vasculitis (LVV) in PMR remains uncertain. Current expert recommendations suggest starting glucocorticoids in PMR patients with clear imaging evidence of LVV, even in the absence of classic GCA symptoms, to reduce the risk of complications.137 However, no standardized therapeutic protocol exists for these cases, and randomized trials are lacking.
Moderate‐level evidence from a prospective, multicenter ultrasound study by De Miguel et al. that imaging‐detected LVV may identify a more aggressive disease phenotype, associated with higher relapse rates (62% vs. 16%, p < 0.001), greater glucocorticoid burden, and increased need for immunosuppressants like methotrexate.129 In particular, rapid tapering of glucocorticoids appears to increase relapse risk in this subgroup. However, these observational findings must be interpreted with caution, as clinicians were not blinded to the ultrasound results, which influenced treatment decisions. Nevertheless, the prognostic significance of subclinical vasculitis remains debated. While US‐based studies report increased relapse risk, others using FDG‐PET do not confirm this, likely due to methodological differences (see Table 4 for more details). At the moment, current evidence is heterogeneous and largely observational, with a high risk of bias from confounding by indication, warranting cautious interpretation and individualized management strategies.149 Notably, the absence of systematic vascular assessment in most PMR trials may have contributed to underestimating the true clinical impact of subclinical vasculitis in this setting.150
The emerging concept of the combined GPSD entity supports the idea that patients with PMR and vascular involvement represent a biologically distinct and more aggressive phenotype, rather than a simple coexistence of two entities.151, 152
Despite these important insights, optimal therapeutic approaches remain incompletely defined for patients with PMR‐associated subclinical large‐vessel involvement. While glucocorticoid dosing regimens for clinically overt GCA typically involve at least twice the dosage recommended for isolated PMR, observational data from the De Miguel cohort suggest that PMR patients with subclinical GCA often receive intermediate doses (e.g. 20–30 mg prednisone/day), but relapse despite these regimens, indicating that a ‘PMR‐style’ approach may be insufficient.129
Long‐term vascular outcomes such as aneurysms or stenosis are poorly characterized, and medium‐term studies have not demonstrated significant ischemic progression, though follow‐up data remain limited.153 Given these uncertainties, routine vascular imaging may be considered for selected high‐risk PMR patients, particularly those with persistent symptoms, poor response to therapy, or elevated inflammatory markers, while broader screening strategies will require the development of clinical stratification tools.
Ultimately, randomized controlled trials stratifying patients based on vascular imaging findings are needed to determine whether tailored treatment improves outcomes and to define evidence‐based management strategies for this increasingly recognized subset of PMR.
LIMITATIONS OF THE CURRENT EVIDENCE BASE
6
While this narrative review aims to provide a comprehensive and balanced synthesis of the current literature, several potential sources of bias should be acknowledged. Firstly, publication bias, favouring studies with positive or novel findings, remains an inherent limitation, particularly as evidence for early diagnosis and intervention in rheumatic diseases is often shaped by high‐profile trials or guidelines rather than negative or null results. In addition, the review integrates studies with differing designs, populations, and definitions of ‘early’ disease, resulting in substantial heterogeneity that may limit direct comparability between the considered conditions. The predominance of European and North American cohorts, variable classification criteria, and evolving technologies (e.g. imaging or biomarker assays) further contribute to this heterogeneity.
Most of the included studies were appraised qualitatively, and thus conclusions may reflect subjective interpretation of study robustness and clinical applicability. Moreover, evidence gaps remain in some areas, particularly for preclinical phases and early intervention in SSc and LVV/PMR, where randomized controlled trials are scarce and observational or expert opinion predominates. As such, recommendations and interpretations should be considered within the context of these methodological limitations, and there is a need for larger, diverse and prospective studies to strengthen the evidence base and reduce the risk of selection, reporting and publication biases in this field.
CONCLUSION
7
The landscape of early diagnosis and intervention in IARDs has evolved toward proactive identification strategies, though with markedly different levels of evidence across conditions. Our overview shows that while early detection capabilities have advanced significantly through integrated clinical, serological, and imaging approaches, the translation to effective interventions varies considerably.
Evidence for early intervention is most robust in RA, especially in ACPA positive patients, where abatacept has demonstrated significant benefits in preventing disease progression in seropositive individuals with subclinical inflammation. However, important challenges remain in identifying which at‐risk individuals will actually develop disease, raising concerns about potential overtreatment.
In SSc, while laboratory and imaging advances, in particular thanks to the progress in identifying the earliest microvascular damage (i.e. NVC) at the earliest step of the disease, therapeutic interventions, especially early immunosuppressive therapies in preclinical disease stages, remain largely not yet standardized and are under progressive investigation.
For PMR, the recognition of subclinical LVV as a distinct phenotype has important prognostic implications, yet optimal management strategies remain undefined due to conflicting evidence from different imaging modalities and study designs.
Moving forward, more nuanced approaches are required to balance early intervention benefits against risks of overtreatment. Priority areas include developing better predictive algorithms to identify patients most likely to progress, conducting adequately powered randomized trials in truly and well‐defined early disease stages and establishing cost‐effective screening strategies.
AUTHOR CONTRIBUTIONS
Elvis Hysa: Conceptualization; methodology; investigation; data curation; writing—original draft preparation; writing—review and editing; resources; visualization. Emanuele Gotelli: Conceptualization; investigation; writing—original draft preparation; writing—review and editing; visualization. Carmen Pizzorni: Investigation; data curation; writing—review and editing; visualization. Sabrina Paolino: Investigation; data curation; writing—review and editing. Alberto Sulli: Methodology; investigation; writing—review and editing; supervision. Vanessa Smith: Methodology; investigation; writing—review and editing; supervision. Rosanna Campitiello: Conceptualization; methodology; supervision; writing—review and editing; resources. Maurizio Cutolo: Conceptualization; methodology; investigation; project administration and draft finalization; supervision; writing—review and editing; resources; visualization; final approval.
FUNDING INFORMATION
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not‐for‐profit sectors.
CONFLICT OF INTEREST STATEMENT
The authors declare no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Choi MY , Costenbader KH . Understanding the concept of pre‐clinical autoimmunity: prediction and prevention of systemic lupus erythematosus: identifying risk factors and developing strategies against disease development. Front Immunol. 2022;13:890522.35720390 10.3389/fimmu.2022.890522 PMC 9203849 · doi ↗ · pubmed ↗
- 2Zabotti A , De Marco G , Gossec L , et al. EULAR points to consider for the definition of clinical and imaging features suspicious for progression from psoriasis to psoriatic arthritis. Ann Rheum Dis. 2023;82(9):1162‐1170.37295926 10.1136/ard-2023-224148 · doi ↗ · pubmed ↗
- 3Ogdie A . The preclinical phase of Ps A: a challenge for the epidemiologist. Ann Rheum Dis. 2017;76(9):1481‐1483.28274910 10.1136/annrheumdis-2017-211109 PMC 5554090 · doi ↗ · pubmed ↗
- 4Baethge C , Goldbeck‐Wood S , Mertens S . SANRA‐a scale for the quality assessment of narrative review articles. Res Integr Peer Rev. 2019;4:5.30962953 10.1186/s 41073-019-0064-8PMC 6434870 · doi ↗ · pubmed ↗
- 5Taylor PC . Update on the diagnosis and management of early rheumatoid arthritis. Clin Med (Lond). 2020;20(6):561‐564.33199320 10.7861/clinmed.2020-0727 PMC 7687323 · doi ↗ · pubmed ↗
- 6Aletaha D , Neogi T , Silman AJ , et al. Rheumatoid arthritis classification criteria: an American College of Rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. 2010;62:2569‐2581.20872595 10.1002/art.27584 · doi ↗ · pubmed ↗
- 7Le Roy EC , Medsger TA Jr . Criteria for the classification of early systemic sclerosis. J Rheumatol. 2001;28(7):1573‐1576.11469464 · pubmed ↗
- 8Tomelleri A , van der Geest KSM , Khurshid MA , et al. Disease stratification in GCA and PMR: state of the art and future perspectives. Nat Rev Rheumatol. 2023;19(7):446‐459.37308659 10.1038/s 41584-023-00976-8 · doi ↗ · pubmed ↗