Target trial emulation of statin discontinuation in multimorbid older adults with polypharmacy
Valerie Aponte Ribero, Oliver Baretella, Cinzia Del Giovane, Moa Haller, Martin Feller, Benoît Boland, Antoine Christiaens, Wilma Knol, Denis O'Mahony, Viktoria Gastens, Baris Gencer, Stéphanie Baggio, Nicolas Rodondi

TL;DR
Statin discontinuation in older adults with multiple health conditions and many medications is linked to higher non-cardiovascular mortality, but not clearly linked to heart issues.
Contribution
First target trial emulation in multimorbid older adults assessing statin discontinuation effects.
Findings
Statin discontinuation was associated with increased composite outcome risk (cardiovascular events or mortality).
Non-cardiovascular deaths were higher in those who discontinued statins.
Adjusting for geriatric syndromes did not change the results.
Abstract
The benefit of statins in multimorbid older adults is controversial. Prior observational studies evaluating statin discontinuation in older adults were retrospective cohorts, did not focus on multimorbidity, or lacked adjustment for geriatric syndromes. We aimed to assess the effect of statin discontinuation on cardiovascular and mortality outcomes using the target trial emulation framework. We conducted a prospective cohort study using data from the OPERAM trial in adults aged ≥70 years with ≥3 chronic conditions and ≥5 chronic drugs, comparing statin discontinuation to continuation. The primary composite outcome was cardiovascular events or all‐cause mortality at 12 months. We calculated adjusted hazard ratios (HR) using weighted pooled logistic regressions without (model‐A) and with adjustment for two geriatric syndromes (falls and weight loss; model‐B). Of 2668 person‐trial units…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
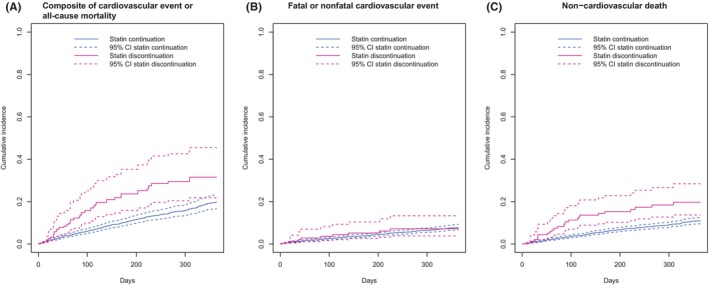 FIGURE 1
FIGURE 1| Characteristics | Overall | Statin continuation | Statin discontinuation |
|
|---|---|---|---|---|
| ( | ( | ( | ||
| Socio‐demographics | ||||
| Age (years) | 78.5 (5.9) | 78.5 (5.8) | 80.2 (6.9) | .001 |
| Women | 1025 (38.4%) | 977 (38.5%) | 48 (36.1%) | .635 |
| Study sites | ||||
| Bern | 1065 (39.9%) | 1005 (39.6%) | 60 (45.1%) | .035 |
| Cork | 539 (20.2%) | 519 (20.5%) | 20 (15.0%) | |
| Louvain | 415 (15.6%) | 386 (15.2%) | 29 (21.8%) | |
| Utrecht | 649 (24.3%) | 625 (24.7%) | 24 (18.0%) | |
| Trial randomization group | ||||
| OPERAM Control | 1403 (52.6%) | 1331 (52.5%) | 72 (54.1%) | .781 |
| OPERAM Intervention | 1265 (47.4%) | 1204 (47.5%) | 61 (45.9%) | |
| Medication | ||||
| Number of chronic medications | 10 (7–13) | 10 (7–13) | 10 (7–13) | .757 |
| Statin type | ||||
| Atorvastatin | 1261 (47.3%) | 1192 (47.0%) | 69 (51.9%) | .691 |
| Fluvastatin | 41 (1.5%) | 38 (1.5%) | 3 (2.3%) | |
| Pravastatin | 213 (8.0%) | 204 (8.0%) | 9 (6.8%) | |
| Rosuvastatin | 535 (20.1%) | 513 (20.2%) | 22 (16.5%) | |
| Simvastatin | 618 (23.2%) | 588 (23.2%) | 30 (22.6%) | |
| Statin intensity | ||||
| High | 826 (31.0%) | 791 (31.0%) | 40 (30.1%) | .896 |
| Low/moderate | 1842 (69.0%) | 1749 (69.0%) | 93 (69.9%) | |
| Glucose‐lowering drugs | 821 (30.8%) | 783 (30.9%) | 38 (28.6%) | .640 |
| At least one drug–drug interaction | 1557 (58.4%) | 1475 (58.2%) | 82 (61.7%) | .483 |
| Comorbidities | ||||
| Cardiovascular disease | 1934 (72.5%) | 1858 (73.3%) | 76 (57.1%) | <.001 |
| Heart failure | 624 (23.4%) | 589 (23.2%) | 35 (26.3%) | .476 |
| Chronic respiratory disease | 1180 (44.2%) | 1116 (44.0%) | 64 (48.1%) | .402 |
| Cancer (active malignancy except skin) | 717 (26.9%) | 678 (26.7%) | 39 (29.3%) | .580 |
| Health and frailty indicators | ||||
| Barthel index | 1054 (39.5%) | 985 (38.9%) | 69 (51.9%) | .004 |
| EQ‐5D VAS | 60.2 (20.5) | 60.3 (20.5) | 58.0 (20.6) | .203 |
| Number of falls in the previous year | ||||
| 0 | 1704 (63.9%) | 1626 (64.1%) | 78 (58.6%) | .623 |
| 1 | 475 (17.8%) | 449 (17.7%) | 26 (19.5%) | |
| 2 | 201 (7.5%) | 189 (7.5%) | 12 (9.0%) | |
| 3+ | 288 (10.8%) | 271 (10.7%) | 17 (12.8%) | |
| Lost weight in the previous year | 860 (32.2%) | 817 (32.2%) | 43 (32.3%) | 1.000 |
| Outcome | Statin discontinuation | Statin continuation | Hazard ratio (95% CI) | ||
|---|---|---|---|---|---|
| Crude | Crude | Crude | Model A | Model B | |
| Primary and secondary outcomes | |||||
| Death or cardiovascular event | 33 (24.8%) | 362 (14.3%) | 1.83 (1.28 to 2.62) | 1.53 (1.14 to 2.06) | 1.49 (1.12 to 1.99) |
| Fatal or nonfatal cardiovascular event | 8 (6.0%) | 155 (6.1%) | 1.04 (.51 to 2.11) | 1.36 (.86 to 2.14) | 1.35 (.86 to 2.12) |
| Nonfatal cardiovascular event | 8 (6.0%) | 135 (5.3%) | 1.19 (.58 to 2.43) | 1.39 (.85 to 2.26) | 1.38 (.85 to 2.25) |
| Fatal cardiovascular event | 0 (0%) | 27 (1.1%) | Not estimable | 1.00 (.30 to 3.28) | .99 (.30 to 3.26) |
| Non‐cardiovascular death | 26 (19.5%) | 223 (8.8%) | 2.33 (1.55 to 3.49) | 1.56 (1.08 to 2.27) | 1.52 (1.06 to 2.19) |
| Cancer death | 12 (9.0%) | 72 (2.8%) | 3.32 (1.80 to 6.13) | 1.91 (.95 to 3.82) | 1.71 (.89 to 3.29) |
| Fall‐related injury or fracture | 27 (20.3%) | 521 (20.6%) | 1.06 (.72 to 1.56) | 1.04 (.77 to 1.39) | 1.02 (.76 to 1.36) |
| Barthel index <90 | 39 (29.3%) | 742 (29.3%) | 1.29 | 1.13 | 1.10 |
| EQ‐5D VAS | 62.9 (17.4) | 67.0 (18.8) | −4.13 | −2.11 | −2.08 |
| Negative control outcome | |||||
| Gastrointestinal disorder | 3 (2.3%) | 88 (3.5%) | .68 (.22 to 2.15) | 1.17 (.64 to 2.13) | 1.17 (.63 to 2.14) |
| Sensitivity analysis: primary outcome including heart failure | |||||
| Death or cardiovascular event incl. heart failure | 41 (30.8%) | 467 (18.4%) | 1.80 (1.31 to 2.47) | 1.42 (1.10 to 1.83) | 1.39 (1.08 to 1.79) |
| Fatal or nonfatal cardiovascular event incl. heart failure | 22 (16.5%) | 322 (12.7%) | 1.40 (.91 to 2.15) | 1.29 (.95 to 1.75) | 1.30 (.95 to 1.77) |
- —University of Bern10.13039/100009068
- —Staatssekretariat für Bildung, Forschung und Innovation10.13039/501100007352
- —Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung10.13039/501100001711
- —Horizon 2020 Framework Programme10.13039/100010661
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLipoproteins and Cardiovascular Health · Health Systems, Economic Evaluations, Quality of Life · Pharmaceutical Economics and Policy
INTRODUCTION
1
Statin use is highly prevalent among older persons aged ≥70 years, with prevalence ranging from 15% to 70%.1 However, robust evidence from clinical trials on the benefits of statins for primary cardiovascular prevention in older adults with multimorbidity is lacking.2, 3 Benefits of statins are well established in secondary prevention but with limited data in multimorbid populations due to their underrepresentation in clinical trials.4 Moreover, older adults with multimorbidity and polypharmacy are at increased risk of statin side effects.2 Consequently, statin deprescribing may be considered in this population, according to guidelines of the American Heart Association.5 However, clear evidence from randomized controlled trials (RCT) on the effects of statin discontinuation in multimorbid older people is sparse. One small RCT in patients in palliative care reported improved quality of life with no increase in cardiovascular events after statin discontinuation.3 However, this was a highly selected patient cohort with poor short‐term survival prognosis. A pragmatic primary prevention RCT in older patients with multimorbidity is currently ongoing, but results will not be expected before 2026.6
Target trial emulation as a framework for observational data analyses has the potential to provide valid causal estimates using observational data when data from RCTs are unavailable.7 Three observational studies in older adults found an increased risk of cardiovascular events, and one found no difference in all‐cause mortality after statin discontinuation prescribed for primary and secondary prevention.8, 9, 10, 11 However, all were retrospective cohort studies, which may limit the accuracy of data collection; none specifically examined a multimorbid population, and some did not adjust for geriatric syndromes, which may be confounding factors as they are associated with adverse medication effects and poor outcomes.8, 9, 10, 12, 13 Furthermore, none of these studies used a clone‐censor‐weight approach to handle immortal‐time bias, which has been recommended as better than other approaches as it avoids selection bias and offers a clearer interpretation of the estimand.14
In this study, we employed the target trial emulation framework to estimate the effect of statin discontinuation versus continuation on clinical outcomes in a well‐characterized prospective cohort of multimorbid older adults with polypharmacy using data from a recent large‐scale multicenter clinical trial.15 The primary objective was to assess the impact of statin discontinuation on cardiovascular events and mortality outcomes using two models with and without adjustment for geriatric syndromes. Secondary objectives were to assess the effect of statin discontinuation on falls, activities of daily living functionality and quality of life.
METHODS
2
Data source
2.1
Data for this target trial emulation was obtained from the OPERAM clinical trial (Optimizing thERapy to prevent Avoidable hospital admissions in Multimorbid older adults).15 The trial enrolled 2008 hospitalized patients aged 70 years or older with multimorbidity (≥3 chronic conditions) and polypharmacy (≥5 drugs used for over 30 days prior to eligibility assessment) in four European countries (Belgium, Ireland, the Netherlands and Switzerland) and enrolled patients from December 2016 to October 2018. The trial objective was to assess the effect of a medication review intervention versus usual pharmaceutical care on the first drug‐related hospital admission within 12 months after hospital discharge.15 Detailed data on medication use were collected at enrolment and follow‐up visits post‐randomization. Ethics committees at each site approved the trial and written informed consent was obtained from each participant.
Participants
2.2
Participants aged ≥70 years with multimorbidity and polypharmacy who were taking statins at enrolment were eligible for inclusion in the current study. From a total of 1115 eligible patients under statins, 38 patients (3%) were excluded due to missing follow‐up data after discharge, 36 patients (3%) were excluded due to missing covariate data, and 13 patients (1%) were excluded as they had discontinued statins over 15 days prior to hospital discharge (Figure S1). Overall, 1028 statin‐treated patients were included in the current analysis.
Exposure
2.3
We compared statin discontinuation to statin continuation within three sequential emulated trials starting at hospital discharge, 2 months and 6 months follow‐up to maximize the number of participants (Figure S2). All enrolled patients were followed for 12 months post‐enrolment. Patients were assigned to the statin discontinuation or continuation group at each of these timepoints, based on medication data collected at discharge, 2‐month and 6‐month follow‐up from at least one of the following sources: patients (or proxies), general practitioners, medical charts and/or charts from the local pharmacy. Statins were identified using the Anatomical Therapeutic Chemical (ATC) code C10AA. Since the recorded date of statin discontinuation did not always align with the follow‐up dates, we adopted a grace period of 30 days16 around the date of each starting timepoint (discharge, 2 months and 6 months follow‐up) to assign participants to statin discontinuation or continuation (Figure S2), and used a ‘clone‐censor‐weight’ approach to avoid any resulting immortal‐time bias.14 Although the majority of statin discontinuations were captured using the 30‐day grace period, to account for any potential misclassification of participants discontinuing statins afterwards, we conducted a sensitivity analysis prolonging the grace period to 3 months. Furthermore, we conducted a per‐protocol analysis in which participants were censored when restarting statins in the discontinuation group, or when discontinuing statins in the continuation group.
Outcomes
2.4
The primary outcome was a composite of first occurrence of a cardiovascular event (a composite of hospitalization for acute coronary syndrome, stroke, transient ischemic attack, or peripheral vascular disease; these are atherosclerotic cardiovascular outcomes as defined by the American Heart Association17) or all‐cause death within 12 months. All‐cause death (and not cardiovascular death only) was selected in the composite to account for competing mortality among this multimorbid older population and a possible shift from cardiovascular to other causes of death (such patterns were seen in two statin RCTs).18 Cardiovascular events were identified via International Classification of Diseases, Tenth Revision (ICD‐10) diagnoses of hospital admissions (Table S1) and via serious adverse events reported as ‘acute coronary syndrome’ or ‘stroke’ which were reported for all patients as part of the OPERAM trial. Follow‐up of participants started at hospital discharge, 2 months or 6 months, respectively, and ended at the first occurrence of the outcome, death, loss to follow‐up, or end of follow‐up (12 months; Figure S2). We also evaluated the components of the composite outcome incorporating (i) first fatal or non‐fatal cardiovascular event and (ii) non‐cardiovascular death. Secondary outcomes included incident falls, health‐related quality of life (measured using the EQ‐5D visual analogue scale [VAS]) and functional independence (measured using Barthel index; dichotomized using a cutoff score of 90 [corresponding to none or slight vs. moderate to total dependence]19 due to severe skewness) at 12 months. Different cut‐offs for the Barthel index were explored in sensitivity analyses. As a negative control outcome, we assessed the impact of statin discontinuation on hospitalization for gastrointestinal disorders to assess the potential for residual confounding due to healthy‐user effects.
Statistical analysis
2.5
As this was a secondary analysis, no sample size was calculated a priori. We performed a sensitivity power analysis using G*Power 3.1 to determine the minimum effect size the study could detect. With alpha = .05, power = .80, n = 2533 in the no statin group, n = 133 in the statin group, and a two‐tailed independent t‐test, we could detect an effect size of d = .25. Therefore, our study was powered to detect medium effect sizes.
The specifications of the target trial emulation are available in Table S2. We presented unweighted crude baseline characteristics and effect estimates using the pre‐cloned dataset. Baseline characteristics are shown in person‐trial units, which reflect the number of unique trial entries rather than unique individuals. In target trial emulation, patients can contribute to multiple trials (e.g., a person on statins may be eligible for the statin continuation group at multiple time points) and are therefore counted separately for each trial entry.
We used a three‐step ‘clone‐censor‐weight’ approach for the emulation.14 First, all patients were cloned and assigned to each treatment group (statin discontinuation and statin continuation). Since each group comprised all included patients, the groups were balanced in terms of all (measured and unmeasured) baseline characteristics by definition. Second, each clone was censored once they deviated from their assigned treatment group. A clone assigned to the statin discontinuation group was censored at the end of the grace period, while a clone assigned to the statin continuation group was censored once they discontinued the statin during the grace period. Third, patients were weighted using time‐varying inverse probability of censoring weights (IPCW) to account for selection bias from censoring and loss to follow‐up. Our assumed confounding structure is presented in Figure S3. Two logistic regression models were fitted to calculate stabilized IPCW for each emulated trial separately: model A was fitted with treatment group (discontinuation vs. continuation) as the dependent variable and time from baseline (in days), OPERAM randomization group, study site, age, sex, statin intensity (low/moderate vs. high),17 use of glucose‐lowering drugs (ATC code A10), presence of comorbidities (cardiovascular disease, cancer, chronic respiratory disease, heart failure; Table S1) and Barthel index (≥90 vs. <90) as independent variables (Figure S2). Model B additionally included two geriatric syndromes, number of falls in the previous year (0, 1, 2 or 3+) and weight loss in the previous year (yes or no), as independent variables.
Outcomes were analysed with pooled data from all three emulated trials. For time‐to‐event outcomes, we estimated hazard ratios (HR) and 95% confidence intervals (CI) using IPCW‐weighted pooled logistic regression models, which approximate a time‐dependent Cox model when time intervals are short (1 day in our study).20 A post‐hoc decision was made to present weighted cumulative incidence curves and 12‐month event probabilities (Aalen‐Johansen estimates) for the primary outcome, following recommendations to report absolute risks in addition to hazard ratios.21 We estimated odds ratios (OR) for binary outcomes using weighted logistic regressions and mean differences for continuous outcomes using weighted linear regressions. Robust standard errors were calculated to account for the fact that patients may be included multiple times across the three emulated trials.
We performed stratified analyses by primary and secondary cardiovascular prevention and computed interaction p‐values by adding an interaction term between treatment group and history of cardiovascular disease to model B. We conducted several sensitivity analyses: running the analyses without a grace period and lengthening it to 3 months; including new cancer diagnoses as a time‐varying confounder; including hospitalizations for heart failure in the cardiovascular event definition; using other commonly used cut‐offs of the Barthel index (≤60 for severe dependence, ≤20 for total dependence); and excluding participants with cancer at baseline.19 We also conducted a ‘per‐protocol’ analysis in which patients were censored upon deviation from their assigned treatment group (i.e., restarting statins in the discontinuation group and discontinuing statins in the continuation group). For continuous and binary outcomes, those patients were excluded from the ‘per‐protocol’ analyses. Finally, we calculated the E‐value for confounding to assess the magnitude of confounding necessary to explain away the results.22 Analyses were conducted using R statistical software, version 4.3.2.
RESULTS
3
Cohort characteristics
3.1
We included data from a total of 1028 unique patients contributing to 2668 person‐trial units across the three emulated trials (Table 1). The mean age was 78.5 years (standard deviation [SD] 5.9) and 38% were women. A total of 73% of patients had established cardiovascular disease and 31% used high‐intensity statins at baseline. Statins were discontinued within 1 month by 133 (5%) patients while 2535 (95%) patients continued statins. Of those who discontinued statin therapy, 57 patients (43%) did not have prior cardiovascular disease and 76 patients (57%) had established cardiovascular disease. The reason for discontinuation was undocumented in most cases (62%). When a reason was stated, ‘no current indication’ was the most common reason given (22% of cases). Patients in the statin discontinuation group were older (80.2 years vs. 78.5 years), fewer had cardiovascular disease (57.1% vs. 73.3%) and were less functionally independent (Barthel index <90; 51.9% vs. 38.9%) than patients in the continuation group. Patients in Bern (Switzerland) and Louvain (Belgium) were more likely to discontinue statins than patients in Cork (Ireland) and Utrecht (the Netherlands). Other characteristics were similar between groups. Over a median follow‐up of 9.9 months (interquartile range: 6.1–11.7), 395 (14.9%) patients experienced the primary outcome. A total of 163 patients (6.1%) had a fatal or nonfatal cardiovascular event and 249 (9.3%) patients died due to non‐cardiovascular causes. The most common cause of non‐cardiovascular death was disseminated cancer (30% of deaths; Table S3).
Impact of statin discontinuation on clinical outcomes
3.2
Results are shown in Table 2. The crude number of patients who died or had a cardiovascular event at 12 months was 33 (24.8%) in the discontinuation group and 362 (14.3%) in the continuation group, with a crude HR of 1.83 (95% CI 1.28–2.62). After cloning and weighting, the 12‐month event probability was 27% (95% CI 18%–35%) for statin discontinuation and 18% (95% CI 15%–21%) for statin continuation (Figure 1). The rate of the primary outcome remained higher for statin discontinuation versus continuation (HR 1.53, 95% CI 1.14–2.06). Additional adjustment for the number of falls and weight loss in the previous year resulted in a similar HR (1.49, 95% CI 1.12–1.99). These results were mainly driven by an increased risk of non‐cardiovascular death, with a weighted event probability at 12 months of 20% (95% CI 14%–28%) and 11% (95% CI 10%–12%) for the statin discontinuation and continuation groups, respectively (Figure 1, HR model‐A 1.56, 95% CI 1.08–2.27; model‐B 1.52, 95% CI 1.06–2.19). There was no evidence for a difference in the rate of fatal or nonfatal cardiovascular events; the weighted 12‐month event probability was 7% (95% CI 4%–13%) for statin discontinuation and 8% (95% CI 7%–9%) for continuation (Figure 1, HR model‐A 1.36, 95% CI .86–2.14; model‐B 1.35, 95% CI .86–2.12). Results from the ‘per‐protocol’ analysis were similar to the main analysis (Table S5). Conclusions were also unchanged in sensitivity analyses (Tables S6–S10). The E‐value for unmeasured confounding was 1.96 for the primary composite outcome; hence, confounders would have to be associated with a 2‐fold increase of the outcome and prevalence in statin discontinuation to account for the result.
Weighted cumulative incidence curves of death and cardiovascular event outcomes. Weighted cumulative incidence curves were estimated using stabilized inverse probability weights controlling for randomization group, study site, age, sex, glucose‐lowering drugs, statin intensity, Barthel index, comorbidities (cardiovascular disease, cancer [except skin], chronic respiratory disease, heart failure), number of falls and weight lost in the previous year.
Results of secondary outcomes did not show evidence for an association between statin discontinuation and fall‐related injuries or fractures, the Barthel Index score, or the EQ‐5D VAS score (Table 2). Similarly, there was no evidence for an association between statin discontinuation and incident gastrointestinal disorders (Table 2).
Subgroup analyses
3.3
Subgroup analyses by statin deprescribing for primary and secondary cardiovascular prevention did not provide evidence for a difference in the primary composite outcome or in the cardiovascular events outcome (Table S4). Interestingly, the association between statin discontinuation and non‐cardiovascular death was significantly weaker for secondary cardiovascular prevention (HR 1.23, 95% CI .80–1.91) compared to primary prevention (HR 2.10, 95% CI 1.06–4.17; p‐value for interaction = .036). There was also evidence for a difference on the EQ‐5D VAS (p‐value for interaction = .044) and weak evidence for a difference in the Barthel Index score (p‐value for interaction = .069), with statin discontinuation being associated with lower EQ‐5D VAS and higher odds of Barthel index <90 versus continuation in primary prevention but not in secondary prevention.
DISCUSSION
4
In this target trial emulation of statin discontinuation prescribed in multimorbid older patients for primary and secondary cardiovascular prevention, statin discontinuation was associated with a higher risk of the composite outcome of cardiovascular events or all‐cause mortality over 12 months. This excess was mainly due to an increased risk of non‐cardiovascular deaths. In contrast with previous observational studies, there was no clear evidence for an association of statin discontinuation with cardiovascular events in this multimorbid older population. There was also no association with secondary outcomes of incident falls, functional independence status, or health‐related quality of life. These results were not modified by adjusting for the common geriatric syndromes of falls and weight loss.
To our knowledge, this is the first target trial emulation to assess statin discontinuation in an exclusively multimorbid older population.13 One small RCT of patients in palliative care did not find a significant difference in cardiovascular events between statin discontinuation and continuation, and quality of life improved marginally in the discontinuation group.3 However, the short‐term survival of most patients in the palliative care setting may account for the lack of any survival difference. Our study did not provide clear evidence for an association between statin discontinuation and cardiovascular events (HR 1.35, 95% CI .86–2.12). Although the point estimate was consistent with previous observational studies in older adults (HR range: 1.14–1.32),8, 9, 10 unlike previous studies we found similar absolute cardiovascular risk at 12 months between statin discontinuation (7%) and statin continuation (8%). However, confidence intervals were wide due to the low event rate. Unlike previous studies, we used a ‘clone‐censor‐weighting’ approach to address immortal‐time bias which avoids limitations of the landmark and time‐varying exposure models and upholds target trial emulation principles.14 Results from our study are not directly comparable to studies of older patients initiating statins due to different patient populations (statin‐naïve versus statin users) and potential legacy effects of statins.23
In the present cohort of multimorbid older adults with polypharmacy, statin discontinuation over 12 months' follow‐up was uncommon (5% of patients). A reason for the low discontinuation rate may be the high prevalence of established cardiovascular disease in this population (>70%, Table 1), as general practitioners may be less inclined to discontinue statins for secondary prevention even in the presence of side effects and frailty.24 Other potential reasons relating to deprescribing choices among both healthcare professionals and patients may include lack of evidence and guidelines on deprescribing statins, fear of health deterioration and patient preferences.24 Indeed, benefits of statins may extend cardiovascular risk reduction, reducing mortality even in lean older individuals with liver fibrosis.25 Whether such effects persist with multimorbidity and polypharmacy remains unclear. Notably, drug–drug interactions are common in polypharmacy (58% of participants had an interaction in the present study),26 including interactions with statins,27 and multiple severe interactions may increase mortality.28
While the target trial emulation framework helps to reduce certain avoidable biases (e.g., prevalent user and immortal time biases), confounding bias remains a major concern.29 We observed a large increased risk of non‐cardiovascular death with statin discontinuation that is both clinically and pathophysiologically implausible,30 indicating probable confounding bias. Controlling for reduced functional independence (Barthel Index score), frequency of past falls and weight loss as common geriatric syndromes in our analyses did not eliminate this association. Poor overall health and frailty have been suggested as common confounders.8 Perceived short life expectancy may confound results as it was associated with primary care physicians' advice to stop statins in older patients (OR of 50.7),24 exceeding the E‐value of 2 needed to explain results.22 However, a sensitivity analysis excluding patients with cancer at baseline did not change results. Since similar issues with confounding influences have been observed previously,8, 29 future studies should carefully consider potential biases, particularly by examining non‐cardiovascular mortality. Results from ongoing RCTs are needed to firmly establish the benefit–risk of statin discontinuation.6
Strengths and Limitations
4.1
Strengths of this study were (i) the high‐quality data on a well‐characterized cohort of multimorbid older adults from four European countries participating in the OPERAM trial, and (ii) the rigorous application of target trial emulation principles, including the use of the ‘clone‐censor‐weight’ method which has not been applied in previous studies on statin discontinuation. Importantly, this study is the first to assess statin discontinuation specifically in a multimorbid population.
Our study also has limitations. Residual confounding remained despite controlling for geriatric syndromes. One possible confounder might be perceived short life expectancy, which we could not sufficiently adjust for due to a lack of adequate variables. The reason for statin discontinuation could have provided useful information on confounding by indication, but it was only available for 38% of patients. Additionally, frailty was not explicitly assessed in the OPERAM study. Moreover, the OPERAM study was limited to a one‐year follow‐up and relatively few statin discontinuations (n = 133). While effects on cardiovascular events may appear at longer follow‐up, we observed no divergence of cumulative incidence curves between groups. Further, medication use data were based on various sources, including patient report, which may have introduced exposure misclassification due to imprecise reporting of medication start and end dates or non‐adherence. However, adherence was notably high in the OPERAM study.15 As participants accepted to be part of a clinical trial, they may differ from routine practice, but it allows for systematic data collection. We acknowledge that the OPERAM trial was not designed to adjudicate deaths resulting from drug–drug interactions, including those of statins.15
CONCLUSION
5
In this first target trial emulation of multimorbid older adults with polypharmacy enrolled during hospitalization, statin discontinuation was associated with a higher risk of the composite outcome of cardiovascular events or all‐cause mortality. However, non‐cardiovascular mortality was the main driver of the increased risk, suggesting residual confounding by indication. These increased risks were not modified by adjusting for common geriatric syndromes. In contrast to some previous retrospective cohort studies, there was no clear evidence of increased cardiovascular events arising from statin discontinuation. Our study highlights that only RCTs can clarify the safety of statin discontinuation in multimorbid older adults.
AUTHOR CONTRIBUTIONS
Concept and design: Rodondi, Del Giovane, Baggio, Baretella, Aponte Ribero. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: Aponte Ribero. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: Aponte Ribero, Baggio. Obtained funding: Rodondi, Baretella. Supervision: Rodondi, Baggio.
FUNDING INFORMATION
This work is part of the project ‘OPERAM: OPtimising thERapy to prevent Avoidable hospital admissions in Multimorbid Older Patients’ supported by the European Union's Horizon 2020 research and innovation program under the grant agreement No 634238, and by the Swiss State Secretariat for Education, Research and Innovation (SERI) under contract number 15.0137 and of the project ‘Discontinuing Statins in Multimorbid Older Adults without Cardiovascular Disease (STREAM)’ supported by the Swiss National Science Foundation (SNSF) under the grant agreement No IICT 33IC30‐193052 (to Prof. Rodondi). The opinions expressed and arguments employed herein are those of the authors and do not necessarily reflect the official views of the European Commission and the Swiss government. VAR was supported by the Swiss National Scientific Foundation (grant number 325130_204361/1). OB obtained a Protected Research Time (PRT) Grant from the University of Bern for this project.
CONFLICT OF INTEREST STATEMENT
None.
Supporting information
Appendix S1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thompson W , Pottegård A , Nielsen JB , Haastrup P , Jarbøl DE . How common is statin use in the oldest old? Drugs Aging. 2018;35(8):679‐686. doi:10.1007/s 40266-018-0567-x 29987758 · doi ↗ · pubmed ↗
- 2Noaman S , Ibrahim JE , Grenfell R . Prescribing statins for cardiovascular disease prevention in the old: an absence of evidence and an absence of guidelines. Heart Lung Circ. 2014;23(7):619‐624. doi:10.1016/j.hlc.2014.03.002 24704467 · doi ↗ · pubmed ↗
- 3Kutner JS , Blatchford PJ , Taylor DH Jr , et al. Safety and benefit of discontinuing statin therapy in the setting of advanced, life‐limiting illness: a randomized clinical trial. JAMA Intern Med. 2015;175(5):691‐700. doi:10.1001/jamainternmed.2015.0289 25798575 PMC 4618294 · doi ↗ · pubmed ↗
- 4Aeschbacher‐Germann M , Kaiser N , Speierer A , et al. Lipid‐lowering trials are not representative of patients managed in clinical practice: a systematic review and meta‐analysis of exclusion criteria. J Am Heart Assoc. 2023;12(1):e 026551. doi:10.1161/jaha.122.026551 36565207 PMC 9973576 · doi ↗ · pubmed ↗
- 5Grundy SM , Stone NJ , Bailey AL , et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/A Ph A/ASPC/NLA/PCNA guideline on the Management of Blood Cholesterol: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73(24):e 285‐e 350. doi:10.1016/j.jacc.2018.11.003 30423393 · doi ↗ · pubmed ↗
- 6Discontinuing Statins in Multimorbid Older Adults Without Cardiovascular Disease (STREAM)—a Randomized Non‐inferiority Clinical Trial. Clinical Trials.Gov Identifier: NCT 05178420. Recruiting, Insel Gruppe AG, University Hospital Bern. Accessed 27.01.2025. https://clinicaltrials.gov/study/NCT 05178420
- 7Wang SV , Schneeweiss S , Initiative R‐D , et al. Emulation of randomized clinical trials with nonrandomized database analyses: results of 32 clinical trials. JAMA. 2023;329(16):1376‐1385. doi:10.1001/jama.2023.4221 37097356 PMC 10130954 · doi ↗ · pubmed ↗
- 8Thompson W , Morin L , Jarbøl DE , et al. Statin discontinuation and cardiovascular events among older people in Denmark. JAMA Netw Open. 2021;4(12):e 2136802. doi:10.1001/jamanetworkopen.2021.36802 34854906 PMC 8640890 · doi ↗ · pubmed ↗