A retrospective cohort study of supervised and home baked and/or neat hen's egg challenge for pediatric IgE hen's egg allergy
Caitlin Pollock, Benjamin James Talks, Julie Pentland, Emily Walton, Carina Venter, Louise J. Michaelis

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
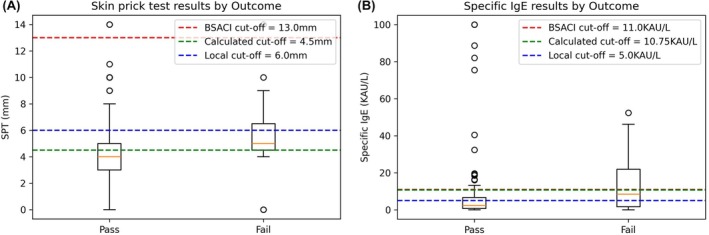 FIGURE 1
FIGURE 1| Outcome of introduction | Pass | Fail |
| ||||||
|---|---|---|---|---|---|---|---|---|---|
| Location of introduction | Supervised | Home | Supervised | Home | |||||
|
| median ± IQR/ |
| median ± IQR/ |
| median ± IQR/ |
| median ± IQR/ | ||
| Demographics | |||||||||
| Age at introduction, months | 107 | 46.0 ± 55.5 | 49 | 32.0 ± 31.8 | 19 | 63.0 ± 82.5 | 6 | 25.2 ± 8.6 | .31 |
| Sex, female | 107 | 39 (34.6) | 49 | 22 (44.9) | 19 | 8 (42.1) | 6 | 3 (50.0) | .71 |
| Ethnicity | 107 | 49 | 19 | 6 | .19 | ||||
| White | 77 (72.0) | 35 (71.4) | 12 (63.2) | 6 (100.0) | |||||
| White—Other | 3 (2.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||||
| Mixed—White/Black Caribbean | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||||
| Mixed—White/Asian | 3 (2.8) | 2 (4.1) | 0 (0.0) | 0 (0.0) | |||||
| Asian and British Asian—Indian | 0 (0.0) | 1 (2.0) | 1 (5.3) | 0 (0.0) | |||||
| Asian and British Asian—Pakistani | 5 (4.7) | 3 (6.1) | 0 (0.0) | 0 (0.0) | |||||
| Asian and British Asian—Bangladeshi | 3 (2.8) | 0 (0.0) | 2 (10.5) | 0 (0.0) | |||||
| Chinese | 0 (0.0) | 0 (0.0) | 1 (5.3) | 0 (0.0) | |||||
| Black and Black British—African | 0 (0.0) | 1 (2.0) | 1 (5.3) | 0 (0.0) | |||||
| Mixed—Other | 0 (0.0) | 1 (2.0) | 0 (0.0) | 0 (0.0) | |||||
| Other | 14 (13.1) | 6 (12.2) | 2 (10.5) | 0 (0.0) | |||||
| Past medical history | |||||||||
| Atopic dermatitis | 107 | 89 (83.2) | 49 | 41 (83.7) | 19 | 16 (84.2) | 6 | 6 (100.0) | .77 |
| Allergic rhinitis | 107 | 32 (29.9) | 49 | 5 (10.2) | 19 | 12 (63.2) | 6 | 1 (16.7) | . |
| Atopic asthma | 107 | 13 (12.2) | 49 | 3 (6.1) | 19 | 6 (31.6) | 6 | 1 (16.7) | .03 |
| Uncontrolled atopy | 91 | 12 (13.1) | 45 | 2 (4.4) | 17 | 3 (17.7) | 6 | 0 (0.0) | .98 |
| Additional food allergy | 107 | 49 | 19 | 6 | .05 | ||||
| One additional | 33 (30.1) | 10 (20.4) | 7 (36.8) | 2 (33.3) | |||||
| More than one | 31 (29.0) | 11 (22.4) | 8 (42.1) | 3 (50.0) | |||||
| Previous anaphylaxis to egg protein | 76 | 7 (9.2) | 37 | 1 (2.7) | 16 | 0 (0.0) | 6 | 0 (0.0) | .36 |
| Dietician input | 107 | 50 (46.7) | 49 | 24 (49.0) | 19 | 13 (68.4) | 6 | 5 (83.3) | .04 |
| Index reaction | |||||||||
| Type of egg | 103 | 48 | 17 | 6 | .92 | ||||
| Baked | 12 (11.7) | 3 (6.3) | 2 (11.8) | 0 (0.0) | |||||
| Neat | 91 (88.3) | 42 (87.5) | 15 (88.2) | 6 (100.0) | |||||
| Symptoms | 107 | 49 | 19 | 6 | .21 | ||||
| Respiratory symptoms | 16 (15.0) | 5 (10.9) | 5 (26.3) | 0 (0.0) | |||||
| Skin symptoms only | 67 (63.2) | 36 (73.5) | 9 (47.4) | 5 (83.3) | |||||
| Plus atopic dermatitis flare | 10 (9.4) | 6 (12.2) | 0 (0.0) | 0 (0.0) | |||||
| Plus gastrointestinal symptoms | 31 (29.0) | 9 (18.4) | 7 (36.8) | 1 (16.7) | |||||
| Investigations | |||||||||
| Skin prick test (mm) | 97 | 4.0 ± 3.0 | 42 | 2.5 ± 5.0 | 19 | 6.0 ± 2.5 | 4 | 4.5 ± 2.0 | . |
| Specific IgE—egg (KAU/L) | 80 | 2.7 ± 6.5 | 26 | 1.4 ± 5.25 | 17 | 13.3 ± 25.5 | 3 | 0.8 ± 2.1 | . |
| Total IgE (KAU/L) | 21 | 281 ± 2071 | 7 | 101.0 ± 574.9 | 6 | 461.5 ± 961.3 | 0 | – | .74 |
| CRD—Ovomucoid (ISU‐E) | 61 | 0.7 ± 2.6 | 20 | 0.0 ± 1.2 | 15 | 2.0 ± 7.6 | 3 | 0.0 ± 0.0 | .37 |
| CRD—Ovalbumin (ISU‐E) | 13 | 1.8 ± 3.3 | 5 | 1.1 ± 1.2 | 4 | 21.3 ± 10.1 | 0 | – | .06 |
| Reintroduction | |||||||||
| Type of egg | 107 | 49 | 19 | 6 | .23 | ||||
| Baked | 42 (39.2) | 28 (57.1) | 12 (63.2) | 3 (50.0) | |||||
| Neat | 65 (60.8) | 21 (42.9) | 7 (36.8) | 3 (50.0) | |||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFood Allergy and Anaphylaxis Research · Eosinophilic Esophagitis · Asthma and respiratory diseases
To the Editor(s),
IgE‐mediated food allergy and anaphylaxis are a growing burden on healthcare providers. Consequent highly restrictive diets are associated with faltering growth, further sensitization and allergy, and poor quality of life.1 In‐hospital oral food challenge is the gold standard for reintroducing allergenic foods, referred to as “supervised introduction” (SI). Home introduction (HI) is an alternative strategy that has been recommended for IgE‐mediated hen's egg allergy in the British Society of Allergy and Clinical Immunology (BSACI) 2021 guideline.2 A HI challenge involves graded reintroduction of hen's egg protein into the diet under parental supervision over days to weeks via a “food ladder” with increasing allergenicity at each “stage”.2 HI has the potential to improve patients' healthcare experience as food is reintroduced in a familiar environment whilst reducing the burden on healthcare providers. There have been limited studies on the efficacy of HI or patient factors associated with HI success, representing an area in need of further research.2, 3
To consider this unmet need, we carried out a single‐center retrospective cohort study to review outcomes from a total of 205 oral hen's egg challenges (baked and neat) performed by 197 children with IgE mediated hen's egg allergy over a 12‐month period (2021). This diagnosis is confirmed by a clinical history of an IgE‐mediated reaction to hen's egg together with supporting skin prick test (SPT), specific IgE results (SpIgE) or Component Resolved Diagnostics (CRD) results. The primary outcome was challenge outcome for HI versus SI. Secondary outcomes included subsequent dietary inclusion, adverse reactions to challenge and risk factors related to challenge failure (regardless of setting or egg type). When children had undergone multiple challenges within the same year, only their first challenge result was included in subsequent analysis (131 HI and 66 SI). For risk factor analysis, a total of 181 challenges (excluding those with inconclusive or unknown outcomes) were compared, 127 SI and 55 HI.
HI was first adopted in our department with the switch to remote consultations during the COVID‐19 pandemic with limited SI availability. Additionally, parents declined face‐to‐face appointments, opting to undertake a challenge at home as preference. These children were provided with a food ladder (either baked or neat hen's egg) to follow. We took the opportunity to review these patients, comparing with the SI cohort along with risk factor analysis to inform future guidance and protocols for HI.
Children were allocated SI following multi‐disciplinary team discussion. These children attended the day‐case ward for a nurse‐supervised challenge following National and European protocols.4, 5 As such, neat hen's egg challenges were only offered to children who tolerated baked hen's egg 3–4 times a week, as per guidance.4, 5
HI (81.7% (49/60)) was successfully implemented with a comparable pass rate (no reaction), as SI (81.7% (107/131)) with 6 children having an unknown result from HI. Children undergoing SI were typically older at challenge (39.0 ± 57.0 months for SI, 27.5 ± 39.0 months for HI), potentially due to more severe or complex allergic disease, and long SI waiting lists. The BSACI recommends children be older than 12 months for HI. In this study, 19 children, aged less than 12 months, underwent HI with only 1 (5.0%) failure.2 The safety of HI in this age group is further supported by a large retrospective study of 675 children, in which severe challenge reactions were rarest in children younger than 12 months.6 Indeed, the “Enquiring About Tolerance Study” further advocates the need for early introduction of well‐cooked hen's egg (before 6 months of age), supported by a recent retrospective study recommending low dose challenges in children <12 months.7, 8
Importantly, HI proved safe, with only 6/66 (9.1%) children suffering an adverse reaction: 4/6 (66.7%) had skin reactions, and 2/6 (33.3%) had skin and gastrointestinal reactions. Most of these children (5/6, 83.3%) were given antihistamines, no child required hospital admission nor experienced anaphylaxis.
All children who underwent HI reintroduced hen's egg into their diet compared to only 41/49 (83.7%) children who passed SI during the study period with unknown inclusion for 52/107 of SI cohort This may reflect increased parental confidence, having already reintroduced the allergen in their home environment. Subsequent follow‐up, reviewed in 2023/24, highlighted that only 30/107 (28.0%) of SI did not reintroduce hen's egg into the diet. The reasons given for noninclusion aged >11 was persistent patient stress/anxiety and eczema flare (but no IgE symptoms), whilst those <5 years of age was a result of parental anxiety and child food refusal linked to taste/texture.
It is an ongoing clinical dilemma to predict high‐risk children for failing a food challenge. We compared passed (n = 156; 86.2%) and failed (n = 25; 13.8%) hen's egg challenge of any type (HI or SI) to look for variables that were predictive of challenge outcome (Table 1). The BSACI guideline defines high‐risk children as those with uncontrolled atopic asthma, severe multisystem allergy, or severe allergic reaction symptoms.2
In this study, co‐existing allergic rhinitis and atopic asthma were associated with challenge failure, in keeping with their position as endpoints of the “atopic march”.9 Of those children with asthma, 8/26 (30.8%) had poor control with 2/8 (20%) failing challenge, highlighting the importance of asthma control before challenge. Additionally, a higher rate of allergic rhinitis was seen in children who failed, 13/25 (52.0%) versus only 37/156 (23.7%) who passed. Therefore, we recommend avoiding HI in children with allergic rhinitis and atopic asthma. Interestingly, rates of atopic dermatitis were comparable in pass and fail cohorts with an incidence of 86.1% (130/156) and 88.0% (22/25), respectively.
Previous severe reactions to hen's egg were documented for 29/181 (16.0%) children: 18/23 (78.3%) passed SI and 6/6 (100.0%) passed HI. This demonstrates the potential for HI for children with no recent severe reactions within 6 months.
Of the baseline laboratory investigations performed, only SPT (whole hen's egg) and SpIgE (whole hen's egg) differed significantly between children who had passed and failedtheir challenge. Local calculated cutoff values for SPT and SpIgE (using area under the curve receiver‐operating‐characteristic analysis to maximize sensitivity and specificity) were SPT 4.5 mm and SpIgE 10.75 KAU/L, see Figure 1. This is markedly lower than the BSACI SPT recommendation of >13 mm, likely due to the use of different testing solutions, and highlighting the need for local SPT cutoffs depending on test solution used.2 Although routine testing of CRD is not recommended in the BSACI guideline, aa prospective study reports ovomucoid ISU‐E > 11.0 are associated with challenge failure.2, 10 In our study, of the 103 children who had CRD ovomucoid tested, 6 (5.8%) had a result >11.0 ISU‐E, all of whom underwent SI, and 3/6 (50.0%) failed.
Investigation results from the pass and fail cohorts with cutoffs demonstrated. (A) Skin prick test and (B) Specific IgE were significantly lower in children that passed this challenge, p = .01 for both.
In summary, HI is safe and feasible for challenge and subsequent introduction of hen's egg protein in low‐risk children with IgE‐mediated allergy. HI supports service provision, as HI has the potential to avoid prolonged waiting lists and prevent restrictive diets. However, patient selection is critical. We identified high‐risk children as those with previous severe reactions to hen's egg, uncontrolled atopic disease, older age group (>16 years), SPT >4.5 mm, or SpIgE >10.75 KAU/L. Clinical practice varies at the local and national level. Therefore, standardized HI protocols are needed to facilitate safe and effective HI, develop HI services, and improve comparability of cohorts.
AUTHOR CONTRIBUTIONS
Caitlin Pollock: Data curation; investigation; formal analysis; methodology; writing – original draft. Benjamin James Talks: Writing – review and editing; supervision. Julie Pentland: Data curation; supervision. Emily Walton: Data curation. Carina Venter: Writing – review and editing. Louise J. Michaelis: Conceptualization; supervision; resources; writing – review and editing.
CONFLICT OF INTEREST STATEMENT
None of the authors have a conflict of interest to disclose in relation to this work. Dr. Michaelis has previous national commercial clinical trials with associated Advisory Boards / Lectures with Danone, ALK and Regeneron. Dr. Michaelis is Vice President for Services for the British Society of Allergy and Immunology, United Kingdom. Dr. Venter reports grants from Mead Johnson Nutrition and personal fees from Mead Johnson Nutrition, Nestle Nutrition Institute, Danone, Abbott Nutrition, and Novalac outside the submitted work.
ETHICS STATEMENT
This retrospective cohort study was registered with the Clinical Effectiveness Register of Newcastle Upon Tyne Hospitals NHS Foundation Trust (project number: 13495). Since this was a retrospective study reviewing routine medical notes, individual patient consent was not obtained and would not be practicable to obtain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baseggio Conrado A , Ierodiakonou D , Gowland MH , Boyle RJ , Turner PJ . Food anaphylaxis in the United Kingdom: analysis of national data, 1998–2018. BMJ. 2021;372:n 251.33597169 10.1136/bmj.n 251PMC 7885259 · doi ↗ · pubmed ↗
- 2Leech SC , Ewan PW , Skypala IJ , et al. BSACI 2021 guideline for the management of egg allergy. Clin Exp Allergy. 2021;51(10):1262‐1278.34586690 10.1111/cea.14009 · doi ↗ · pubmed ↗
- 3Thomas L , Belcher J , Phillips R , Preece K , Bhatia R . Use of an egg ladder for home egg introduction in children with Ig E‐mediated egg allergy. Pediatr Allergy Immunol. 2021;32(7):1572‐1574.34008180 10.1111/pai.13541 · doi ↗ · pubmed ↗
- 4Sampson HA , Gerth Van Wijk R , Bindslev‐Jensen C , et al. Standardizing double‐blind, placebo‐controlled oral food challenges: American Academy of Allergy, Asthma & Immunology‐European academy of allergy and clinical immunology PRACTALL consensus report. J Allergy Clin Immunol. 2012;130(6):1260‐1274. doi:10.1016/j.jaci.2012.10.017 23195525 · doi ↗ · pubmed ↗
- 5Sampson HA , Arasi S , Bahnson HT , et al. AAAAI–EAACI PRACTALL: standardizing oral food challenges—2024 update. Pediatr Allergy Immunol. 2024;35(11):e 14276.39560049 10.1111/pai.14276 · doi ↗ · pubmed ↗
- 6Kennedy K , Alfaro MKC , Spergel ZC , Dorris SL , Spergel JM , Capucilli P . Differences in oral food challenge reaction severity based on increasing age in a pediatric population. Ann Allergy Asthma Immunol. 2021;127(5):562‐567.34010700 10.1016/j.anai.2021.05.013 · doi ↗ · pubmed ↗
- 7Takei M , Yanagida N , Sato S , Ebisawa M . Low‐dose oral food challenges. Pediatr Allergy Immunol. 2024;35(10):e 14258.39396116 10.1111/pai.14258 · doi ↗ · pubmed ↗
- 8Perkin MR , Logan K , Marrs T , et al. Enquiring about tolerance (EAT) study: feasibility of an early allergenic food introduction regimen. J Allergy Clin Immunol. 2016;137(5):1477‐1486.26896232 10.1016/j.jaci.2015.12.1322 PMC 4852987 · doi ↗ · pubmed ↗