Musculoskeletal Sarcoidosis With Sacroiliac Involvement: Report of a Rare Case
Mohamed Nassiri, Abdessamad Laaribi, Abdessalam Achkoun, Rachid Chafik

TL;DR
A rare case of sarcoidosis affecting the musculoskeletal system, including the sacroiliac joints, is reported with MRI findings and successful corticosteroid treatment.
Contribution
This paper presents a rare clinical case of musculoskeletal sarcoidosis with sacroiliac involvement and highlights the importance of histopathological confirmation.
Findings
MRI revealed bilateral sacroiliitis and pseudotumoral muscle lesions in a patient with musculoskeletal sarcoidosis.
Histopathological analysis confirmed non-caseating granulomas, leading to a sarcoidosis diagnosis.
Treatment with oral prednisone resulted in significant clinical improvement.
Abstract
Sarcoidosis is a systemic granulomatous disease of unknown etiology that rarely affects the musculoskeletal system. Sacroiliac involvement is exceptional and may mimic spondyloarthropathies or malignancy. We report the case of a 47-year-old man presenting with progressive bilateral sacroiliac and shoulder pain. MRI showed bilateral sacroiliitis with diffuse bone marrow lesions in the pelvic girdle and femoral heads, as well as a pseudotumoral lesion of the iliopsoas muscle. CT demonstrated a lytic lesion of the left humeral head with cortical rupture. Laboratory findings revealed elevated C-reactive protein, hypercalciuria, and increased serum angiotensin-converting enzyme (ACE) levels. Histopathological examination of bone and muscle biopsies demonstrated non-caseating granulomas. The diagnosis of musculoskeletal sarcoidosis was established. The patient was treated with oral prednisone…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
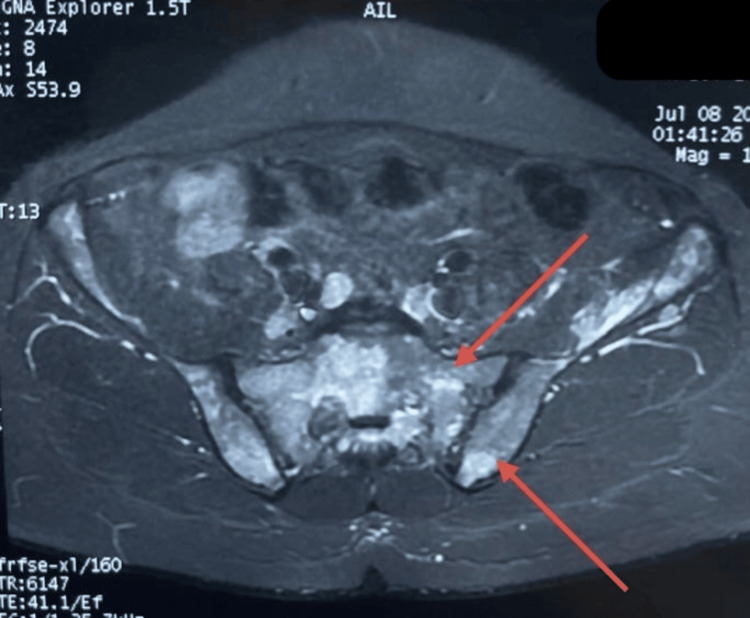 Figure 1
Figure 1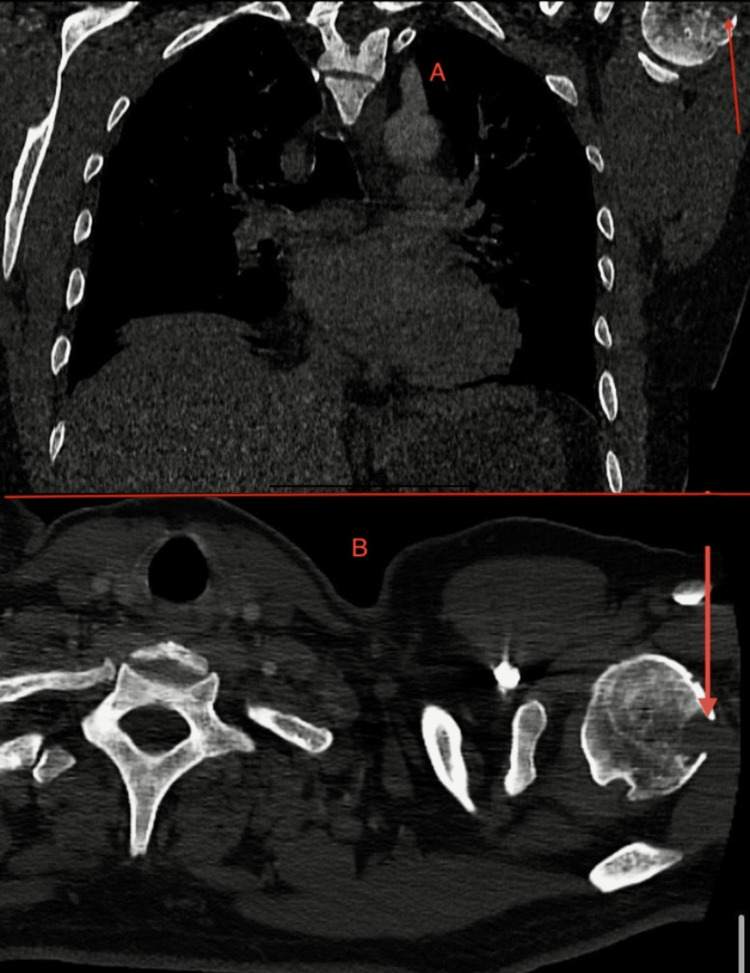 Figure 2
Figure 2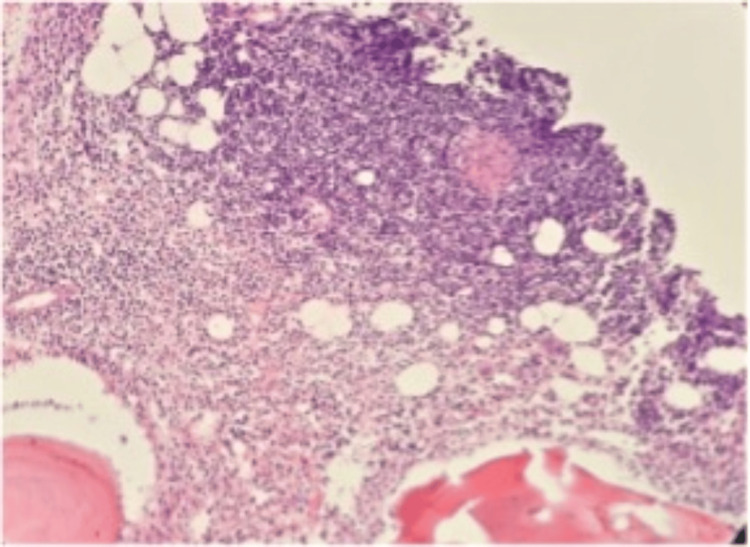 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Bone and Joint Diseases · Orthopedic Infections and Treatments
Introduction
Sarcoidosis is a multi-system granulomatous disorder of unknown etiology, most commonly affecting the lungs and lymph nodes, but virtually any organ system may be involved. The disease is characterized histologically by non-caseating granulomas and displays a wide spectrum of clinical presentations, ranging from asymptomatic forms to severe, multi-system disease [1].
Musculoskeletal involvement is reported in approximately 1-13% of patients and may manifest as acute or chronic arthritis, periarticular soft tissue inflammation, tenosynovitis, myopathy, or osseous lesions [1]. While acute arthritis is relatively well recognized, bone and muscle involvement remain uncommon and are often underdiagnosed due to their nonspecific clinical and radiological features. Osseous sarcoidosis may present with lytic, sclerotic, or mixed lesions that can closely resemble metastatic disease, infection, or other inflammatory conditions, frequently leading to diagnostic delay.
Sacroiliac joint involvement is particularly rare, with an estimated prevalence of about 6% among patients with sarcoidosis. When present, sacroiliac sarcoidosis may clinically and radiologically mimic ankylosing spondylitis, tuberculosis, or neoplastic disease, making differential diagnosis challenging. Imaging modalities such as MRI are helpful for detecting inflammatory and infiltrative lesions, but findings are not specific, and histological confirmation is often required to establish the diagnosis.
Muscle sarcoidosis is usually asymptomatic and frequently discovered incidentally, although symptomatic forms such as chronic myopathy or pseudo-tumoral myositis have been described. The pseudo-tumoral form is exceptionally rare and may simulate soft tissue tumors on imaging, further complicating diagnosis [2-3].
Herein, we present a rare case of musculoskeletal sarcoidosis with concomitant sacroiliac involvement, diffuse osseous lesions, and pseudo-tumoral muscular involvement, highlighting the diagnostic challenges and the importance of histopathological confirmation.
Case presentation
A 47-year-old man with no prior medical history presented with a six-month history of progressive bilateral sacroiliac and shoulder pain. Initial symptoms included fever, chills, and weight loss, which resolved spontaneously within two weeks, leaving persistent articular pain. The patient subsequently developed transient cervical and inguinal lymphadenopathy.
Pelvic MRI revealed bilateral sacroiliac arthritis with diffuse bone marrow signal abnormalities involving the pelvic girdle and femoral heads, hyperintense on short tau inversion recovery (STIR) sequences with preserved cortical integrity. A poorly defined lobulated lesion of the left iliopsoas muscle (53 mm) was also detected (Figure 1).
Pelvic MRIPelvic MRI (coronal STIR sequence) showing bilateral sacroiliac arthritis with diffuse bone marrow hyperintensity involving the pelvic girdle and femoral heads. Cortical integrity is preserved.STIR - short tau inversion recovery
Chest and abdominal CT identified a lytic lesion of the left humeral head (15×11 mm) with cortical rupture and sclerotic changes in vertebral bodies (Figure 2).
CT of the chest and shoulder demonstrating a 15×11 mm lytic lesion in the left humeral head with cortical ruptureA: coronal CT scan showing a bone lesion in the upper thoracic region compatible with granulomatous involvement.B: axial CT scan demonstrating a lytic mass of the right scapula corresponding to osseous sarcoidosis involvement.
Laboratory tests showed leukopenia (3600/mm³), lymphopenia, and elevated C-reactive protein (99 mg/dL). Angiotensin-converting enzyme (ACE) was elevated (64.6 U/L), and 24-hour urine calcium was increased. Tests for human leukocyte antigen B27 (HLA-B27), HIV, hepatitis viruses, Brucella, Chlamydia, Coxiella, and tuberculosis were negative.
Bone marrow biopsy and CT-guided biopsy of the iliopsoas lesion revealed non-caseating epithelioid granulomas with Langhans-type giant cells, confirming sarcoidosis (Figure 3).
Histological examination of bone biopsyHistological examination of bone biopsy showing non-caseating granulomas composed of epithelioid cells, Langhans-type giant cells, and lymphocytes, without caseous necrosis (H&E staining, ×200).
The patient was started on oral prednisone (1 mg/kg/day) with rapid clinical improvement and significant reduction of pain. A tapering regimen was initiated, with outpatient follow-up scheduled.
Discussion
Musculoskeletal involvement in sarcoidosis is uncommon but clinically significant. Osseous lesions are reported in 1-15% of cases, often mimicking metastases or infections. Sacroiliac joint disease is particularly rare and has been described in only a limited number of case reports [4-6]. Histological confirmation is essential to distinguish sarcoidosis from tuberculosis or ankylosing spondylitis. Muscle sarcoidosis is usually asymptomatic, though up to 80% of patients show subclinical involvement. Pseudotumoral myositis, as in our case, is the rarest form (~3%) [7-8]. Imaging is useful for lesion detection but nonspecific; biopsy remains the gold standard for diagnosis. Corticosteroids remain the first-line therapy, typically 0.5-1 mg/kg/day with tapering. Methotrexate, azathioprine, or biologic agents targeting tumor necrosis factor alpha (TNF-α)are reserved for refractory cases. Our patient responded well to prednisone, consistent with reported outcomes [9-10].
Conclusions
Sacroiliac sarcoidosis is a rare manifestation that may mimic inflammatory or malignant bone disease. MRI is crucial for detecting multifocal osseous and muscular lesions, but definitive diagnosis requires histological evidence of non-caseating granulomas. Corticosteroid therapy remains the mainstay of treatment. Early recognition is essential to avoid misdiagnosis and inappropriate therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sarcoidosis N Engl J Med Iannuzzi MC Rybicki BA Teirstein AS 2153216535720071803276510.1056/NEJ Mra 071714 · doi ↗ · pubmed ↗
- 2ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis Statement Committee. American Thoracic Society. European Respiratory Society. World Association for Sarcoidosis and Other Granulomatous Disorders Eur Respir J Costabel U Hunninghake GW 7357371419991057321310.1034/j.1399-3003.1999.14d 02.x · doi ↗ · pubmed ↗
- 3Prevalence and clinical picture of musculoskeletal sarcoidosis Iran Red Crescent Med J Salari M Rezaieyazdi Z 0162014 https://pmc.ncbi.nlm.nih.gov/articles/PMC 4166103/10.5812/ircmj.17918 PMC 416610325237584 · doi ↗ · pubmed ↗
- 4Sacroiliitis in sarcoidosis: case reports and review of the literature Clin Rheumatol Kotter I Durk H Saal JG 695700141995860869110.1007/BF 02207939 · doi ↗ · pubmed ↗
- 5An assessment of back pain and the prevalence of sacroiliitis in sarcoidosis Chest Erb N Cushley MJ Kassimos DG Shave RM Kitas GD 19219612720051565398310.1378/chest.127.1.192 · doi ↗ · pubmed ↗
- 6Osseous sarcoidosis of the hand: pathologic analysis and review of the literature J Hand Surg Am Ugwonali OF Parisien M Nickerson KG Scully B Ristic S Strauch RJ 8548583020051603938410.1016/j.jhsa.2005.03.004 · doi ↗ · pubmed ↗
- 7Vertebral sarcoidosis: clinical and imaging findings Semin Arthritis Rheum Rúa-Figueroa I Gantes MA Erausquin C Mhaidli H Montesdeoca A 3463523120021196559810.1053/sarh.2002.31553 · doi ↗ · pubmed ↗
- 8Muscle involvement in sarcoidosis: a retrospective and followup studies J Rheumatol Fayad F LiotéF Berenbaum F Orcel P Bardin T 98103332006 https://pubmed.ncbi.nlm.nih.gov/16395757/16395757 · pubmed ↗