Neoplastic risk in hyperplastic esophagogastric junction lesions: Comprehensive multicenter study
Elena De Cristofaro, Federico Barbaro, Jérôme Rivory, Alexandru Lupu, Benedetto Neri, Dario Biasutto, Gianluca Andrisani, Rui Morais, Franscisco Mendes, João Santos-Antunes, Germana de Nucci, Sandro Sferrazza, Silvia Pecere, Yanis Dahel, Jean-Philippe Ratone, Laura Rovedatti

TL;DR
This study finds that some esophagogastric junction lesions, previously thought benign, have a significant risk of becoming cancerous, emphasizing the need for careful endoscopic evaluation.
Contribution
The study identifies specific endoscopic features that predict neoplastic transformation in hyperplastic esophagogastric junction lesions.
Findings
Non-polypoid morphology, surface ulceration, and lesion size >12 mm are significant predictors of neoplastic transformation.
23% of hyperplastic esophagogastric junction lesions showed neoplastic transformation upon histological analysis.
Accurate endoscopic assessment is crucial for identifying malignancy risk in these lesions.
Abstract
Esophagogastric junction (EGJ) lesions are uncommon and histologically diverse. Among these, EGJ hyperplastic lesions are rare and generally considered benign. However, their nonspecific appearance makes accurate endoscopic identification challenging. Endoscopic resection is both a diagnostic and therapeutic approach, yet risk factors for neoplastic transformation in EGJ lesions remain unclear. This study aimed to identify predictive factors for neoplastic transformation in hyperplastic EGJ lesions. This multicenter, retrospective study included patients with hyperplastic EGJ lesions endoscopically resected across 13 European hospitals. Data were collected from endoscopy and pathology reports. Neoplastic transformation was defined by presence of dysplasia or adenocarcinoma. A multivariable logistic regression model was conducted to assess predictive factors for neoplastic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
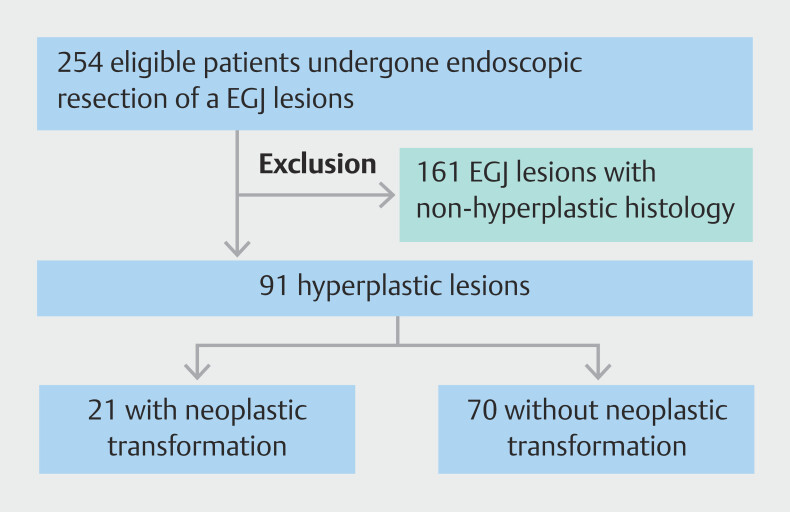 Fig. 1
Fig. 1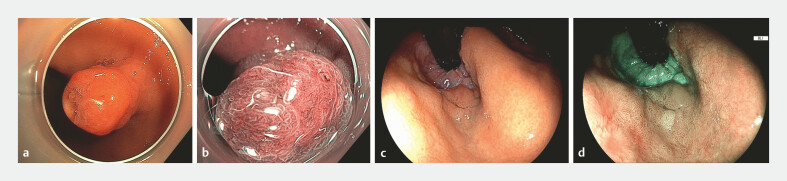 Fig. 2
Fig. 2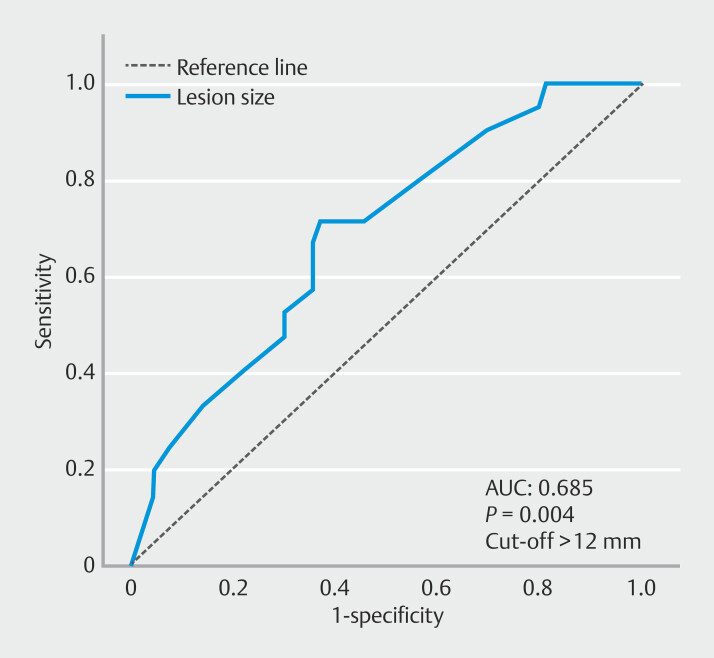 Fig. 3
Fig. 3|
| |
| IQR, interquartile range. | |
| Age at endoscopy; Median (IQR, range) | 72 (21.0; 20–97) |
| Sex, n (%) | |
Male | 45(47) |
Female | 48 (53) |
| Barrett’s esophagus, n (%) | |
Yes | 7 (8) |
No | 83 (91) |
Missing data | 1 (1) |
| History of esophageal reflux disease | |
Yes | 28 (31) |
No | 48 (53) |
Missing data | 15 (16) |
| Helicobacter pylori infection, n (%) | |
Yes | 4 (4) |
No | 66 (73) |
Missing data | 21 (23) |
| Polyp size | |
Median IQR, (range) | 10 (12.0; 3–60) |
< 25 mm, n (%) | 76 (83.5) |
≥ 25 mm, n (%) | 15 (16.5) |
| Location, n (%) | |
Greater curvature, anterior wall | 21 (23) |
Greater curvature, posterior wall | 22 (24) |
Lesser curvature, anterior wall | 11 (12) |
Lesser curvature, posterior wall | 11 (12) |
Missing data | 26 (29) |
| Morphology, Paris Classification n (%) | |
0-Is | 51 (56) |
0-Isp/0-Ip | 20 (22) |
0-IIa | 10 (11) |
0-IIb | 2 (2) |
0-IIc | 2 (2) |
Missing data | 6 (7) |
| Pit Pattern, n (%) | |
Regular | 72 (79) |
Irregular | 6 (7) |
Missing data | 13 (14) |
| Presence of surface ulceration, n (%) | |
Yes | 19 (21) |
No | 61 (67) |
Missing data | 11 (12) |
| Type of resection, n (%) | |
EMR/polypectomy | 78 (86) |
ESD | 17 (19) |
Others [cap-mucosectomy) | 3 (3) |
| En bloc resection, n (%) | |
Yes | 85 (93) |
No | 6 (7) |
| Complications, n (%) | |
Bleeding | 11 (12) |
Stenosis | 1 (0.8) |
| Quality of resection, n (%) | |
R0 | 76 (84) |
R1 | 15 (16) |
|
|
| |||
|
|
|
|
| |
| OR, odds ratio. | ||||
| Greater curvature location | 1.66 (0.55–5.02) | 0.37 | ||
| Size, median (range) | 1.04 (1.01–1.09) |
| 5.48 (1.01–1.11) |
|
| Non polypoid morphology | 3.81 (1.18–12.3) |
| 5.48 (1.29–23.2) |
|
| Irregular pit pattern | 3.23 (0.59 17.5) | 0.18 | ||
| Irregular vascular pattern | 1.96 (0.31–12.7) | 0.49 | ||
| Presence of ulcerate surface | 5.05 (1.67–15.3) |
| 11.5 (2.88–45.8) |
|
| Barrett’s esophagus | 1.12 (0.2 – 6.05) | 0.89 | ||
| 054 (0.05–4.98) | 0.57 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Gastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment
Introduction
Esophagogastric junction (EGJ) lesions represent a distinct and uncommon subset of gastrointestinal lesions, encompassing a heterogeneous group of histopathologic entities. These include adenoma, squamous papilloma, leiomyoma, Barrett's esophagus (BE)-associated polypoid dysplasia, polypoid carcinoma, inflammatory fibroid polyps, and fundic gland polyps 1 2 3 . Hyperplastic lesions of the EGJ are another rare type of polyp, characterized by proliferation of gastric-type foveolar epithelium, squamous epithelium, or both 4 5 .
The first systematic analysis of hyperplastic EGJ polyps was conducted in the early 2000s by Abraham et al. 6 , who reported that these lesions were most often located at the EGJ (67%), followed by the distal esophagus (30%). Most polyps (80%) were predominantly composed of cardiac-type mucosa, with a smaller proportion consisting of squamous mucosa (17%) or a mixture of both (3%). Intestinal metaplasia and low-grade dysplasia were rare, observed in 7% and 3% of cases, respectively. However, this study analyzed only 30 hyperplastic polyps from 27 patients and did not fully elucidate endoscopic features of EGJ lesions.
Differentiating hyperplastic polyps of the EGJ from other lesions in this region remains challenging, due to their nonspecific macroscopic appearance and limited understanding of their neoplastic potential 7 8 9 . Although some studies suggest a potential association with BE and gastroesophageal reflux disease (GERD) 5 10 11 , the evidence is conflicting. In addition, unlike other gastric locations, the relationship between EGJ hyperplastic lesions and Helicobacter pylori infection remains unclear 6 12 . Overall, prevalence of dysplasia arising in hyperplastic lesions remains debated, with reported rates ranging from 1.9% to 19% 13 14 15 16 17 . Similarly, risk of adenocarcinoma has been documented in larger studies, varying from 0% to 13.5% 13 15 16 18 19 20 . This wide variability complicates clinical decision-making regarding need for resection and long-term surveillance. Moreover, limited data are available specifically on EGJ lesions and their potential risk of malignant transformation. Understanding the neoplastic potential of these lesions is crucial for guiding endoscopic management and surveillance strategies. This study aimed to assess risk of neoplastic transformation in hyperplastic EGJ lesions.
Patients and methods
Study group
This retrospective multicenter study investigated EGJ hyperplastic lesions across 13 European hospitals, including three centers in France, one in Portugal, one in Belgium, and eight in Italy, between January 2015 and October 2024. Patients were identified retrospectively using disease coding systems or prospectively maintained databases at each center. Relevant clinical data were extracted from endoscopy, pathology, and hospitalization reports and anonymized prior to analysis.
Inclusion criteria comprised patients aged ≥ 18 years who underwent endoscopic resection of a hyperplastic lesion located at the EGJ. Exclusion criteria included lesions recurring at the site of a previous endoscopic resection, non-hyperplastic lesions, hyperplastic lesions not resected, and patients with hereditary gastric polyposis syndromes (e.g., familial adenomatous polyposis or hamartomatous polyposis). Additional clinical variables were recorded, including presence of BE, history of GERD—defined as presence of typical symptoms such as heartburn and/or regurgitation at least twice per week 21 —and Helicobacter pylori infection. Endoscopic follow-up data were collected when available. Lesions were classified according to the Paris classification 22 23 as polypoid (sessile 0-Is, pedunculated 0-Ip, or semi-pedunculated 0-Isp) or non-polypoid (slightly elevated 0-IIa, flat 0-IIb, or slightly depressed 0-IIc). Anatomical location was further categorized into greater or lesser curvature and anterior or posterior wall. Vascular and pit patterns were described as regular or irregular and presence of surface ulceration was noted.
Resection technique was categorized as endoscopic mucosal resection (EMR)/polypectomy, endoscopic submucosal dissection [ESD]), or other. Immediate and delayed adverse events, such as bleeding, perforation, or stenosis, were identified retrospectively from medical records and classified according to the Adverse events in GastRointEstinal Endoscopy (AGREE) system 24 .
Definitions
EGJ lesions were defined as suspected hyperplastic lesions located within 2 cm above or below the endoscopic EGJ. Histologically, they were classified as hyperplastic polyps based on presence of elongated, tortuous, and dilated foveolar glands lined by mucin-rich epithelium, often associated with surface erosions and a chronically inflamed lamina propria. En bloc resection was defined as complete removal of the lesion in a single piece without fragmentation. R0 resection was defined as en bloc resection with tumor-free horizontal and vertical margins. Neoplastic transformation was defined by histological presence of dysplasia or adenocarcinoma arising within a hyperplastic EGJ lesion 25 .
Objectives
The primary objective was to identify independent predictive factors associated with neoplastic transformation in EGJ hyperplastic lesions that underwent endoscopic resection.
Secondary objectives included assessment of recurrence rates following endoscopic resection and evaluation of en bloc and R0 resection rates according to the technique used.
Statistical analysis
Quantitative variables were described using the mean and standard deviation or the median with the range and interquartile range (IQR). Qualitative variables were summarized by frequency and percentage, excluding missing data from percentage calculations. The effect of various factors on risk of neoplastic transformation was quantified using odds ratios (ORs) with corresponding 95% confidence intervals (CIs). Group comparisons were conducted using Student’s t -test, chi-squared test, or Mann-Whitney U test (Wilcoxon rank-sum test), depending on data distribution.
Univariable analyses were performed using mixed logistic regressions to explore associations between potential risk factors and neoplastic transformation. Variables with P < 0.01 in univariable analysis were then included in a multivariable logistic regression model, followed by a backward selection process to identify the most significant predictors. P < 0.05 was considered statistically significant. The receiver operating characteristic (ROC) curve was plotted to determine the optimal cut-off point for lesion size as a predictor of neoplastic transformation. Statistical analyses were performed on all available data (SPSS 29.0).
Ethical considerations
The study was conducted according to the Declaration of Helsinki and received approval from the ethics committee of the Policlinico Tor Vergata (Rome), February 28, 2024, code 15.24 CET2 ptv.
Results
Study populations and outcomes
Between January 2015 and October 2024, a total of 254 endoscopically resected EGJ lesions were recorded. After excluding non-hyperplastic lesions, 91 EGJ hyperplastic lesions were included in the study ( Fig. 1 ). The clinical and endoscopic characteristics of cohort are presented in Table 1 .
Flowchart of the study.
: Table 1 Clinical and endoscopic characteristics of full cohort (91 patients).
The cohort predominantly consisted of elderly patients (72 years; IQR 21.0), with a slight male predominance (47%). A minority had a history of GERD (31%) or BE (8%). Helicobacter pylori status was available for 70 out of 91 patients, with four positive cases (6%).
Median lesion size was 10 mm (IQR 12.0; range: 3–60 mm). Seventy-seven of 91 lesions (85%) were classified as polypoid, whereas 14 lesions (15%) were non-polypoid according to the Paris classification. Vascular and pit patterns were described as regular in 71 (78%) and 72 (79%) lesions, respectively. Surface ulceration was observed in 19 cases (21%).
Of 91 evaluable lesions, 78 (86%) were resected using conventional EMR, 17 (19%) with ESD, and three (3%) with cap-assisted EMR. En bloc resection was achieved in 85 cases (93%) and R0 resection was confirmed in 76 lesions (84%), including 60 of 78 (77%) after EMR and 16 of 17 (94%) after ESD. Immediate post-procedure bleeding occurred in 11 cases (12%) and was managed endoscopically. One patient developed a stricture after resection of a large (45 mm), nearly circumferential lesion.
Recurrence after endoscopic resection
Among the 91 patients, 38 (42%) underwent at least one endoscopic follow-up, with the first control endoscopy performed after a median interval of 7 months. During follow-up, 10 of 38 patients (26%) presented with recurrence of hyperplastic lesions. Notably, eight of 10 recurrences occurred in lesions initially resected using EMR, whereas two recurrences were observed in lesions resected by ESD, despite histologically confirmed R0 resection. All recurrent lesions were successfully managed with repeat endoscopic resection.
Predictive factors of neoplastic transformation in hyperplastic lesions
Histological examination revealed that 21 of 91 hyperplastic lesions (23%) exhibited neoplastic transformation. Among these, seven were classified as low-grade dysplasia, two as high-grade dysplasia, and 12 as adenocarcinoma (including 10 intramucosal and 2 with submucosal invasion). An example of a malignant hyperplastic lesion is presented in Fig. 2 . Median lesion size was 14 mm (IQR 28; 12–40) for dysplastic lesions and 10 mm (IQR 10 mm; 8–18) for adenocarcinomas. Surface ulceration was present in one of nine (11%) dysplastic lesions and nine of 12 (75%) were adenocarcinomas.
Representative examples of hyperplastic lesions of the esophagogastric junction. a Malignant hyperplastic lesion showing a distinct neoplastic component under white light imaging. b The same lesion observed in close-up view with dual focus and narrow-band imaging, demonstrating irregular microsurface and microvascular patterns consistent with neoplastic transformation. c Non-dysplastic hyperplastic polyp of the esophagogastric junction, visualized in retroflexed view under white light. d The same lesion examined with blue light imaging (BLI).
Univariable analysis identified surface ulceration (OR 5.05, 95% CI 1.67–15.35; p = 0.004), non-polypoid morphology (OR 3.81, 95% CI 1.18–12.27; P = 0.027), and lesion size (OR 1.04, 95% CI 1.01–1.09; p = 0.033) as significant risk factors for neoplastic transformation.
These associations were confirmed in multivariable analysis, which demonstrated that surface ulceration (OR 11.5, 95% CI 2.88–45.78; P = 0.0005), non-polypoid morphology (OR 5.48, 95% CI 1.29–23.19; P = 0.025), and lesion size (OR 1.06, 95% CI 1.01–1.11; P = 0.021) were independent predictors of dysplasia ( Table 2 ).
: Table 2 Univariable and multivariable analysis to identify factors predictive of neoplastic transformation in hyperplastic esophagogastric junction lesions.
The predictive value of lesion size for neoplastic transformation, including dysplastic lesions and adenocarcinomas, was further evaluated using ROC curve analysis. The area under the ROC curve was 0.685 (95% CI: 0.561–0.809; P = 0.004). The optimal cut-off value was 12 mm, yielding a sensitivity of 71% and a specificity of 63% ( Fig. 3 ).
Receiver operating curve for neoplastic transformation based on the lesion size.
Discussion
This multicenter study evaluated risk of neoplastic transformation in EGJ hyperplastic lesions, a condition traditionally considered rare and benign 26 , and therefore, often left unresected. However, the mechanisms underlying potential malignant transformation and the associated risk factors remain poorly defined. The previous analysis, conducted by Abraham et al. 6 , included a limited cohort of 30 polyps from 27 patients and did not provide a comprehensive characterization of EGJ lesions, particularly regarding their endoscopic features and neoplastic potential.
In our study, 23% of resected hyperplastic EGJ lesions showed neoplastic transformation (i.e., dysplasia or adenocarcinoma), reinforcing the hypothesis that these lesions may undergo chronic irritation and regenerative proliferation, contributing to dysplastic progression 27 .
Consistent with earlier reports 6 26 28 29 , we identified three independent predictors of neoplastic transformation: non-polypoid morphology, surface ulceration, and lesion size. Notably, non-polypoid lesions were associated with substantially increased risk, mirroring findings from gastric and colorectal literature where flat or depressed lesions are more likely to harbor high-grade dysplasia or carcinoma. Surface ulceration also emerged as a significant predictor, highlighting the importance of meticulous endoscopic inspection, because ulceration may reflect more aggressive biological behavior.
Although the association between lesion size and neoplastic transformation has been previously reported 30 31 , with rates rising from 5.2% in all gastric hyperplastic polyps to 8.3% in those > 10 mm, these studies considered the entire stomach. Our study specifically addresses the EGJ, a region for which evidence remains scarce. Interestingly, GERD, BE, and H. pylori infection did not appear to influence neoplastic transformation in EGJ hyperplastic lesions, contrasting with what is observed in other gastric regions.
In our study, the rate of neoplastic transformation was higher than previously reported in studies that included hyperplastic lesions from the entire stomach 13 14 15 16 17 18 19 20 . This finding suggests that additional factors may contribute to development of dysplasia in the EGJ region, which presents unique characteristics such as the transition between squamous and columnar epithelium, greater exposure to gastric acid, and different patterns of H. pylori colonization. Our study provides a broader assessment of EGJ hyperplastic lesions, emphasizing their endoscopic characteristics and implications for early detection and resection. This supports existing recommendations to favor complete endoscopic resection of suspicious lesions, because biopsy alone is often inadequate to rule out neoplastic transformation 32 . In our series, follow-up was available for 42% of patients, and approximately 30% of resected lesions recurred, even after histologically confirmed R0 resection. This may support the theory that fibrosis and scarring contribute to new hyperplastic growth, as previously described 27 . These findings highlight the need for ongoing surveillance, even in apparently completely resected lesions.
Despite the strengths of its multicenter design and the relatively large sample size for such a specific topic, this study has several limitations. The retrospective design introduces potential selection bias, although most centers used prospectively maintained databases. A major inherent bias lies in inclusion of only lesions that underwent endoscopic resection, which were, therefore, likely considered suspicious by the endoscopist. However, biopsy alone may not provide a comprehensive assessment of dysplastic risk in EGJ hyperplastic lesions, given their potential histological heterogeneity. In addition, the macroscopic endoscopic features of these lesions are not yet clearly defined, making reliable risk characterization difficult. The other limitation is that follow-up was not standardized, and long-term outcomes were not uniformly available, limiting assessment of recurrence and progression. Furthermore, histopathological evaluation was not centralized and detailed pathological parameters were not always recorded, including information on the epithelial origin of the neoplastic proliferation (squamous versus gastric-type), thus precluding comparative analysis.
Conclusions
In conclusion, although this retrospective multicenter study included a selected population, our findings indicate that hyperplastic lesions of the EGJ may harbor neoplastic potential, particularly when they present with suspicious endoscopic features. In such cases, especially for lesions ≥ 12 mm, ulcerated, or non-polypoid, endoscopic resection should be considered, ideally with en bloc removal to ensure complete histological assessment. Careful endoscopic evaluation and appropriate management strategies are warranted. Further prospective studies are needed to confirm the neoplastic transformation rate, validate predictive criteria, and determine whether systematic R0 resection should be recommended to reduce risk of missing neoplastic changes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bosch O González Campos CJ Esophageal inflammatory fibroid polyp - Endoscopic and radiologic features Dig Dis Sci 199439256125667995180 10.1007/BF 02087691 · doi ↗ · pubmed ↗
- 2Carmack SW Genta RM Schuler CM The current spectrum of gastric polyps: A 1-year national study of over 120,000 patients Am J Gastroenterol 20091041524153210.1038/ajg.2009.13919491866 · doi ↗ · pubmed ↗
- 3Adorisio O Ceriati E Camassei FD Inflammatory fibroid polyp of the esophagogastric junction J Pediatr Gastroenterol Nutr 201764 e 15410.1097/MPG.000000000000097726360659 · doi ↗ · pubmed ↗
- 4Long KB Odze RD Gastroesophageal junction hyperplastic [inflammatory) polyps: A clinical and pathologic study of 46 cases Am J Surg Pathol 2011351038104410.1097/PAS.0b 013e 318218942521606824 · doi ↗ · pubmed ↗
- 5Kim A Park WY Shin N Cardiac mucosa at the gastroesophageal junction: An Eastern perspective World J Gastroenterol 2015219126913310.3748/wjg.v 21.i 30.912626290639 PMC 4533044 · doi ↗ · pubmed ↗
- 6Abraham SC Singh VK Yardley JH Hyperplastic polyps of the esophagus and esophagogastric junction: Histologic and clinicopathologic findings Am J Surg Pathol 2001251180118710.1097/00000478-200109000-0000911688578 · doi ↗ · pubmed ↗
- 7Murney RG Huston JD Endoscopic evaluation of the esophagogastric polyp and fold Gastrointest Endosc 19832929429610.1016/s 0016-5107(83)72636-26642160 · doi ↗ · pubmed ↗
- 8Melton SD Genta RM Gastric cardiac polyps: a clinicopathologic study of 330 cases Am J Surg Pathol 2010341792179710.1097/PAS.0b 013e 3181 fc 714d 21107084 · doi ↗ · pubmed ↗