Automated 3D Quantitative Analysis of Intrapulmonary Vessel Volume on Non-contrast CT in Healthy Individuals
Ying Ming, Yu Zhang, Ran Xiao, Ruijie Zhao, Jiaru Wang, Sirong Piao, Lan Song, Yinghao Xu, Xin Sui, Wei Song

TL;DR
This study shows that automated 3D analysis of lung vessel volume in healthy people varies depending on the CT scan window used.
Contribution
The study introduces an automated method for 3D quantitative analysis of intrapulmonary vessel volume using non-contrast CT scans.
Findings
IPVV values from the lung window were significantly higher than those from the mediastinal window.
Sex-based differences in IPVV were observed in specific vessel diameter ranges.
Automated IPVV extraction proved feasible for identifying vessel morphological characteristics.
Abstract
This study aimed to compare automated three-dimensional Intrapulmonary Vessel Volume (IPVV) differences between lung and mediastinal windows in healthy individuals using quantitative measurements obtained from chest Computed Tomography (CT) plain scans. A total of 258 participants (aged 21–83 years) with negative chest CT scans from routine physical examinations conducted between January to November 2023 were retrospectively enrolled. For each healthy participant, an algorithm was used to automatically extract total lung IPVVs as well as IPVVs for vessels of specific diameter. Differences in IPVVs were then compared between those extracted using the lung window and those extracted using the mediastinal window. The IPVVs for the entire lung, intrapulmonary arteries, intrapulmonary veins, and small pulmonary vessels (categorized by different diameters) extracted from the lung window…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
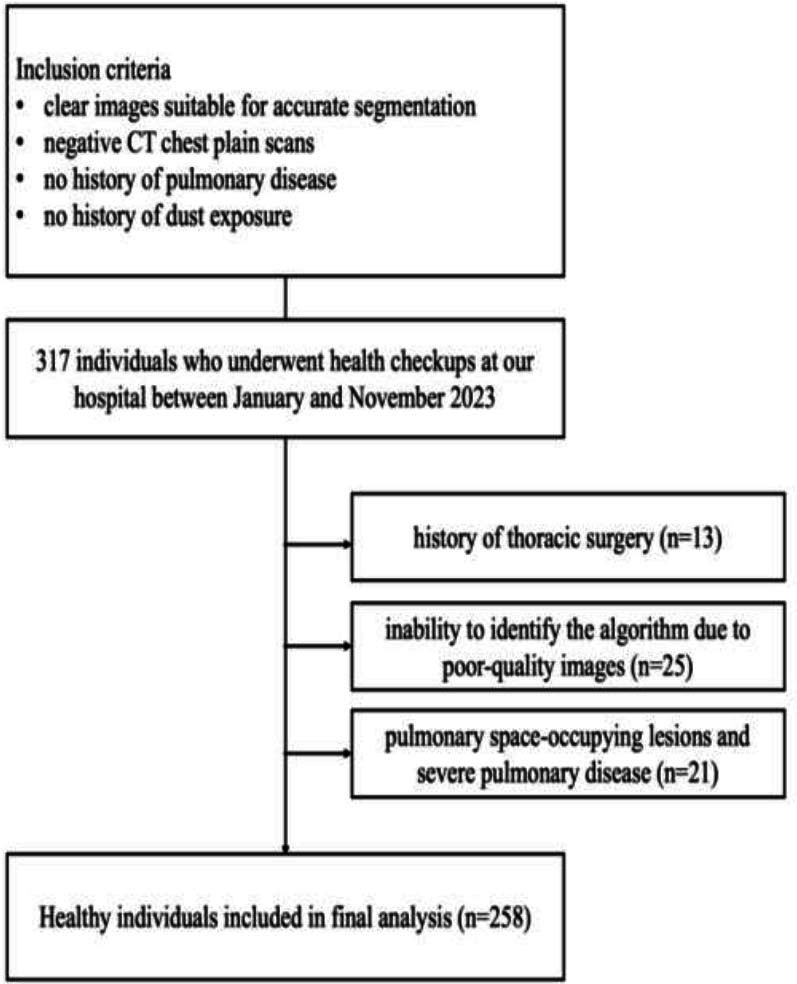 Figure 1
Figure 1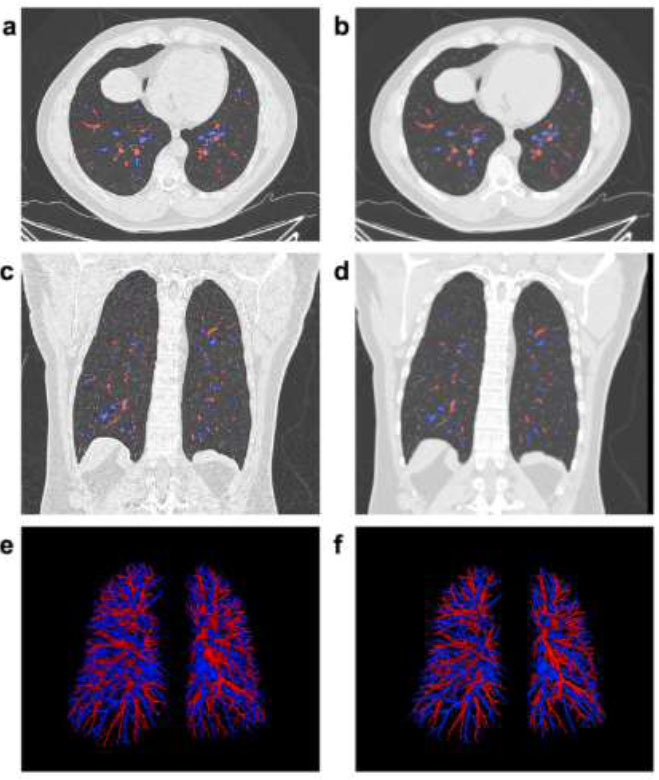 Figure 2
Figure 2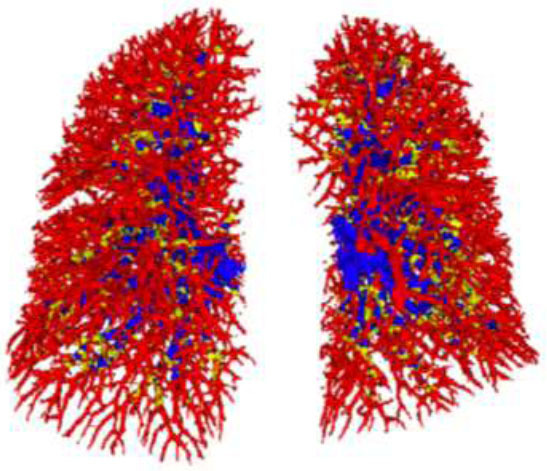 Figure 3
Figure 3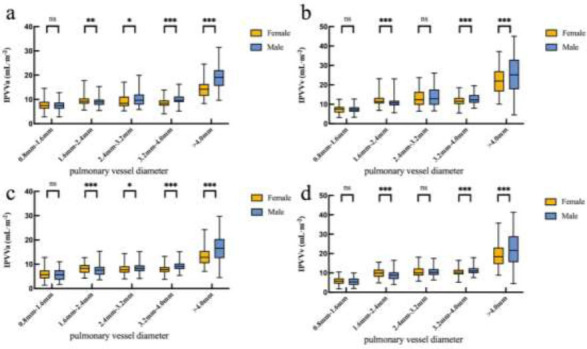 Figure 4
Figure 4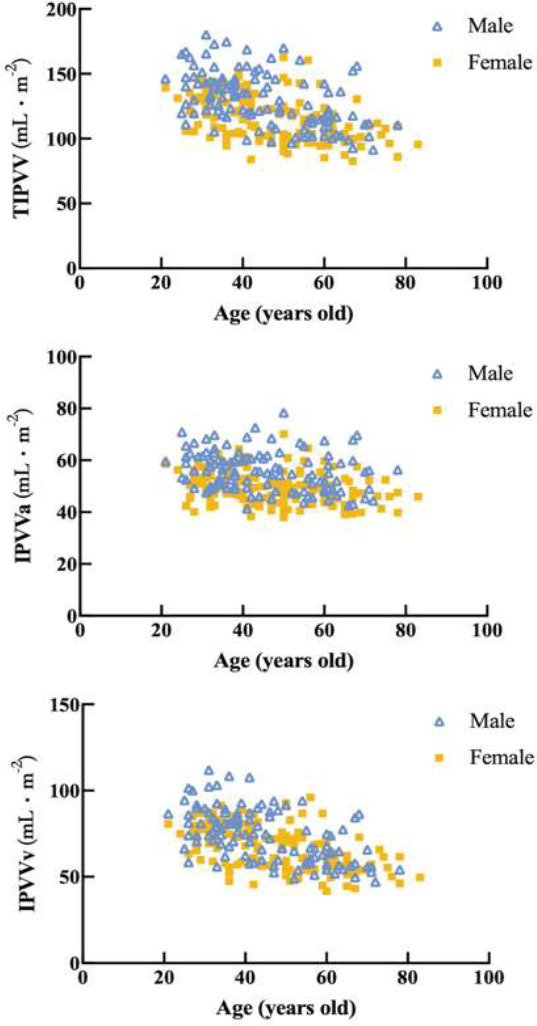 Figure 5
Figure 5- —China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPulmonary Hypertension Research and Treatments · Congenital Heart Disease Studies · Vascular anomalies and interventions
INTRODUCTION
1
Studying pulmonary vasculature morphology in healthy individuals is essential for understanding the complex network underpinning pulmonary functions [1]. Diseases that cause abnormal vascularization in the lungs impact both cardiac and pulmonary function. Pulmonary vasculature injury and reductions in pulmonary vessel volume can impair cardiac filling [2]. Existing studies on normal values for pulmonary vessel size and number have largely relied on autopsy findings, which have inherent limitations [3-5]. Consequently, there is a pressing need for more objective, non-invasive, and accurate methods to assess Intrapulmonary Vascular Volume (IPVV).
Computed Tomography (CT) is the most commonly used imaging modality for diagnosing and evaluating pulmonary diseases [6, 7]. CT scans can visualize small pulmonary vessels, assessing features, such as dilatation, tortuosity, and tapering in vessels that are only 1 mm in diameter [8, 9]. Sato et al. [10] and Frangi et al. [11] showed that pulmonary vessels have tube-like structures, and substantial research has focused on extracting and analyzing pulmonary vascular morphology. Numerous studies have proposed methods for segmenting pulmonary vessels in chest CT images [12]. However, arteries and veins are rarely analyzed separately because of technical limitations [13]. Identifying pulmonary arteries and veins remains challenging due to the high number of vessels, making manual labeling time-intensive and difficult to standardize. Computational algorithms, however, can independently identify intrapulmonary vessels from chest CT images and interpret related morphological information [7, 14], facilitating accurate identification and measurement of individual vascular segments.
Extracting and analyzing pulmonary vessels could aid in the non-invasive diagnosis of lung diseases and may be valuable for accessing, diagnosing, and predicting outcomes in patients with a history of smoking [15], pulmonary hypertension [13, 16, 17], Chronic Obstructive Pulmonary Disease (COPD) [18, 19], and/or Coronavirus Disease 2019 (COVID-19) [20, 21]. To date, however, no studies have examined potential discrepancies in quantitatively extracted IPVVs derived from either lung or mediastinal CT windows in healthy participants. Most previous studies have used the mediastinal window to measure vessel diameters [22].
In this study, we aimed to automatically extract IPVVs using a new post-processing method to separately analyze pulmonary arteries and veins and investigate differences in IPVV derived from lung and mediastinal windows in vivo. This non-invasive and quantitative evaluation tool may facilitate further research.
MATERIALS AND METHODS
2
Participants
2.1
This retrospective study, approved by the ethics committee and the institutional review board (no. I-23PJ2181), was granted an exemption from informed consent. A total of 317 individuals who underwent non-contrast chest Computed Tomography (CT) at our hospital between January and November 2023 were retrospectively enrolled.
The inclusion criteria were as follows: (1) clear images suitable for accurate segmentation, (2) negative CT chest plain scans, (3) no history of pulmonary disease, and (4) no history of dust exposure. Exclusion criteria included (1) a history of thoracic surgery, (2) inability to identify the algorithm due to poor-quality images, (3) pulmonary space-occupying lesions and severe pulmonary disease, including consolidations, pulmonary nodules, severe emphysema, and severe interstitial pneumonia, which could impact results, and (4) thoracic deformity.
Clinical metrics, including the height (cm) and weight (kg) of the participants, were collected from electronic medical records. All images were saved in Digital Imaging and Communications in Medicine (DICOM) format. Fig. (1) shows the flow diagram of the included individuals.
EXPERIMENTAL
3
CT Image Acquisition
3.1
All individuals underwent whole-lung volume CT scans. Non-contrast chest CT scans were performed using the IQon CT (Philips Medical Systems, Best, Netherlands) and Aquilion ONE GENESIS (Toshiba Medical Systems, Tokyo, Japan). Participants were instructed to hold their breath before the CT scan and during the examination and take on a supine position, supporting their heads with both arms. Breath-holding was performed at the end of deep inspiration, while whole-lung scans were performed from the pulmonary apex to the lung base. CT scan parameters were as follows: tube voltage, 120 kVp; tube current, automatic tube current modulation technology; rotation time, 0.5 s; image matrix, 512×512; collimation, 64×0.625 mm (IQon CT), 80×0.5 mm (Aquilion ONE GENESIS); field of view, < 410 mm. Instead of using complex iterative algorithms for noise reduction, the images were reconstructed using deep learning reconstruction (Advanced Intelligent Clear-IQ Engine, AiCE).
Quantitative Evaluation of Pulmonary Vessels
3.2
All image files in DICOM format were transferred to a separate post-processing workstation. An algorithm (Canon Medical Systems, Tokyo, Japan) automatically extracted and segmented pulmonary vessels with high repeatability. This process involved utilizing a pulmonary artery/vein separation algorithm to categorize voxels into three classes: background, pulmonary arteries, and pulmonary veins.
Firstly, the input CT images underwent preprocessing, including cropping, normalization, and resampling. Cropping was conducted based on the lung mask’s bounding box, yielding smaller images. These cropped images were then resampled to a target resolution of 0.726 mm, 0.726 mm, and 0.8 mm. The intensity values of the resampled images were clipped to 0.5%–99.5% of the foreground intensity value, followed by normalization using means ± Standard Deviations (SDs) of the foreground intensity value. Secondly, with a U-Net-based model, the preprocessed images underwent inference, and a sliding window algorithm was used to handle the varying volume sizes. The full volume was divided into blocks based on patch size and neural networks predicted outputs for each block, which were then scaled using a Gaussian function and summed up within overlapping regions. Finally, post-processing algorithms refined the results. Since the model inference used a cropped volume, a rollback geometry implementation was applied to resample resolution and reinsert the cropped volume into the original volume. This operation relied on the bounding box used for volume cropping during preprocessing. A post-processing algorithm, accessed via a C interface, performed outlier removal and adjusted the vessel branch for labeling the changes.
The algorithm automatically extracted IPVV from both lung and mediastinal windows. Two radiologists (with 4 and 15 years of experience in chest CT interpretation, respectively) visually evaluated all data. After their evaluation, any identified mislabeling of arteries and veins was manually corrected. Quantitative measurements of Total Intrapulmonary Vessel Volume (TIPVV), Intrapulmonary arterial Vessel Volume (IPVVa), Intrapulmonary venous Vessel Volume (IPVVv), and IPVV of small pulmonary vessels across various diameter categories (pulmonary vessels < 0.8 mm, 0.8 mm < pulmonary vessels < 1.6 mm, 1.6 mm < pulmonary vessels < 2.4 mm, 2.4 mm < pulmonary vessels < 3.2 mm, 3.2 mm < pulmonary vessels < 4.0 mm, pulmonary vessels > 4.0 mm) were obtained. Because pulmonary artery size is known to be associated with Body Surface Area (BSA) [23], each participant’s BSA was calculated to adjust the vascular parameters using a standard formula [24].
Statistical Analysis
3.3
All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) (version 26; IBM, New York, USA), and data analysis was performed using the GraphPad Prism software (version 9.5.1; GraphPad Prism software, San Diego, USA). Data have been presented as mean ± Standard Deviations (SDs) or as medians (interquartile range), while enumeration data have been expressed as percentage. Differences in these parameters were assessed using t-tests or U-tests, depending on the outcome of the normality test. A p-value of less than 0.05 (p < 0.05) was considered statistically significant.
RESULTS
4
Participant Characteristics
4.1
Based on the inclusion and exclusion criteria, 258 healthy participants were enrolled in this study. Their baseline characteristics are summarized in Table 1. All participants underwent lung window and mediastinal window thin-slice (CT) scans. Among the participants, 116 were male (45%) and 142 were female (55%). The algorithm achieved an extraction success rate of approximately 100%.
Comparison of IPVV Extracted from Lung and Mediastinal Windows
4.2
Fig. (2) illustrates the differences in IPVV extracted from the lung and mediastinal windows in axial, coronal, and three-dimensional (3D) images, underscoring the lung window’s advantage in displaying distal pulmonary small vessels. Table 2 shows that the TIPVV, IPVVa, IPVVv, and pulmonary small vessel volumes extracted from the lung window were significantly higher than those from the mediastinal window. Fig. (3) presents 3D reconstructions of IPVV in healthy individuals, with color-coded lung segments based on different diameters. No sex-based differences were found in pulmonary arteries and veins between 0.8 mm and 1.6 mm in either window. However, females exhibited significantly higher IPVV for pulmonary vessels between 1.6 mm and 2.4 mm. There were no statistically significant sex-based differences for pulmonary veins between 2.4 mm and 3.2 mm; however, males consistently showed higher values for all remaining IPVVs (Fig. 4). Fig. (5) shows that IPVVs in both males and females decrease progressively with advancing age. Overall, our results have suggested TIPVV, IPVVa, and IPVVv to be generally greater in males than in females.
DISCUSSION
5
The distribution and diameter of small blood vessels in the lungs are indicative of pulmonary blood flow, which is essential for diagnosing intrapulmonary vascular disease. Over recent decades, CT technology has become invaluable for visualizing lung structures and quantifying pulmonary abnormalities. Modern CT scans, utilizing advanced imaging techniques, provide highly accurate representations of pulmonary anatomy, including the automated identification and extraction of pulmonary blood vessel measurements [7, 25]. CT scans also facilitate the examination of airway remodeling and changes in the pulmonary vasculature. In this study, IPVV was extracted and reconstructed from CT scans of healthy participants using both lung and mediastinal windows. The characteristics of pulmonary blood vessels with varying diameters were quantified to enhance an understanding of the morphological traits of the pulmonary vasculature. The objective of this study was to explore the potential of automated techniques in CT image analysis to evaluate IPVV and assess the impact of different window techniques on measurement outcomes. This study has provided normal value ranges for IPVV with different vascular diameters in a healthy population, aiming to identify appropriate measurement parameters. The findings have indicated that non-contrast CT scans could be utilized as a screening tool in the future, aiding in the early detection of small pulmonary vessel abnormalities in clinical diagnosis and treatment.
We have performed automatic extraction and reconstruction of all vascular structures across pulmonary tissue and quantified vessels in various lung regions. Generally, IPVV extracted from the lung window exceeded that from the mediastinal window. Together, arteries and veins accounted for approximately 50% of total pulmonary volume. No statistical differences were found between males and females in either IPVVa or IPVVv for vessels with diameters between 0.8–1.6 mm or for IPVVv for vessels with diameters of 2.4–3.2 mm. However, females showed higher average IPVVa and IPVVv than males for vessels with diameters between 1.6–2.4 mm. Conversely, the remaining IPVV was larger in males than in females, and this was consistent with prior research findings [1]. Specifically, Pienn et al. examined the number and volume of 2–10 mm pulmonary vessels during CT pulmonary angiography and demonstrated that males had more vascular segments than females across all vessel diameter ranges. This discrepancy may have likely risen from the fact that adult males generally have larger body sizes and higher cardiac output than adult females. Additionally, males possess larger pulmonary vascular trees to accommodate gas exchange, resulting in higher IPVV compared to females. Images tend to be smoother in mediastinal window reconstructions and sharper in bone-window reconstructions. Different window reconstructions facilitate varied disease diagnoses [26]. The lung window has been reported to demonstrate better specificity, precision, and sensitivity than the mediastinal window. Adjusting the window level and width has been found to improve differentiation between Ground-glass Opacities (GGOs) from bronchi and pulmonary blood vessels [27, 28]. Moreover, the lung window is more accurate than the mediastinal window for assessing tumor size and providing valuable information for predicting malignant tumors [29, 30]. This may be attributed to the default lung window settings, including a higher window width and lower window levels. The lung window enhances contrasts between pulmonary tissue and air, facilitating a clear visualization of delicate structures, like small pulmonary vessels. Conversely, the mediastinal window is better suited for observing various mediastinal structures.
Previous studies have demonstrated the percentage of small pulmonary vessels with a Cross-sectional Area (CSA) less than 5 mm^2^ as useful for assessing changes in pulmonary vasculature and determining the severity of Chronic Obstructive Pulmonary Disease (COPD) [31, 32]. Additionally, CSA measurements of small pulmonary vessels provide information on pulmonary hypertension [33], facilitating early disease detection and monitoring. Jacob et al. reported that measurements of pulmonary vessels and vessel-related structures using CT can enhance prognosis prediction in patients with Idiopathic Pulmonary Fibrosis (IPF) [34]. However, these assessments have been conducted using one-dimensional levels, introducing subjectivity and limiting comprehensive evaluations of intrapulmonary vasculature. In contrast, three-dimensional (3D) volumetry, employed in vascular systems and conditions, such as abdominal aortic aneurysms [35, 36], offers increased reliability by accurately reflecting morphological changes [37]. Furthermore, measurements of IPVV categorized by vessel size could provide critical insights into the progression of IPF. Previous studies have shown that the involvement of smaller vessels and changes in vessel morphology often serve as early indicators of disease progression in IPF, potentially reflecting early fibrotic changes. By quantifying IPVV and categorizing it by vessel size, clinicians may better stratify patients based on disease severity, monitor progression, and tailor management strategies accordingly. This study lays a foundational understanding of IPVV measurement in healthy individuals, paving the way for future research to validate these findings in patients with IPF and other interstitial lung diseases. This simple, replicable, and objective IPVV assessment method holds significant value.
Our algorithm automatically extracted IPVVs and differentiated between pulmonary arteries and veins. The results of the algorithm have been found to be objective and accurate. The segmentation and extraction methods we applied have been found to be efficient and rapid, suggesting that our algorithm could be applied and assessed in future large-sample studies. Additionally, Artificial Intelligence (AI) may provide further insights into medical imaging as it continues to evolve [38]. Despite our significant findings, this study has involved some limitations.
Firstly, as a single-center, retrospective study with a small sample size, our healthy participants may not represent the broader Chinese population. Secondly, selection bias was present and, thirdly, the size estimations for pulmonary blood vessels were limited by CT pixel size (~0.8 mm), which made it impossible to capture the pulmonary microvasculature (estimated capillary blood volume was 140 mL) [2]. However, a previous study has reported that vessels with a diameter less than 1.2 mm have a stronger correlation with survival prediction than those with a diameter less than 0.8 mm [16]. This may be because although small vessels indicate microvascular damage, they contribute little to the total vascular volume. In contrast, larger vessels tend to be more clinically relevant to functional outcomes and are more reflective of overall health. Currently, most conventional CT scanners operate with a 512 matrix, and the FOV for chest scans is typically between 350-400 mm. The algorithm used in this study can be applied to most CT scanners. In the future, with the development and widespread acceptance of 1024 matrix machines, pixel values and thresholds will be significantly reduced. This study has thus established a foundation and offered guidance for the future use of non-contrast CT scans as a potential screening tool for pulmonary vascular diseases, aiming to facilitate the early detection of pulmonary vascular abnormalities in clinical practice.
CONCLUSION
Herein, a quantitative analysis algorithm has been developed to enable the automatic extraction of IPVV from plain chest CT scans. Our findings have indicated pulmonary small vessels to be more visible in the lung window, compared to the mediastinal window, providing higher accuracy in quantifying these structures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pienn M. Burgard C. Payer C. Avian A. Urschler M. Stollberger R. Olschewski A. Olschewski H. Johnson T. Meinel F.G. Bálint Z. Healthy lung vessel morphology derived from thoracic computed tomography.Front. Physiol.2018934610.3389/fphys.2018.0034629755360 PMC 5932382 · doi ↗ · pubmed ↗
- 2Aaron C.P. Hoffman E.A. Lima J.A.C. Kawut S.M. Bertoni A.G. Vogel-Claussen J. Habibi M. Hueper K. Jacobs D.R.Jr Kalhan R. Michos E.D. Post W.S. Prince M.R. Smith B.M. Ambale-Venkatesh B. Liu C.Y. Zemrak F. Watson K.E. Budoff M. Bluemke D.A. Barr R.G. Pulmonary vascular volume, impaired left ventricular filling and dyspnea: The MESA Lung Study.P Lo S One 2017124 e 017618010.1371/journal.pone.017618028426728 PMC 5398710 · doi ↗ · pubmed ↗
- 3Huang W Yen RT Mc Laurine M Bledsoe G Morphometry of the human pulmonary vasculature.J Appl Physiol 1996815212333894153710.1152/jappl.1996.81.5.2123 · doi ↗ · pubmed ↗
- 4Horsfield K. Gordon W.I. Morphometry of pulmonary veins in man.Lung 1981159121121810.1007/BF 027139177289655 · doi ↗ · pubmed ↗
- 5Singhal S. Henderson R. Horsfield K. Harding K. Cumming G. Morphometry of the human pulmonary arterial tree.Circ. Res.197333219019710.1161/01.RES.33.2.1904727370 · doi ↗ · pubmed ↗
- 6Sluimer I. Schilham A. Prokop M. van Ginneken B. Computer analysis of computed tomography scans of the lung: A survey.IEEE Trans. Med. Imaging 200625438540510.1109/TMI.2005.86275316608056 · doi ↗ · pubmed ↗
- 7Nardelli P. Jimenez-Carretero D. Bermejo-Pelaez D. Washko G.R. Rahaghi F.N. Ledesma-Carbayo M.J. San Jose Estepar R. Pulmonary artery-vein classification in CT images using deep learning.IEEE Trans. Med. Imaging 201837112428244010.1109/TMI.2018.283338529993996 PMC 6214740 · doi ↗ · pubmed ↗
- 8Resten A. Maitre S. Musset D. CT imaging of peripheral pulmonary vessel disease.Eur. Radiol.200515102045205610.1007/s 00330-005-2740-y 15906039 · doi ↗ · pubmed ↗